
Abstract
Purpose
Prostate cancer is one of the most common cancers in men, with higher prevalence in developed countries. Nothing much is known regarding the incidence and mortality of prostate cancer in Brazilian population or among the indigenous groups in Brazil. Therefore, this study aimed to correlate prostate-specific antigen (PSA) level and age in the tribe with Macuxi ethnicity, from the jungles of Amazon (between Brazil and Venezuela).
Patients and methods
This was an epidemiological cross-sectional study aimed to find the correlation between age and PSA in the 110 Brazilian Indian tribal men of Macuxi ethnicity. Serum PSA levels (total and free PSA [tPSA and fPSA]) were screened and analyzed considering age groups.
Results
We found that there was a significant correlation between the age and either tPSA (p=0.016) or fPSA (p=0.036). Interestingly, there was no correlation between tPSA and fPSA with any of the age groups, but we found a significant correlation between fPSA and tPSA in only the age groups 60–69 years and 70–80 years (p=0.008).
Conclusion
In this study, we found a significant correlation between tPSA, fPSA, and the age of patients. However, the age-specific correlation was insignificant. From our current findings, we found that the levels of PSA may be considered as an important determinant in determining this correlation and specificity, even though more work needs to be done to verify this. Although PSA screening is a valuable research tool for male patients, the low specificity of the screening might provide false-positive results leading to overtreatment.
Introduction
Prostate cancer is one of the most common cancers in men, with greater prevalence in developed countries. The worldwide rate of mortality due to prostate cancer in 2008 was estimated to be 28.6%.Citation1 Prostate cancer usually affects older age men, those aged >50 years,Citation2 with a median age at diagnosis of 72 years.Citation3 Prostate-specific antigen (PSA) screening guidelines among different medical organizations vary widely worldwide. In addition, the evidence for PSA screening also remains highly controversial. The literature suggests that no standard of care exists for PSA screening today. There is a marked difference in the incidence of prostate cancer in different geographical areas, which point toward genetic and environmental influences as one of the risk factors.Citation4 Ethnicity, diet, aging, and genetic factors are known to play an important role in the prevalence and progression of prostate cancer.Citation5 Although there have been demographic and racial differences in incidences of prostate cancer, the epidemiological data on prostate cancer in Latin America are scant.Citation6 Interestingly, prostate cancer was once identified as the leading cause of cancer death among native American Indian men.Citation7 But as of today, data on the incidence and mortality of prostate cancer in Brazilian population or among the indigenous groups in Brazil is insufficient.Citation8 This indicates the underreporting of cases of prostate cancer in these areas, due to socioeconomic and geographical difficulties.Citation9 Therefore, this study aimed to correlate PSA and age in the tribe of Macuxi ethnicity who hail from the jungles of Amazon (between Brazil and Venezuela).
Screening for prostate cancer is conducted via digital rectal examination and PSA measurement. PSA is an important prognostic factor for prostate cancer development.Citation10,Citation11 PSA, an androgen-regulated serine protease, is produced by prostate epithelial cells.Citation12 PSA screening has significantly increased the early diagnosis and hence diminished the mortality from prostate cancer.Citation13 However, PSA screening is also known to lead to unnecessary biopsies, overdetection, and overtreatment.Citation14
Although PSA is organ specific, being produced exclusively by prostate, it is synthesized by both normal and benign prostate tissues, and hence, it is not specific for detecting any malignancy.Citation15 In addition, prostate cancer can be present in the absence of elevated PSA.Citation16 But the probability of prostate cancer detection increases with increasing total PSA (tPSA) levels.Citation17 Most of the PSA in the blood occurs in complexed form, bound to inhibitors, and about 10%–30% of it exists as free PSA (fPSA).Citation14 Therefore, in patients with high PSA levels, evaluation of free versus protein-bound PSA is definitive of an underlying prostate abnormality.Citation18 fPSA is usually associated with benign conditions, whereas bound PSA is associated with prostate malignancies. Therefore, the ratio of fPSA to tPSA has more clinical relevance in the early detection of prostate abnormality and prevents the further malignancy.Citation19 Serum PSA levels and patient age have a direct correlation, which is shown to increase with age,Citation20–Citation22 although there are some conflicting reports.Citation23 Therefore, reduction in the reference range for PSA levels for younger men will improve the sensitivity resulting in the early detection of prostate cancer.Citation24 Moreover, age-specific PSA reference ranges also improve the specificity of the PSA test by raising the PSA threshold for older men.Citation24
Patients and methods
This was an epidemiological, cross-sectional, descriptive, prospective study done on a tribe of Macuxi ethnicity who hailed from the jungles of Amazon (between Brazil and Venezuela). Indian tribes in the Brazilian Amazon jungle on the border with Venezuela were approached for this study. Men aged >40 years were recruited to participate in the study. Laboratory tests were performed and processed by our staff in the city of Boa Vista (300 km from the Indian tribe).
