 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background
Vascular α2B-adrenoreceptors have the potential to increase blood pressure by mediating vasoconstriction. A nine-nucleotide deletion in the receptor enhances vasoconstriction and exacerbates hypertension. The aim of this study was to determine the association between insertion/deletion (I/D) polymorphism of the α2B-adrenoceptor and hypertension with and without diabetes.
Methods
The study was carried out in 35 hypertensive patients with diabetes, 35 hypertensive patients without diabetes, and 30 healthy controls. Clinical data, blood lipid profiles, and I/D polymorphism were assessed.
Results
Hypertensive patients were significantly older, with significantly higher systolic/diastolic blood pressures and worse plasma lipid profiles than controls. The frequency of the DD genotype was significantly higher in both hypertensive patients with (77.14%, P < 0.01) and without (71.43%, P < 0.05) diabetes versus controls (40%). Also, the D allele was significantly more common in both hypertensive patients with (84.29%, P < 0.01) and without (80%, P < 0.05) diabetes versus controls (58.33%). Hypertensive patients were more likely to have the D allele with (3.83-fold) and without (2.85-fold) diabetes. The frequencies of the DD genotype and the D allele were not significantly (P > 0.05) different between the patient groups. The DD genotype was associated with significantly lower high-density lipoprotein (P = 0.001) and significantly higher low-density lipoprotein (P = 0.017) levels versus the II and ID genotypes in the hypertensive group without diabetes.
Conclusion
A marked and statistically significant association between DD genotype and D allele of I/D polymorphism in the α2B-adrenoceptor gene may be a risk factor for hypertension ± diabetes. The association between the DD genotype and dyslipidemia may partially explain its role in precipitating hypertension.
Introduction
Hypertension is a greater burden at the population level in economically developing rather than developed countries.Citation1 It has been identified as the leading risk factor for mortality, and is ranked third as a cause of disability-adjusted life-years.Citation2 Data from the National Health and Nutrition Examination Survey for 2005–2006 found that 29% of US adults aged ≥18 years were hypertensive.Citation3,Citation4 Data on 6671 individuals from the 2008 Egyptian Demographic and Health Survey found that the overall prevalence of prehypertension and hypertension in Egypt was 57.2% and 17.6%, respectively. Only 25.2% of the population had normal blood pressure < 120/80 mmHg.Citation5 The highest prevalence of hypertension was found in the Ismailia, Alexandria, Menya, Menoufia, and Luxor governorates.Citation5
Primary hypertension in humans is likely to be of a complex nature, arising from environmental and genetic factors.Citation6 The alpha2-adrenergic receptor (α2-AR) is widely expressed within the central and peripheral nervous systems. It mediates diverse physiological functions of the sympathetic nervous system, and is also involved in the pathogenesis of cardiovascular disease and modulation of pain.Citation7,Citation8
Three distinct α2-AR subtypes, ie, α2A, α2B, and α2C, that mediate many of the physiological actions of the catecholamines, epinephrine and norepinephrine, have been described.Citation9,Citation10 They belong to the family of G protein-coupled receptors and are linked to the inhibitory G proteins.Citation9,Citation10 The α2-ARs mediate a wide variety of functions, including regulation of blood pressure, sympathetic tone, lipolysis, and insulin secretion.Citation11,Citation12
Studies have suggested that sympathetic outflow from the central nervous system is inhibited by stimulation of α2-AR, thus mediating a hypotensive effect, whereas stimulation of the α2B-AR mediates a hypertensive effect by opposing sympathetic inhibition by α2A-AR in the central nervous system. The α2C-AR does not seem to have any effect in the regulation of blood pressure.Citation6
