
Abstract
Background
As the C-terminal section of vasopressin precursor, copeptin has been recently suggested as a new prognostic biomarker after heart failure (HF). Thus, the aim of this study was to evaluate the prognostic value of plasma copeptin level with all-cause mortality in patients with HF.
Methods
Comprehensive strategies were used to search relevant studies from electronic databases. Pooled hazard ratios (HRs) and standardized mean differences (SMDs) together with their 95% confidence intervals (CIs) were calculated. Subgroup analysis and sensitivity analysis were performed to find the potential sources of heterogeneity.
Results
A total of 5,989 participants from 17 prospective studies were included in this meta-analysis. A significant association was observed between circulating copeptin levels and risk of all-cause mortality in patients with HF (categorical copeptin: HR =1.69, 95% CI =1.42–2.01; per unit copeptin: HR =1.03, 95% CI =1.00–1.07; log unit copeptin: HR =3.26, 95% CI =0.95–11.25). Pooled SMD showed that copeptin levels were significantly higher in patients with HF who died during the follow-up period than in survivors (SMD =1.19, 95% CI =0.81–1.57). Subgroup analyses also confirmed this significant association, while sensitivity analyses indicated that the overall results were stable.
Conclusion
This study demonstrated that circulating copeptin seemed to be a novel biomarker to provide better prediction of all-cause mortality in patients with HF.
Introduction
As the terminal stage of all kinds of cardiovascular diseases, including hypertension, myocardial infarction (MI) and cardiomyopathy, heart failure (HF) is known as one of the leading burdens to the health care system not only for cost but also for morbidity and mortality all over the world.Citation1 According to the estimation of the US Centers for Disease Control and Prevention, the total cost of treatment for HF was up to ≥34 billion in 2010.Citation2 Furthermore, mortality rates in patients with HF were even similar to the 5-year mortality rates of some most severe cancers, which were up to 50%.Citation3
Copeptin, which was first discovered in 1972, is located in the C-terminal section of the arginine vasopressin (AVP) precursor (pro-AVP) and consists of 39 amino acid glycopeptides.Citation4 Evidence demonstrated that copeptin is released from pro-AVP together and equivalent with AVP. AVP is widely known as a vital hormone with numerous effects in the human body, such as central nervous, hemodynamic, hemostatic and endocrinologic effects.Citation5 Plasma AVP levels increase apparently during the process of some acute and chronic diseases, and the measurement of AVP would be useful for the diagnosis of patients.Citation6 However, because of the pulse release mode and the short half-life of AVP, the clinical application of AVP is restricted.Citation7 Recently, as a result of the long-term stability and being easy to measure, copeptin has been used as an alternative marker of AVP and suggested as a biomarker for poor clinical outcome and mortality of some diseases, such as pneumonia,Citation8 MI,Citation9 diabetes,Citation10,Citation11 HF,Citation12 strokeCitation13 and transient ischemic attack.Citation14,Citation15
In the current study, we performed a systematic review and meta-analysis aimed to assess the prognostic value of circulating copeptin levels for all-cause mortality in patients with HF.
Methods
We used comprehensive electronic literature databases to search for potential studies that estimated the prognostic value of copeptin in patients with HF. The current study was conducted according to the Meta-analysis of Observational Studies in Epidemiology (MOOSE) checklist.Citation16
Electronic literature databases (PubMed, the Web of Science, EMBASE, Cochrane Collaboration Databases, Medline, Chinese National Knowledge Infrastructure, Wan Fang Database and Chong Qing VIP Database) were searched for relevant studies published up to October 2016 without restrictions of the type of document and language. The following search terms were used: (“heart failure” OR “HF” OR “cardiac dysfunction”) and (“copeptin” OR “C-terminal provasopressin” OR “CT-pro-AVP”). Moreover, we also searched the references of the selected articles and textbooks manually as a source of related studies.
Two reviewers (PZ and GL) selected the relevant articles according to the inclusion criteria independently. Studies included in this meta-analysis should satisfy the following criteria: 1) adult patients with HF; 2) prospective studies that estimated the association between copeptin and all-cause mortality risk in patients with HF and 3) studies that reported the description of risk estimation of the relative risks (RRs) or hazard ratios (HRs) together with their corresponding 95% confidence intervals (CIs) or provided mean differences of copeptin in survivors and non-survivors. For studies on the same population or overlapping data, only the one with the largest number of subjects was included.
Information of all involved studies was carefully extracted by two reviewers (PZ and XW) independently, and any disagreement was settled by other reviewers (GL and HS). The following information was extracted from all the eligible studies: first author’s name, publication year, country, number of centers, type of patients, follow-up period, sample size (including number of survivors and non-survivors), mean age, baseline copeptin levels, type of copeptin measurement, RRs or HRs together with their 95% CIs and mean copeptin levels with standard deviations (SDs); if not reported, median copeptin levels with interquartile ranges (IQRs) were used.