Serum levels of 110 adult males aged 40–80 years were assessed by the same urologist for fPSA and tPSA. Written informed consent was taken from the patients before they were enrolled for the study. The indigenous people of this region are aware of the Portuguese language, and thus signed/provided fingerprint on the consent form. The study was approved by the Universidade Federal de Roraima Ethics Committee (number: 21799613.2.0000.5302). The patients were also subgrouped on the basis of age, the 4 age groups being 40–49, 50–59, 60–69, and 70–79 years, to compare the effect of PSA on various age groups. fPSA, tPSA, and the ratio of fPSA to tPSA (relation%) were used as indicators of risk of prostate cancer in various age groups. Although prostate cancer risk is difficult to assess accurately without prostate biopsy, we inferred it here based on the literature for nonindigenous individuals.Citation25
Statistical analysis
Bivariate correlation analysis was performed using SPSS software to find Pearson’s correlation and any significant correlation between the age of all patients and fPSA, age and tPSA, and age and fPSA/tPSA. The same analysis was performed in the 4 subgroups. A P-value of >0.05 was taken as significant in all the statistical analyses preformed. We also performed a nonparametric analysis, Spearman analysis, to check any correlation. There was no adjustment for multiple analyses. There was no bias in statistical analysis since we did not perform prostatic biopsy in this population. We used the analysis results vis-à-vis literature reports about the risk of prostate cancer in patients with PSA to interpret our results on probable histological risk (based on Gleason gradation).
Results
For our study, we divided the 110 men included in the study into 4 subgroups according to age: 40–49, 50–59, 60–69, and 70–79 years. As shown in , there is an increasing trend in the median and maximum levels of PSA, with the median value of PSA as low as 0.7 in the age group of 40–49 years and the highest value of 2.0 in the age group of 70–79 years (). Similarly, the maximum value of PSA showed similar trend, with the lowest value of 2.5 in the age group of 40–49 years and the highest value of 6.5 in the age group 70–79 years (). Thus, the data point toward a trend of an increase in the PSA value with an increase in age in the groups. The prostate cancer risk according to the levels of PSA, as can be seen in , was approximately 10.1% in the age groups 40–49 and 50–59, whereas the risk increased to 17% in the age groups 60–69 and 70–79 (). The prostate cancer risk with Gleason score >7 was 1% in the age group 40–49 and 50–59 and 2% in the age groups 60–69 and 70–79 ().
Table 1 Adjustment of PSA for age in 110 Brazilian Macuxis Indians and estimated prostate cancer risk
Since the ratio of fPSA and tPSA has been reported to be a better determinant of prostate cancer risk, we aimed to calculate the ratio of fPSA to tPSA in different age groups and compared the median of the groups to conclude if there was any age-related change in fPSA/tPSA in this Indian population. shows the median values of fPSA/tPSA after subgrouping the patients by age. We did not find any significant difference in the median values of fPSA/tPSA in all the 4 groups, and there was no change in the prostate cancer probability in most of the age groups.