All three α2-AR subtypes are expressed in both the exocrine and endocrine cells of the human pancreas, including beta cells.Citation13 Insertion/deletion (I/D) polymorphism in the α2B-AR was reported to be associated with impaired beta cell function in a group of Finnish subjects with impaired glucose tolerance. Interestingly, this genetic polymorphism may also predispose its carriers to type 2 diabetes.Citation14
The α2B-AR is critically involved in cardiovascular regulation, because disruption of its genes in mice affects blood pressure responses to α2-AR agonists, eg, clonidine.Citation9,Citation15 The α2B-AR gene is located on chromosome 2 in a region where several genome scansCitation16 have found linkage with blood pressure variation and hypertension.Citation17–Citation19 In the third intracellular loop of the receptor, in an area of importance in downregulation, there is a polymorphism consisting of either an insertion or a deletion of three glutamate amino acids at positions 301–303.Citation6,Citation20
The 301–303 deletion variant is phosphorylated only half as efficiently and fails to undergo homologous desensitization. This indicates that the α2B-AR 301–303 deletion variant might increase long-term receptor signaling (ie, induce vasoconstriction) by preventing normal agonist-mediated desensitization.Citation21 Earlier studies showed a conflicting association of the α2B-AR deletion allele with hypertension. The aim of this study was to determine if I/D α2B-AR polymorphism is a risk factor for hypertension, and if type 2 diabetes mellitus augments this association in a sample of Egyptian patients.
Materials and methods
Subjects
The patients in this study were selected from the Hypertension Clinic, Department of Cardiology, Menoufiya University Hospital. A full history and a general and clinical examination was performed prior to selection. Ethical approval for this investigation was obtained from the research ethics committee at the Faculty of Medicine, Menoufiya University.
The study included a total of 35 hypertensive subjects with type 2 diabetes mellitus, 35 hypertensive subjects without diabetes, and 30 healthy individuals. Exclusion criteria were familial hypercholesterolemia, cancer, renal disease, and any other chronic illness.
Essential hypertension was defined as systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥ 90 mmHg, or current antihypertensive therapy.Citation22 Resting blood pressure was measured in the right arm using a sphygmomanometer.
Type 2 diabetes mellitus was defined as fasting plasma glucose ≥ 126 mg/dL (≥7.0 mmol/L) or symptoms of hyperglycemia and a random plasma glucose ≥ 200 mg/dL (≥11 mmol/L).Citation23 Thirty healthy individuals were selected from volunteers with a negative history of hypertension and diabetes, with a resting systolic blood pressure ≤ 120 mmHg and diastolic blood pressure ≤ 80 mmHg on at least two separate occasions and not receiving any medications. The subjects were divided into group 1 (hypertension with diabetes), group 2 (hypertension without diabetes), and group 3 (control subjects).
Analysis of lipid profiles
A 5 mL sample of venous blood was taken from each patient after an overnight fast for determination of total serum cholesterol, triglycerides, and high-density lipoprotein (HDL) cholesterol levels. Lipid profiles were measured using standard enzymatic colorimetric kits (Spinreact, La Vall D’En Bas, Spain). Serum low-density lipoprotein (LDL) cholesterol was calculated by this formula as triglyceride levels not exceed 400 mg/dL:
DNA analysis
