
Abstract
Introduction
Leydig cell tumors (LCT) are the most common hormone-secreting testicular tumors; it is a rare cause for precocious pseudo-puberty in boys. The tumors secrete high amounts of testosterone. We present two cases of LCT in prepubertal boys presenting with precocious puberty.
Case Reports
Case 1. A 6-year-old boy was referred from the pediatric department with a diagnosis of precocious puberty. The patient had reported enlarged and painless swelling of the left testicle from a year ago. The puberty status of the patient was A1P3G4. Ultrasonography examination had found left testicular mass. Elective radical orchiectomy of the left testicle was performed. Histopathological analysis confirmed the diagnosis of benign LCT. Case 2. A 6-year-old boy presented with an enlarged left testicle for the last three months. Features of puberty were noted on the patient (appearance of pubic and facial hair). The puberty status of the patient was A1P3G3. Left testicle US had found homogenous, hypoechoic mass with calcification. Bone age had found increased bone maturation. Increased androgen hormones were detected through a blood test. Radical orchiectomy of the left testicle was performed. The histopathological examination showed malignant LCT.
Conclusion
Leydig cell tumors uncommonly occur in children. Prepubertal-aged boys presented with asymmetrical, firm, painless testicular enlargement with signs of puberty should be evaluated for LCT. Histopathological analysis is the mainstay of diagnosis and radical orchiectomy is the treatment of choice of LCT.
Introduction
Leydig cell tumors (LCT) are the most common hormone-secreting testicular tumors and are an unusual cause of precocious pseudo-puberty in boys. It is one form of testicular tumor, presenting in 3–6% of all testicular masses found in prepubertal males. Less than 25% of these tumors have been found in boys aged between 5 and 10 years. Most of the cases were unilateral and benign in the presentation. Only up to 10% of all reported cases in adults were malignant tumors during a further investigation, while no report mentioned malignant LCT cases in children.Citation1–Citation3 Leydig cell tumors present as functionally active tumors, producing high testosterone levels.Citation2 We present two cases of LCT in prepubertal boys, manifesting with precocious puberty with the different histopathological results.
Case Report
Case 1
A 6-year-old boy was referred from the pediatric department with precocious puberty and enlarged left testicle starting a year before the presentation. The lump was painless, and no inflammatory sign was noted. The pubertal state of the patient was A1P3G3–4 (see , ).
Figure 1 Acne and facial hair (A) and enlarged penis with scant pubic hair (B) in a 6-year-old boy, showing signs of precocious pseudo-puberty as shown on both cases. Advanced bone age of Case 2 (C).

Table 1 Characteristics of Patients
The hormonal assays showed prepubertal levels of gonadotropin, increased level of testosterone, and normal levels of AFP, β-HCG, and LDH (see ). Ultrasound revealed an enlarged abnormal left testicle ultrasound, as shown in A. Chest x-ray, abdominal ultrasonography, and abdominal-pelvis magnetic resonance imaging (MRI) results were within normal limits.
Figure 2 Ultrasound of the testicles of Case 1 (A) and Case 2 (B).
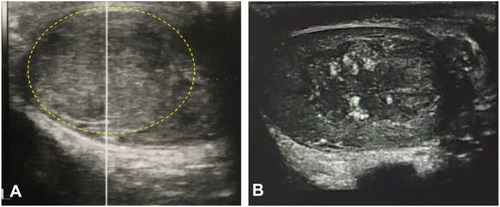
Table 2 Hormonal Assessment of the Patients
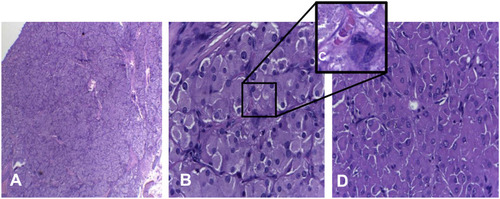
Radical inguinal orchiectomy of the left testicle was performed under general anesthesia. The excised left testicle’s dimensions were 4.5 x 3 x 2 cm with a greyish color, firm, and smooth surface (see ) and the histopathological examination had revealed yellowish-brownish tumor mass with an indistinct border, lobulated, separated by connective tissue. Tumor cells were mildly pleomorphic with eosinophilic granules and intracytoplasmic Reinke crystals. No signs of mitosis, necrosis, or lymphovascular invasion. The tumor did not infiltrate the epididymis and seminiferous tubules (see ). These findings confirmed the diagnosis of a benign LCT. Testosterone serum level was decreasing while US and MRI showed normal result without visible recurrence or metastasis on six-month follow-up.