Table 2 Median and maximum values of fPSA/tPSA in different age groups
Since there seems to be an increasing trend in the PSA levels from younger age to older, we next aimed to find out if the trend showed a significant difference and if there was any correlation between the age and PSA values. We therefore performed correlation analysis to find a Pearson coefficient value. We calculated the correlation of individual age groups and their tPSA/fPSA (relation%), respectively, but did not find any correlation (data not shown). Hence, we next wanted to find out if the tPSA/fPSA (relation%) of different age groups has any correlation. As shown in , there was no significant correlation between the age group and the tPSA values (p-value >0.05 in all the 4 groups). The box plot of the data is shown in .
Figure 1 The box plot of data shows the correlation between the age group and the tPSA values (p-value <0.05 in all the 4 groups).
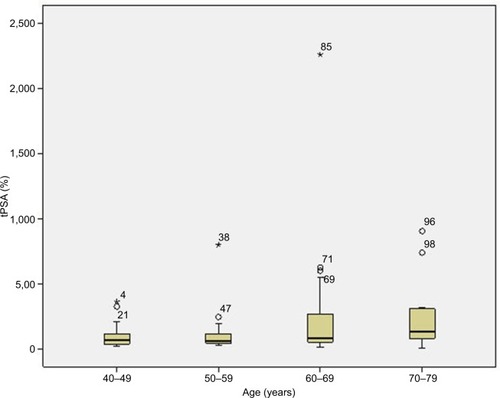
Table 3 Pearson correlation between tPSA after subgrouping patients according to age
Since we could not find any difference in the median values of fPSA/tPSA (relation%) in any of the 4 groups, we wanted to find out if the cumulative data of the values had any significant correlation with the age group. We did not find any significant correlation between the relation% and different age groups, except for the age groups 60–69 and 70–79 (p-value =0.008) (). Also, a borderline correlation was observed between PSA levels and age groups 40–49 and 70–79 (p-value =0.059) (). The box plot of fPSA vs age is shown in , and the box plot of relation% vs age is shown in .
Figure 2 Box plot of fPSA vs age.
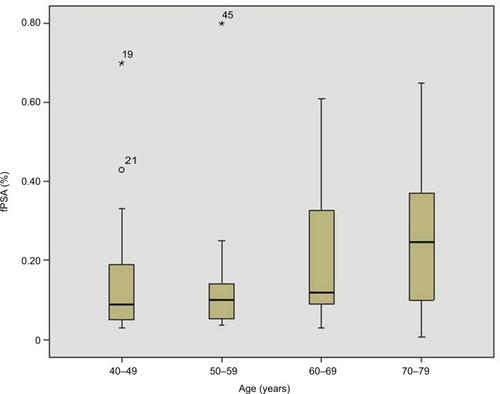
Figure 3 Box plot of fPSA/tPSA vs age.
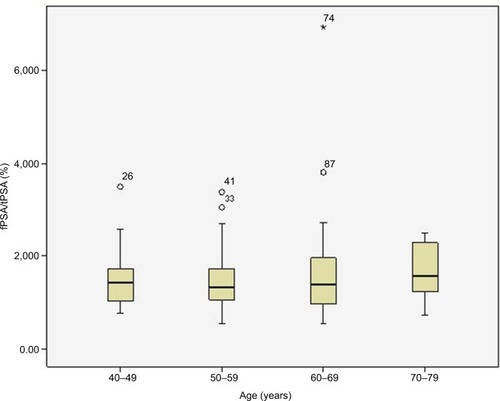
Table 4 Pearson correlation between fPSA/tPSA (%) after subgrouping based on age
Since we believe that subgrouping may reduce the power of the study, we wanted to find out if there was any correlation between age and the PSA levels (tPSA or the ratio) without subgrouping, ie, age was treated as a continuous variable. On performing correlation bivariate analysis on all the patients without subgrouping them, we found a significant correlation of tPSA and age (p=0.01) ().
Table 5 Pearson correlation between all ages and tPSA
We found a significant correlation between age groups 60–69 and 70–79 years (p=0.008) as shown in . On performing correlation bivariate analysis on all the patients and the fPSA/tPSA (relation%), we could not obtain any significance for this correlation related to age (p=0.398) ().