A 5 mL sample of venous blood was collected slowly into an evacuated tube containing ethylenediamine tetra-acetic acid for isolation of peripheral blood mononuclear cells using Lymphoflot solution (Bio Test AG, Dreieich, Germany). Briefly, a 5 mL sample of the patient’s blood was added to an equal volume of saline and mixed carefully. This diluted blood sample was carefully layered onto the Lymphoflot solution so as not to mix the Lymphoflot solution and the diluted blood sample. The mixture was centrifuged at 1500 rpm for 25 minutes at 20°C. The upper plasma layer was drawn off, leaving the lymphocyte layer undisturbed at the interface. The lymphocyte layer was transferred into a clean centrifuge tube containing 4 mL of balanced salt solution and mixed gently, then centrifuged at 1500 rpm for 10 minutes at 4°C. The supernatant was discarded, after which 1 mL of phosphate-buffered saline was added to the lymphocyte pellet, and transferred to a clean CryoTube™ by pipette and stored at −80°C for further DNA extraction and purification.Citation25
Genomic DNA was extracted from peripheral blood mononuclear cells using QIAamp DNA blood mini kits (Qiagen Hilden, Qiagen, Valencia, CA), to yield pure DNA and stored at −20°C for direct amplification. I/D mutation of α2B-AR was detected using the polymerase chain reaction (PCR) method, as previously described.Citation26
DNA was amplified using a forward primer, 5′-AGGGTGTTTGTGGGGCATCT-3′ and a reverse primer, 5′-CAAGCTGAGGCCGGAGACACT-3′ (Midland Certified Reagent Co, Midland, TX). A total volume of 25 μL reaction mixture containing 20 pmol of each primer, 0.4 mmol/L of dNTP, 2 mmol/L of MgCl2, 1 × Taq buffer, 100 mL/L of dimethyl sulfoxide, one unit of Taq DNA polymerase (New England Biolabs, Beverly, MA), and the template DNA was used for amplification of I/D polymorphism in the ADRA2B gene using a 2400 thermal cycler (Perkin Elmer, Boston, MA). The I/D mutation of α2B-AR was shown clearly using a protocol of initial denaturation for 10 minutes at 95°C, denaturation for one minute at 94°C, annealing for 2 minutes at 66°C, extension for one minute at 72°C for 35 cycles, and final extension for 10 minutes at 72°C.
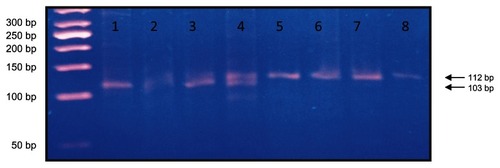
I/D mutation of α2B-AR was detected in the PCR bands in 3% agarose gel electrophoresis and visualized under ultraviolet light. I/D mutation of α2B-AR PCR bands appeared as DD at 103 base pairs, II at 112 base pairs, and ID at both 112 base pairs and 103 base pairsCitation26 ().
Figure 1 Lane 1 shows DD genotypes at 103 base pairs, lanes 2–4 show ID genotype at 103 and 112 base pairs, and lanes 5–8 show II genotypes at 112 base pairs using a 50-base pair ladder.
Statistical analysis
The results were statistically analyzed using the Statistical Package for the Social Sciences version 14 (SPSS Inc, Chicago, IL). Two types of statistics were included, ie, descriptive statistics (percentage, mean, and standard deviation) and analytic statistics, whereby genotypes and allelic frequencies of I/D polymorphism of the α2B-AR were compared between hypertensive patients with and without diabetes and controls using the Chi-square (χ2), Mann-Whitney, and Kruskal-Wallis tests. All odds ratios involving genotypes and alleles were calculated. A two-tailed Student’s t-test was used to compare quantitative data. Statistical significance was considered to be statistically significant at the P < 0.05 value.
Results
Our results showed significantly higher age (P < 0.05), systolic and diastolic blood pressure (P < 0.001), total cholesterol (P < 0.01), triglycerides (P < 0.01), and LDL cholesterol (P < 0.05), and lower HDL cholesterol (P < 0.01) in hypertensive patients with diabetes versus controls (). There was no significant difference in gender distribution or smoking status (P > 0.05) between hypertensive patients with diabetes and controls. There was a significant higher age (P < 0.01), systolic and diastolic blood pressure (P < 0.001), proportion of males (P < 0.05), and LDL cholesterol (P < 0.05), and lower HDL cholesterol (P < 0.001) in hypertensive patients without diabetes versus controls, with no statistically significant differences between the two groups for smoking (P > 0.05), total cholesterol (P > 0.05), or triglycerides (P > 0.05, ). Significantly higher triglyceride levels (P < 0.05) were found in hypertensive patients with diabetes than in those without diabetes, but there was no significant difference in any other parameters between these two groups ().