According to the Newcastle–Ottawa Quality Assessment Scale (NOS),Citation17 two reviewers (PZ and HS) assessed the methodological quality of each eligible study independently. Disagreements were resolved from discussion with other reviewers (GL and XW). The following three aspects were used to assess the quality of cohort studies: the selection of participants, the comparability of the exposed and unexposed cohort and the assessment of the outcome. The total scores of each study ranged between 0 and 9, and studies achieving scores >6 were regarded as high quality.
According to the different reporting forms of copeptin, we separately performed three meta-analyses for the risk estimation between copeptin and all-cause mortality in patients with HF based on unit copeptin, logarithm of copeptin, and copeptin categories, respectively. For the studies that reported the categorical data, we used the RRs (or HRs) between highest and lowest categories of copeptin. When both multivariate and univariate results were available, the former was preferred in the current analysis. Furthermore, for the studies that reported RRs, the RRs were regarded as HRs directly, as pooled HRs were used for all the risk estimations.
Based on the strength of association between copeptin and all-cause mortality in patients with HF, pooled standardized mean differences (SMDs) were estimated according to the mean copeptin levels ± SDs reported in the studies. For studies in which the mean copeptin levels ± SDs were unavailable, medians were treated as mean values directly and IQRs were used to estimate the SDs using the following formula: SD = IQR/1.35.Citation18
I2 test was used for testing the heterogeneity among different studies.Citation19 I2>50% was considered as a sign of high heterogeneity using random-effects model. Otherwise, the fixed-effects model was used.Citation20 Subgroup analyses were performed to find the potential sources of heterogeneity, on the basis of sample size, age, female percentage, baseline copeptin, number of centers, type of HF (acute or chronic), measurement methods of copeptin, quality of studies and follow-up period.
Test for funnel plot asymmetry was conducted when at least 10 studies were included. Only six studies were included in our analyses for HR estimation by copeptin categories and unit copeptin, therefore the potential publication bias was not assessed. Sensitivity analysis was conducted by removing one study each time. P<0.05 was regarded as statistically significant, and all statistical analyses were performed using the STATA 12.0 (Stata, College Station, TX, USA).
Results
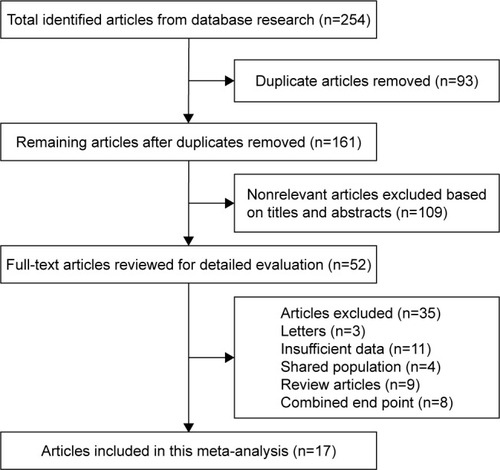
A detailed description of the process of study selection is shown in . At first, 254 potential articles were identified from the databases searching, and only 161 articles remained after removing the duplicate studies. After assessing based on the title and abstract, 109 irrelevant studies were excluded. Finally, a total of 52 articles were fully reviewed, and 17 prospective studies providing data for 5,989 participants met the inclusion criteria and were included in the current meta-analysis.
Figure 1 Flowchart of study selection and exclusion process.
The main characteristics of the included studies are listed in . The mean follow-up period ranged from 14 days to 13 years, while the sample size ranged from 40 to 1,237. The detailed scores of included studies are listed in . A total of 14 studies reported RRs or HRs with 95% CIs for the risk estimation between baseline copeptin level and all-cause mortality in patients with HF, 11 out of these 14 studies reported results from multivariate regression analyses and the other three studies reported results from univariate regression analyses only. As for the evaluation of the strength, three out of nine studies provided the mean copeptin levels with SDs, while the remaining six studies provided median copeptin levels with IQRs only.
Table 1 Main characteristics of included studies
Table 2 The scores of included studies assessed by NOS
Six studies including 2,913 patients with HF reported the risk estimation according to copeptin categories. No evidence of heterogeneity was observed (I2=45.4%, P=0.103), and the fixed-effects model was used in this meta-analysis. The pooled HR was 1.69 (95% CI =1.42–2.01; ). shows the detailed information of subgroup analyses by copeptin categories, and the significant association between copeptin and all-cause mortality in patients with HF was also confirmed in each subgroup.
Figure 2 Pooled estimate of HR of all-cause mortality with copeptin in patients with HF.
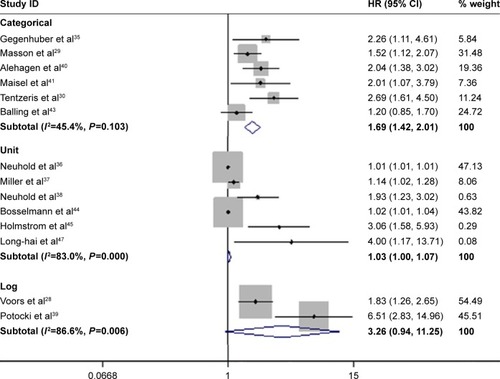
Table 3 Pooled HRs of all-cause mortality by copeptin levels in subgroup analyses
Six studies reported the RRs or HRs with 95% CIs for the risk estimation of all-cause mortality in patients with HF by unit copeptin. A total of 1,769 participants were included in this meta-analysis, and a significant heterogeneity among studies was observed (I2=83.0%, P<0.001). Using the random-effects model, the pooled HR of all-cause mortality was 1.03 (95% CI =1.00–1.07; ). As presented in , a few subgroups by unit copeptin corroborated this association between copeptin and all-cause mortality in patients with HF, even though other subgroups showed a borderline association, such as the higher mortality group (≥30%) and the younger age group (<70).