Table 6 Pearson correlation between all ages and fPSA/tPSA
We also performed a nonparametric test, Spearman test, to find out if there was any correlation between the age of patients and tPSA (), fPSA (), or relation% (). We found a significant correlation between the age of patients and tPSA (p-value =0.023) and fPSA (p-value =0.014), whereas no correlation was seen with the age of patients and relation% (p-value =0.485).
Table 7 Spearman correlation between all ages and tPSA
Table 8 Spearman correlation between all ages and tPSA
Table 9 Spearman correlation between all ages and tPSA
Discussion
PSA measurement is an important diagnostic tool to detect the development of prostate cancer, and the likelihood of prostate cancer detection increases with an increase in total PSA levels.Citation10,Citation11,Citation17 Our group has recently shown that in the Macuxis and Yanomamis tribal population, the testosterone and PSA values were similar with a progressive increase in PSA values with age.Citation26 Although there was an increase in the median and maximum PSA values in our study when the patients were subgrouped according to their age groups (), no significant correlation has been found after performing bivariate analysis to find their correlation with tPSA (). This is in agreement with a number of previous studies.Citation20,Citation21,Citation23,Citation27,Citation28 There was a significant correlation between the fPSA/tPSA ratio and the age groups 60–69 and 70–79 (). This significance is promising while comparing patients over 60 years of age, but it is not predictive of early detection of prostate cancer before 60 years of age. Some authors state that the age-specific reference ranges have never been officially approved, and no approval of the possible role of PSA screening has been obtained from the manufacturers of the commercially available PSA assays.Citation24 We do not rule out the possibility of low number of patients in each group after subdividing them into the 4 age groups, which may provide a false-positive or a false-negative result. To rule out this possibility of low power of the study, we also performed the bivariate analysis on the total patients and compared the age with tPSA, fPSA, and the relation% (fPSA/tPSA). Interestingly, we did find a significant correlation of patients’ age with tPSA (). But the correlation coefficient value is <0.3, so it is considered to have a low positive correlation. To our surprise, there was no correlation between fPSA/tPSA and the age of patients (). This is again in agreement with previous reports stating that for all the 3 ratios, f/tPSA (free to total PSA), c/tPSA (combined to total PSA), and f/cPSA (free to combined PSA), there was no correlation with patient age.Citation22,Citation25 Oesterling et alCitation23 stated the possibility that even though there is an increase in the serum concentration of each molecular form with advancing age, this age dependency is lost when the concentration of 1 molecular form is divided by the concentration of another to generate the ratio.Citation22 On the other hand, Berger et alCitation29 found that fPSA/tPSA significantly increases with age, which according to them may be due to an increase in prostate volume with advancing age.
Several investigators have assessed the impact of race on age-specific PSA reference ranges in prostate cancer and the effect of its ethnogeographical variation in different races. Most of the reports state that PSA levels are higher in black men as compared to white men regardless of age and history of prostate cancer.Citation30,Citation31 Some confliction reports do exist, suggesting no significant difference between tPSA levels in African-Americans and white men without prostate cancer in the population of southern Louisiana.Citation32 It was suggested that the different genetic and epigenetic factors in this region might be responsible for a different observation in this group of African-Americans and white men.Citation32 A study on a Singaporean population also showed no relationship between age and fPSA/tPSA ratio.Citation33 Similarly, another study on the Korean population failed to find any correlation of PSA with age in prostate cancer.Citation34 On the other hand, a study in Chinese men showed a strong correlation of PSA with age.Citation35 Our study has the limitations of low power, and among the patients enrolled in our study with prostate cancer indication, only one of them underwent biopsy. This low number is mainly due to the limited availability of medical resources and the limited mobility of the tribal population to hospitals in the city. The same trend was seen in some Asian countries, due to the restricted access to screening programs and urology clinics.Citation4 Although the incidence of prostate cancer is high among Asian-American individuals compared to the native Asian people, the mortality rate is still considerably lower in Western populations than in native Asian populations. This suggests the lack of facilities in these Asian countries, which could help the patients in early detection of the cancer. It also suggests genetic and environmental influences that might account for these variations.Citation4 The comparison of some demographic differences in the values of tPSA and % fPSA/tPSA in different populations is shown in . As is clear from the table, there is a similar pattern in the tPSA values in different ethnic groups when compared to the Brazilian Indians in our study ().