Table 1 Demographic and clinical characteristics of hypertensive patients with and without diabetes and controls
The distribution of I/D genotypes and α2b-AR alleles in patients with hypertensive ± diabetes and controls is shown in and . The DD genotype was significantly more common in hypertensive patients with (77.14% versus 40.0%, P < 0.01) and without type 2 diabetes (71.43% versus 40.0%, P < 0.05) compared with controls. The D allele was significantly more common in hypertensive patients with (84.29% versus 58.33%, P < 0.01) and without type 2 diabetes (80% versus 58.33%, P < 0.05) compared with controls. There were no statistically significant differences (P > 0.05) in I/D genotypes and alleles between hypertensive patients with and without diabetes. Odds ratios for the DD and ID genotypes and the D allele in hypertensive patients with type 2 diabetes were 5.25 (95% confidence interval [CI] 1.15–23.86, P < 0.01), 1.06 (95% CI 0.19–5.91, P < 0.01), and 3.83 (95% CI 1.68–8.72, P < 0.01), respectively, while odds ratios for the DD and ID genotypes and the D allele in hypertensive patients without type 2 diabetes were 3.64 (95% CI 0.89–14.91, P < 0.05), 0.95 (95% CI 0.19–4.63, P < 0.05), and 2.85 (95% CI 1.31–6.22, P < 0.05, ).
Figure 2 Distribution of I/D genotypes and alleles of α2B adrenergic receptor in hypertensive patients with and without diabetes and control.
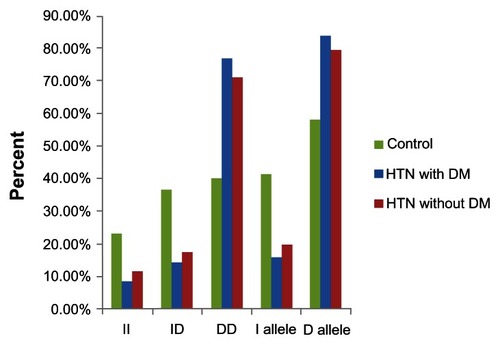
Table 2 Distribution of I/D genotypes and alleles in hypertensive patients with and without diabetes and controls
There was no statistically significant difference between the II, ID, and DD phenotypes with regard to age, gender distribution, smoking, diastolic and systolic blood pressure, total cholesterol, or triglycerides. However, patients with the DD genotype had significantly lower HDL (P = 0.001) and higher LDL (P = 0.017) levels than those with the II and ID genotypes in the hypertensive group without type 2 diabetes ( and ).
Table 3 Clinical parameters in different I/D genotypes in hypertensive patients with and without diabetes and controls
Table 4 Clinical parameters and lipid profile in different I/D genotypes in hypertensive patients with and without diabetes and control groups
Discussion
The α2B-AR is encoded by the ADRA2B gene located on chromosome 2 and mediates a variety of functions. A polymorphism (12Glu9) resulting in insertion or deletion of three glutamic acid residues from an acidic stretch in the third intracellular loop has been described.Citation27 The deletion allele has been found to be associated with adverse metabolic and vascular effects, including reduced basal metabolic rate,Citation28 obesity,Citation29 impaired insulin secretion,Citation14 earlier onset of diabetes,Citation30 increased risk of acute coronary ischemia,Citation31 and autonomic dysfunction, and increased sympathetic nervous system activity.Citation32 The present study was carried out to clarify the role of the deletion allele of α2B-AR in hypertension and if diabetes augments this association or not.