Figure 3 Macroscopic anatomy findings of the left testis from the patient of Case 1 (A) and Case 2 (B). Note a well circumscribed yellowish-brownish mass inside the testis.
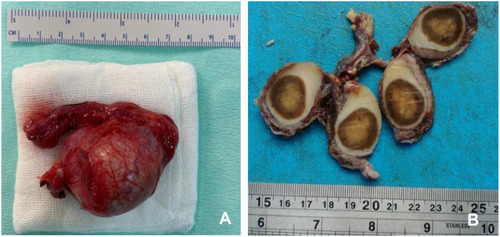
Figure 4 (A) The tumor mass was lobulated had indistinct border; (B) spherical nuclei of tumor cells, pleomorphic, granulated eosinophilic cytoplasm, (high power field, 400x); (C) Reinke crystal. (D) Solid tumors formed nest.
Case 2
A 6-year-old boy with an enlarged left testicle starting 3 months before the presentation. Enlarged left testicle was painless without signs of inflammation, while the right testicle was normal. The pubertal state was A1P3G3 (see ).
Hormonal assays demonstrated prepubertal levels of gonadotropins of LH and FSH. Tumor marker levels of AFP, β-HCG, and LDH were normal (see ). Further hormonal tests showed a slightly increased level of 17-OH progesterone (17-OHP), androstenedione, and testosterone while DHEA-S concentration was normal. Abnormal left testicle was revealed on US and MRI, while bone age was advanced in X-ray (see , ).
The patient was treated with hydrocortisone (dosage of 10 mg/m2) due to increased 17-OHP, suggesting non-classic congenital adrenal hyperplasia (NCCAH). Further follow-up on pubertal signs did not show any improvement with slight reduction on the level of 17-OHP.
Radical inguinal orchiectomy of the left testicle was performed under general anesthesia. The excised left testicle had dimensions of 8.5 x 3 x 2.5 cm with a brownish color, firm, and smooth surface mass inside the testis (see ). The histopathological examination had revealed tumor mass forming a nest (separated by fibrovascular septa); polygonal shape; pleomorphic; coarse chromatin; eosinophilic; and active mitosis in more than 3 out of 10 cells (in high power field) (see ). Several cells with bizarrely shaped (atypical) nuclei were found. Tumor cell invasion to the epididymis and seminiferous tubules was not found. These findings confirmed the diagnosis of LCT with suspected features of malignancy. Testosterone serum level was decreasing and almost reaching normal level on nine-month follow-up (see ). The patient was scheduled for a further visit to follow up on the possibility of recurrence or metastasis.
Discussion
Among all testicular tumors, germ cell tumors and gonadal stromal tumors are the two predominant primary testicular tumors. Leydig cell tumors are sex cord-stromal tumors that arise from Leydig cells, located in the testicular interstitial between the seminiferous tubules. Tumors arising from Leydig cells produce testosterone in response to stimulation by LH. The tumor mainly occurs on adult patients between 20–60 years of age and most commonly asymptomatic, partially due to the prior virilization from increased testosterone concentration that had occurred after pubertal development in such age groups. Leydig cell tumors are uncommon in children, affecting between 4% and 9% of all primary testicular tumors in prepubertal patients, with the highest incidence of 5–10 years of age.Citation1,Citation4
Leydig cell tumors in prepubertal ages manifest in a spectrum from atypical founding without systemic signs with only testicular asymmetry to, more commonly, various signs of precocious pseudo-puberty in the physical examination.Citation5 Further investigations may reveal abnormalities in imaging studies (primarily US) and plasma hormone profiles. Leydig cell tumors are biologically active, secreting testosterone as a response towards LH stimulation, thus causing the appearance of precocious puberty despite the absence of activation of the hypothalamic-pituitary axis.Citation1 In our case, both cases present with the previous complaint of precocious puberty; the first patient had reported the growth of facial hair; both patients had reported having increased penis size and appearance of scant pubic hair despite being aged six at the time of the diagnosis.