Table 10 Values of tPSA and fPSA/tPSA (%) in different demographic populations
A limitation of our study is that the evaluation of the Brazilian Indian population was limited to PSA measurement and its association with age in a relatively small cohort. Moreover, generally, prostate biopsy is needed for an accurate estimation of prostate cancer risk. However, in this case, we measured the PSA profile of an indigenous population from the Brazilian Amazon region, where people live in remote villages inside the Amazon forest, so it is difficult for them to access health care in urban centers. It is difficult to convince indigenous people to undergo biopsy procedure because of their concern related to cultural issues.
Conclusion
We found a significant correlation of age with tPSA and fPSA, but this was lost when the patients were subgrouped to find age-specific correlations of PSA levels in the tribal population of Macuxi. Although there are a large number of reports stating the age-dependent role of tPSA, fPSA, and their ratio, the data is still conflicting. It is therefore important to establish appropriate reference ranges for free, complexed, and tPSA as well as the ratios to integrate these new parameters as a diagnostic evaluation tool for early detection of early prostate cancer.Citation19 However, high PSA levels do not necessary indicate the presence of prostate cancer, and the cutoff PSA limits needs to be rectified. Decreasing or increasing the cutoff point may help in improving the sensitivity and specificity, since lowering the cutoff point increases the sensitivity, whereas increasing it improves specificity. Although PSA screening is a great beneficial tool for some male patients, the low specificity of the screening might provide false-positive results leading to overtreatment. It is therefore important to focus more on screening patients with an augmented genetic risk of developing prostate cancer, and enhancing the specificity of the PSA screening procedure. More studies need to be done including a large number of patients and using rectified cutoff limits.
Author contributions
MMLJr participated in the preparation of the manuscript, collected the data, and carried out the sample collection and examination. SSJF collected the data and carried out the sample processing and analysis. MTM participated in the preparation of the manuscript and analyzed the statistics. All
Disclosure
The authors report no conflicts of interest in this work.
References
- FerlayJParkinDMSteliarova-FoucherEEstimates of cancer incidence and mortality in Europe in 2008Eur J Cancer201046476578120116997
- BonoAVThe global state of prostate cancer: epidemiology and screening in the second millenniumBJU Int200494Suppl 312
- National Cancer InstituteProstate Cancer Treatment (PDQ®) – Health Professional Version. General Information About Prostate Cancer2015 [updated March 31, 2017; cited September 2, 2015] Available from: http://www.cancer.gov/cancertopics/pdq/treatment/prostate/HealthProfessional/Accessed June 1, 2018
- ItoKProstate cancer in Asian menNat Rev Urol201411419721224595118
- CussenotOValeriAHeterogeneity in genetic susceptibility to prostate cancerEur J Int Med2001121116
- FariaEFCarvalhalGFVieiraRASilvaTBMauadECCarvalhoALProgram for prostate cancer screening using a mobile unit: results from BrazilUrology20107651052105720472277
- GillilandFDKeyCRProstate cancer in American Indians, New Mexico, 1969–1994J Urol19981598938989474177
- FacinaTEstimativa 2012 – Incidencia de Cancer no BrasilRevista Brasileira de Cancerologia201157557
- De LimaMMJrde LimaMMGranjaFProstate cancer in Amazon native Indian: a case reportAsian Pharm Tech2014215
- CandasBLabrieFGomezJLRelationship among initial serum prostate specific antigen, prostate specific antigen progression and prostate cancer detection at repeat screening visitsJ Urol2006175251051616406983
- McGreevyKRodgersKLipsitzSBissadaNHoelDImpact of race and baseline PSA on longitudinal PSAInt J Cancer200611871773177616231314