The present study showed significantly higher age, systolic and diastolic pressure, total cholesterol, triglycerides, and LDL cholesterol, and lower HDL cholesterol in hypertensive patients than in controls. These results are in agreement with other reports showing significant elderly, systolic and diastolic hypertensive,Citation6,Citation26 and lower HDL cholesterol.Citation26 There was no significant difference between the II, ID, and DD genotypes with regard to age, gender, smoking, systolic and diastolic blood pressure, total cholesterol, and triglycerides. These results are consistent with those reported previously;Citation26 however, in our study, the DD genotype was associated with higher LDL cholesterol and lower HDL cholesterol in hypertensive patients without diabetes, indicating that the deletion allele may induce hypertension. Association of deletion allele with dyslipidemia may also attribute to hypertension in addition to receptor desensitization and vasoconstriction so it can be considered as a risk factor for hypertension and coronary artery diseases.
The present study shows a significant association between the DD genotype, the D allele, and hypertension ± diabetes, and this finding is in agreement with other reports.Citation6,Citation26,Citation33,Citation34 However, some studies have reported no significant association between the D allele and hypertension.Citation31,Citation35
The hypertensive effect mediated by the α2B-AR has been shown to be especially important in individuals with salt-sensitive hypertension because salt sensitivity is associated with a positive family history of primary hypertension, and is also a characteristic in a large proportion of patients with primary hypertension.Citation6
There is also evidence that the α2B-AR mediates peripheral vasoconstriction. In vivo studies have shown that the DD genotype of the receptor is associated with reduced dilatation of the brachial artery, reduced coronary blood flow, and increased peripheral resistance in response to adrenaline infusion.Citation6
Our study showed that the DD genotype increased the risk of hypertension ± diabetes as compared with controls (by 5.25-fold and 3.65-fold, respectively) and the D allele increases the risk of hypertension ± diabetes as compared with controls (by 3.83-fold and 2.85-fold, respectively). We also showed a stronger association between the DD genotype, the D allele, and hypertension with diabetes, that may indicate potential use of deletion genotype as a risk factor for diabetes.
Earlier studies reporting a rather weak association between the DD genotype and nondiabetic primary hypertension and a stronger association with early-onset hypertension is by no means surprising, given that the hereditary component of primary hypertension is likely to be the sum of many genes, for which the effect of an individual gene is likely to be small to moderate, and the diabetic phenotype seems to add complexity to the phenotype of primary hypertension.Citation6
Siitonen et al reported that the common I/D polymorphism of the α2B-AR influences receptor function by impairing agonist-promoted receptor phosphorylation and desensitization. Based on this observation, they postulated that impairment of α2B-AR desensitization due to I/D polymorphism causes prolonged inhibition of insulin secretion from pancreatic beta cells. Via this mechanism, the polymorphism may constitute one of the genetic components underlying insulin secretion, and could explain the genetic predisposition of certain individuals to type 2 diabetes.Citation14
A potential explanation for the association between the deletion allele and diabetes is that impairment of α2B-AR desensitization due to the allelic variant causes prolonged inhibition of insulin secretion from pancreatic beta cells. As insulin sensitivity decreases, the requirement for insulin secretion by beta cells increases, so individuals with an impaired capacity to secrete insulin are predisposed to type 2 diabetes.Citation30,Citation36
An alternative explanation for the association between α2-AR I/D polymorphism and early-onset diabetes is altered function of the autonomic nervous system, particularly regulation of vascular tone. Altered regulation of vascular resistance may influence glucose metabolism, either directly through redistribution of blood flow or through reflex modulation of autonomic nervous system activity.Citation37 Redistribution of blood flow away from metabolically active tissues, striated muscle in particular, caused by any mechanism leading to regional alterations in vascular resistance, would be expected to alter glucose metabolism.Citation30,Citation37
Talmud et al reinforced the notion that the α2-AR pathway should be considered as a potential drug target for prevention of type 2 diabetes. However, an α2-AR antagonist, which might promote insulin secretion and lipolysis, could potentially raise blood pressure, so a drug that does not cross the blood–brain barrier might be required.Citation38
In conclusion, our study shows a strong association between the DD genotype, the D allele, and hypertension and that this association is more evident in patients with hypertension and diabetes. We postulate that the deletion allele is associated with diabetes, so α2B-AR polymorphism is one of the genetic factors involved in the prediction of hypertension, and diabetes and may be considered to be a risk factor. Also, association of the DD genotype with higher atherogenic LDL and lower HDL may potentiate its role in precipitating hypertension.