In accordance with peripheral precocious puberty, gonadotropin in both cases was in prepubertal levels. The pubertal features in both cases were caused by remarkable increase in androgen hormones, testosterone and androstenedione, which might be produced by testicle tumors. Hormonal phenotypes between boys and girls highlight the distinct manifestation both in hormonal and pathological standpoint. A male patient with an LCT may present with complete suppression of gonadotropins, whereas a female patient will not. It may be partially explained by the relative amounts of androgens and estrogens secreted by the tumor and/or by more efficient extra-tumoral aromatization of testosterone to estradiol in the male patients. Androgens do not exert a direct inhibitory effect on gonadotropin secretion while estrogens create negative feedback on LHRH-secreting cells and reduce FSH secretion and amplitude of LH pulses by exerting its effects on the pituitary gland.Citation5,Citation6 As in our report, Case 1 showed suppressed gonadotropins, which might be explained by more significant increase in testosterone level.
Leydig cell tumor diagnosis might be challenging in cases with congenital adrenal hyperplasia (CAH).Citation6,Citation7 Case 2 had slight increased level of 17-OHP which leads to suggest NCCAH. However, the level of 17-OHP was not suitable enough to cause significant increment in androgen levels and signs of puberty. Furthermore, HC treatment did not reduce the size of testicles. The TART presents mostly in classic form of CAH as bilateral testicle enlargement with extra testicular nodules located at hilum. This should explain that Case 2 was unlikely to have TART, which was confirmed by the histopathological features.
The most commonly used imaging study in diagnosing the condition was US to screen and detect scrotal, testicular, and/or pelvic mass; histopathological examination under a microscope serves as the definitive and confirmatory examination for such tumors.Citation9 Previous imaging using US is deemed sufficiently sensitive and specific in diagnosing testicular masses.Citation10 Due to the histologic characterization uncertainties, it appears advisable to perform an initial CT scan or MRI of the abdomen to rule out metastatic disease.Citation3,Citation10
The confirmatory test of the tumor requires the tissue sample from a surgical biopsy or orchiectomy to be analyzed microscopically for its histopathological features. Macroscopically, Leydig cell tumors are usually small, with most cases presenting with masses less than 5 cm, with the well-circumscribed and solid brownish surface. The low-power histological analysis may find diffuse sheets or large nodules of eosinophilic tumor cells. The cytoplasm of the tumor cells may contain Reinke crystals in up to 30% of the cases. Calcification, ossification, and adipocytic metaplasia may be found in several cases. Both of our cases showed the typical appearance of LCT histopathology, with Reinke crystal was found in the first case. Further immunohistochemistry tests using inhibin (95% cases), calretinin (90% of cases), and Melan-A may support the diagnosis for LCT.Citation8
The suspicion of malignancy may be raised with 2 of the following criteria: greater than 5 cm in diameter, infiltrative borders, nucleic atypia, active mitosis (>3/10 high power fields), vascular invasion, and/or necrosis. In our second case, two criteria of malignancy criteria, which were nucleic atypia and active mitosis, were found. Although it reported that malignant LCT was found in minority cases in adults, as far as we know, this is the first report of Leydig cell tumor with suspicion of malignancy in a pediatric case. Some studies suggest evaluating using an increased expression of Ki67/MIB-1 and p53, DNA aneuploidy and bcl-2 in suspected malignancy.12,13
The mainstay treatment of testicular masses in children is orchiectomy of the affected testicle. Several studies had noted normalization of hormonal profile in children who had received orchiectomy in LCT. In our case, both patients were treated with radical inguinal orchiectomy for consideration of unknown malignant potency and social consideration that both patients living in the remote area and had difficulty to control regularly. Specifically, for the second case, the center position of the tumor inside the testis and suspicion of malignancy (manifested in significant mitotic activity and nucleic atypia in histopathological examination) may justify the decision to perform radical orchiectomy on the patient.
An alternative surgical approach using testis-sparing methods may also be utilized in such cases. Luckie et al suggested that the decision to treat the testicular masses, either with relatively conservative organ-preserving surgery or radical orchiectomy, lies in the clinical findings during the surgery: intraoperative tumor size, location, and the amount of remaining normal testicular parenchyma, facilitated by ultrasound guidance and intraoperative frozen section diagnosis.Citation9 Due to the scarcity of data regarding the comparison of long-term outcomes between organ-preserving surgery and radical orchiectomy in children with LCT, further studies may be required to establish the standard guidelines.