- BalkSPKoYJBubleyGJBiology of prostate-specific antigenJ Clin Oncol200321238339112525533
- MillerBAChuKCHankeyBFRiesLACancer incidence and mortality patterns among specific Asian and Pacific Islander populations in the U.SCancer Causes Control200819322725618066673
- DuffyMJPSA in screening for prostate cancer: more good than harm or more harm than good?Adv Clin Chem20146612325344984
- StenmanUHHakamaMKnektPAromaaATeppoLLeinonenJSerum concentrations of prostate specific antigen and its complex with α1-antichymotrypsin before diagnosis of prostate cancerLancet19943448937159415987527116
- ThompsonIPaulerDGoodmanPPrevalence of prostate cancer among men with a prostate-specific antigen level ≤4.0 ng per milliliterN Engl J Med2004350222239224615163773
- CatalonaWJRichieJPAhmannFRComparison of digital rectal examination and serum prostate specific antigen in the early detection of prostate cancer: results of a multicentre clinical trial of 6,630 menJ Urol19941515128312907512659
- LeeRLocalioARArmstrongKA meta-analysis of the performance characteristics of the free prostate-specific antigen testUrology200667476276816600352
- MieleMEPercent free PSA as an additional measure in a prostate cancer screenClin Lab Sci200114210210715625982
- CollinsGNLeeRJMcKelvieGBRogersACHehirMRelationship between prostate specific antigen, prostate volume and age in the benign prostateBrit J Urol19937144454507684650
- OesterlingJEJacobsenSJChuteCGSerum prostate specific antigen in a community based population of healthy men: establishment of age-specific reference rangesJAMA199327078608647688054
- LudererAAChenYTSorianoTFMeasurement of the proportion of free to total prostate specific antigen improves diagnostic performance of prostate specific antigen in the diagnostic grey zone of total prostate specific antigenUrology19954621871947542820
- OesterlingJEJacobsenSJKleeGGFree, complexed and total prostate specific antigen: the establishment of appropriate reference ranges for their concentrations and ratiosJ Urol19951543109010957543605
- LuboldtHJSchindlerFSRubbenHAge-specific reference ranges for prostate-specific antigen as a marker for prostate cancerEur Urol200753848
- KalishLAMcKinlayJBSerum prostate-specific antigen levels (PSA) in men without clinical evidence of prostate cancer: age-specific reference ranges for total PSA, free PSA, and percent free PSAUrology19995461022102710604702
- De Lima JuniorMMReisLOFerreiraUUnraveling Brazilian Indian Population prostate good health: clinical, anthropometric and genetic featuresInt Braz J Urol201541234435226005978
- DalkinBLAhmannFRKoppJBProstate specific antigen levels in men older than 50 years without clinical evidence of prostatic carcinomaJ Urol19931506183718397693980
- CrawfordEDReport on the 1993 prostate cancer awareness weekAbstract presented at: Annual Meeting of the American Urological AssociationMay 14–19, 1994San Francisco, CA, USA
- BergerAPCheliCLevineRKlockerHBartschGHorningerWImpact of age on complexed PSA levels in men with total PSA levels of up to 20 ng/mLUrology200362584084414624905
- DeAntoniEPCrawfordEDOesterlingJEAge and race-specific reference ranges for prostate-specific antigen from a large community-based studyUrology19964822342398753735
- MoulJWSesterhennIAConellyRRProstate specific antigen values at the time of prostate cancer diagnosis in African-American menJAMA199527416127712817563532
- MartinBCheliCPollardSSimilar age-specific PSA, complexed PSA, and percent cPSA levels among African-American and white men of southern Louisiana. Prostate-specific antigenUrology200361237537912597951
- SawSAwTCAge-related reference intervals for free and total prostate-specific antigen in a Singaporean populationPathology200032424524911186419
- KimJHLeeSWKimJHAssociation between obesity, prostate-specific antigen level and prostate-specific antigen density in men with a negative prostate biopsyJ Int Med Res201442382182724743874
- HeDWangMChenXEthnic differences in distribution of serum prostate-specific antigen: a study in a healthy Chinese male populationUrology200463472272615072888