Disclosure
The authors report no conflicts of interest in this work.
References
- KearneyPMWheltonMReynoldsKMuntnerPWheltonPKHeJGlobal burden of hypertension: analysis of worldwide dataLancet200536521722315652604
- EzzatiMLopezADRodgersAVander HoornSMurrayCJSelected major risk factors and global and regional burden of diseaseLancet20023601347136012423980
- OstchegaYYoonSSHughesJLouisTHypertension Awareness, Treatment, and Control – Continued Disparities in Adults: United States, 2005–2006Hyattsville, MDNational Center for Health Statistics NCHS Data Brief 32008
- SorlieDStaffordRSTuranTNHeart Disease and Stroke Statistics – 2011 Update: a report from the American Heart AssociationCirculation2011123e18e20921160056
- ArafaNASEz-ElarabHSEpidemiology of prehypertension and hypertension among Egyptian adultsThe Egyptian Journal of Community Medicine201129118
- Von WowernFBengtssonKLindbladUFunctional variant in the 2B adrenoceptor gene, a positional candidate on chromosome 2, associates with hypertensionHypertension20044359259714744925
- PertovaaraANoradrenergic pain modulationProg Neurobiol200680538317030082
- ChenQJLuLJinCInsertion/insertion genotype of α2B-adrenergic receptor gene polymorphism is associated with silent myocardial ischemia in patients with type 2 diabetes mellitusClin Biochem2010431201120420692245
- NguyenKKassimatisTLymperopoulosAImpaired desensitization of a human polymorphic a2B-adrenergic receptor variant enhances its sympatho-inhibitory activity in chromaffin cellsCell Commun Signal20119521299895
- BylundDBEikenbergDCHiebleJPIV International Union of Pharmacology nomenclature of adrenoceptorsPharmacol Rev1994461211367938162
- RuffoloRRNicholsAJStadelJMHiebleJPPharmacologic and therapeutic applications of alpha 2-adrenoceptor subtypesAnnu Rev Pharmacol Toxicol1993332432798098595
- PhilippMBredeMHeinLPhysiological significance of alpha(2)-adrenergic receptor subtype diversity: one receptor is not enoughAm J Physiol Regul Integr Comp Physiol2002283R287R29512121839
- LaceyRJChanSLCableHCExpression of alpha 2- and beta-adrenoceptor subtypes in human islets of LangerhansJ Endocrinol19961485315438778232
- SiitonenNLindstromJErikssonJAssociation between a deletion/insertion polymorphism in the alpha2B-adrenergic receptor gene and insulin secretion and type 2 diabetes. The Finnish Diabetes Prevention StudyDiabetologia2004471416142415309292
- PhilippMHeinLAdrenergic receptor knockout mice: distinct functions of 9 receptor subtypesPharmacol Ther2004101657414729393
- Von WowernFBengtssonKLindgrenCMA genome wide scan for early onset primary hypertension in ScandinaviansHum Mol Genet2003122077208112913078
- RiceTRankinenTProvinceMAGenome-wide linkage analysis of systolic and diastolic blood pressure: the Quebec Family StudyCirculation20001021956196311034945
- PerolaMKainulainenKPajukantaPGenome-wide scan of predisposing loci for increased diastolic blood pressure in Finnish siblingsJ Hypertens2000181579158511081770
- KristjanssonKManolescuAKristinssonALinkage of essential hypertension to chromosome 18qHypertension2002391044104912052839
- SuzukiNMatsunagaTNagasumiKα2b-Adrenergic receptor deletion polymorphism associates with autonomic nervous system activity in young healthy JapaneseJ Clin Endocrinol Metab2003881184118712629104
- DornGWAdrenergic signaling polymorphisms and their impact on cardiovascular diseasePhysiol Rev2010901013106220664078