Either orchiectomy or testis-preserving surgery, long term follow-up is needed after surgery. It is also needed for the possibility to have analog GnRH for the potential central precocious puberty and growth hormone for precocious puberty-related advanced bone age and compromised adult height.Citation9,Citation10 Surgery should always be considered as the first option in localized malignant LCT. Further treatment using chemotherapy and radiotherapy has yet to show any noticeable benefit for metastatic malignant LCT. Lack of efficacy in chemotherapy and radiotherapy may warrant further investigation with varying clinical demographics to establish the factors that may contribute to the resistance of such therapies.
The case report presents several limitations associated with its study design and lack of follow-up for the patients included in this study. As such, the risk of recurrence cannot be ascertained from this study alone. Despite the limitations, the study had reported relatively rare cases of LCT.
Conclusion
The LCTs are hormone-secreting testicular tumors that rarely occur in children. Both of our cases present with precocious puberty, manifesting in increased genital size and pubic hair despite the prepubertal age, and increased hormonal profile while presenting different histopathology result. Both cases were treated successfully with radical orchiectomy, even though testis-preserving surgery emerges as an alternative option. Further metabolic and hormonal follow-ups may be required, as well as tumor recurrence status and the possibility of metastasis in the malignancy case.
Ethics Approval and Consent to Participate
The Institutional Review Board of Faculty Medicine Universitas Indonesia approved this study with No. KET-43/UN2.F1/ETIK/PPM.00.02/2020. The parents of the patients provided informed consent for the case details and images to be published.
Acknowledgment
The authors would like to express our gratitude to Dr. Lisnawati from the Department of Anatomical Pathology, Cipto Mangunkusumo General Hospital, Faculty of Medicine Universitas Indonesia, to contribute to review of pathological specimens of the tumor.
Disclosure
The authors declare no potential conflicts of interest.
References
- Verrotti A, Penta L, Zenzeri L, Lucchetti L, Giovenali P, De Feo P. True precocious puberty following treatment of a Leydig cell tumor: two case reports and literature review. Front Pediatr. 2015;3:93. doi:10.3389/fped.2015.00093.26579503
- Ruf C, Sanatgar N, Isbarn H, et al. Leydig-cell tumour of the testis: retrospective analysis of clinical and therapeutic features in 204 cases. World J Urol. 2020;38:2857–2862. doi:10.1007/s00345-020-03079-1.31960106
- Engels M, Span PN, van Herwaarden AE, Sweep FCGJ, Stikkelbroeck NMML, Claahsen-van der Grinten HL. Testicular adrenal rest tumors: current insights on prevalence, characteristics, origin, and treatment. Endocr Rev. 2019;40(4):973–987. doi:10.1210/er.2018-00258.30882882
- García González M, Casal-Beloy I, Somoza Argibay I, Dargallo Carbonell T. Atypical presentation of Leydig cell tumour in three prepubertal patients: diagnosis, treatment and outcomes. J Pediatr Endocrinol Metab. 2019;32(4):369–374. doi:10.1515/jpem-2018-0467.30875329
- Mameli C, Selvaggio G, Cerini C, et al. Atypical Leydig cell tumor in children: report of 2 cases. Pediatrics. 2016;138(5):e20160151. doi:10.1542/peds.2016-0151.27940757
- Mukhopadhyay M, Das C, Sarkar S, Mukhopadhyay B, Mukhopadhyay B, Patra R. Leydig cell tumor of testis in a child: an uncommon presentation. J Indian Assoc Pediatr Surg. 2017;22(3):181. doi:10.4103/jiaps.JIAPS_4_17.28694581
- Chaudhari M, Johnson EK, DaJusta D, Nahata L. Testicular adrenal rest tumor screening and fertility counseling among males with congenital adrenal hyperplasia. J Pediatr Urol [Internet]. 2018;14(2):155.e1–155.e6. doi:10.1016/j.jpurol.2017.11.011
- Mooney KL, Kao C-S. A contemporary review of common adult non-germ cell tumors of the testis and paratestis. Surg Pathol Clin. 2018;11(4):739–758. doi:10.1016/j.path.2018.07.00230447839
- Luckie TM, Danzig M, Zhou S, et al. A multicenter retrospective review of pediatric Leydig cell tumor of the testis. J Pediatr Hematol Oncol. 2019;41(1):74–76. doi:10.1097/MPH.000000000000112429554024
- Sarier M, Tunç M, Özel E, et al. Evaluation of histopathologic results of testicular tumors in antalya: multi center study. Bull Urooncol. 2020;19:64–67. doi:10.4274/uob.galenos.2019.1412