- DuerdenMGBritish Hypertension SocietyGuidelines from the British Hypertension Society: BHS is set to bankrupt NHSBMJ2004329746556957015345637
- GoldsteinDSacksDBrunsDGuidelines and recommendations for laboratory analysis in the diagnosis and management of diabetes mellitusClin Chem20074843647211861436
- WallachJMetabolic and hereditary disordersInterpretation of Diagnostic Tests6th edBoston, MALittle Brown and Company1996
- SirchiaGPizziCScalomognaMA simple procedure for human lymphocyte isolation from peripheral bloodTissue Antigens197272138139
- VasudevanRIsmailPStanslasJShamsudinNAliABAssociation of insertion/deletion polymorphism of alpha-adrenoceptor gene in essential hypertension with or without type 2 diabetes mellitus in Malaysian subjectsInt J Biol Sci2008436236718953403
- PapanasNPapatheodorouKPapazoglouDKotsiouSChristakidisDMaltezosEAn insertion/deletion in the alpha 2B adrenoceptor gene is associated with peripheral neuropathy in patients with type 2 diabetes mellitusExp Clin Endocrinol Diabetes200711532733017516297
- HeinonenPKouluMPesonenUKarvonenMKRissanenALaaksoMIdentification of a three-amino acid deletion in the alpha2B adrenergic receptor that is associated with reduced basal metabolic rate in obese subjectsJ Clin Endocrinol Metab1999842429243310404816
- SiveniusKLindiVNiskanenLLaaksoMUusitupaMEffect of a three amino acid deletion in the alpha2B-adrenergic receptor gene on long term body weight change in Finnish non-diabetic and type 2 diabetic subjectsInt J Obes Relat Metab Disord2001251609161411753579
- PapazoglouDPapanasNPapatheodorouKKotsiouSChristakidisDMaltezosEAn insertion/deletion polymorphism in the alpha2B adrenoceptor gene is associated with age at onset of type 2 diabetes mellitusExp Clin Endocronol Diabetes2006114424427
- SnapirAHeinonenPTuomalainenTPAlhopuroPKarvonenMKLakkaTAAn insertion/deletion polymorphism in the alpha2B-adrenergic receptor gene is a novel genetic risk factor for acute coronary eventsJ Am Coll Cardiol2001371516152211345359
- SiveniusKNiskanenLLaaksoMUusitupaMA deletion in the alpha2B-adrenergic receptor gene and autonomic nervous function in central obesityObes Res20031196297012917501
- LocketteWGhoshSFarrowSAlpha 2-adrenergic receptor gene polymorphism and hypertension in blacksAm J Hypertens199583903947619352
- SnapirAScheininMGroopLCThe insertion/deletion variation in the α2B-adrenoceptor does not seem to modify the risk for acute myocardial infarction, but may modify the risk for hypertension in sib-pairs from families with type 2 diabetesCardiovasc Diabetol200324215
- BaldwinCTSchwartzFBaimaJIdentification of a polymorphic glutamic acid stretch in the alpha2B-adrenergic receptor and lack of linkage with essential hypertensionAm J Hypertens19991285385710509541
- LeRoithDBeta-cell dysfunction and insulin resistance in type 2 diabetes: role of metabolic and genetic abnormalitiesAm J Med20021133S11S12431757
- ClerkLHVincentMALindnerJRClarkMGRattiganSBarrettEJThe vasodilatory actions of insulin on resistance and terminal arterioles and their impact on muscle glucose uptakeDiabetes Metab Res Rev20042031214737741
- TalmudPJCooperJAGauntTVariants of ADRA2A are associated with fasting glucose, blood pressure, body mass index and type 2 diabetes risk: meta-analysis of four prospective studiesDiabetologia2011541710171921455730