The other two studies reported the risk estimation by log copeptin, and the pooled HR was 3.26 (95% CI =0.95–11.25; ) using a random-effects model (I2=86.6%, P<0.001). Subgroup analyses according to log copeptin were not conducted, as the number of original studies was relatively small.
Based on the pooled SMD, nine studies provided data for 630 deaths and 2,152 survivors were included in this meta-analysis. Obvious heterogeneity between studies was observed (I2=92.1%, P<0.001), and the random-effects model was chosen. The result of the pooled SMD (1.19, 95% CI =0.81–1.57; ) showed that baseline copeptin levels were significantly higher in patients who died during the follow-up period than survivors, indicating that higher circulating copeptin levels were positively associated with the risk of all-cause mortality in patients with HF. The results of subgroup analyses are presented in , and the significant association was also observed in each subgroup.
Figure 3 Pooled estimate of standardized mean copeptin value with all-cause mortality in patients with HF.
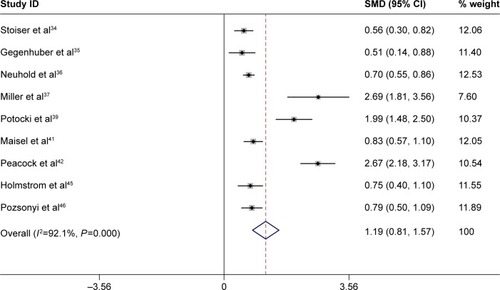
Table 4 Pooled SMDs in subgroup analyses
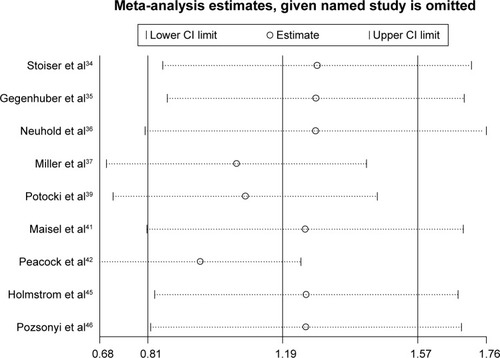
Sensitivity analyses were conducted by removing one study at a time to observe the influence of each included study on the overall pooled estimates. As shown in , no single study was observed to significantly influence the overall pooled estimates, which indicated that our overall results were statistically stable.
Figure 4 Sensitivity analysis of included studies (on SMD).
Discussion
AVP, also called antidiuretic hormone, was produced by the hypothalamus and secreted from the neurohypophysis in reaction to osmotic and hemodynamic stimuli.Citation21 When released into the blood flow, AVP began to take different peripheral effects through three different receptors, namely V1a, V1b, and V2, respectively. In patients with HF, increased AVP contributed to the process of left ventricular dysfunction, by activating V1a and V2 receptors and making further effects such as leading to water retention, peripheral vasoconstriction, and myocardial remodeling.Citation22 Generally, plasma AVP level increased sharply in patients with HF and was relevant to the severity of disease.Citation23 Thus, knowledge of circulating AVP levels would be of vital importance to the diagnosis and assessment of therapeutic intervention with HF. However, due to the shortages of the half-time of 24 minutes, unstability in frozen plasma and difficult measurement method, the clinical use of AVP for HF was restricted.Citation24,Citation25
Copeptin, also named the AVP-associated glycopeptides, was derived from pro-AVP together with AVP, neurophysin II and a signal peptide.Citation26 Different from AVP, copeptin was discovered to be stable even at room temperature and easily measured by sandwich immunoassay, with results stable in 20–60 minutes.Citation27 In recent years, despite the exact mechanism connecting copeptin with the severity of HF not clear, the clinical use of copeptin as a surrogate marker of AVP was proposed. Early studies had indicated that a higher circulating copeptin level was an independent prognostic factor not only for mortality but also for poor functional outcome in patients with HF.Citation28,Citation29 These multiple studies in different clinical settings showed that circulating copeptin levels were necessary for risk stratification in patients with HF.Citation30,Citation31
A previous research conducted by Sun et alCitation32 suggested that copeptin was a prognostic biomarker for all-cause mortality in patients with cardio-cerebrovascular disease. However, comprehensive study about the prognostic role of copeptin in patients with HF was not reported. To our best knowledge, this was the first systematic review and meta-analysis attempting to evaluate the prognostic value of copeptin and all-cause mortality in patients with HF. Through this collaborative meta-analysis, our study provided new and powerful evidence to the suggestion of using copeptin as an independent prognostic biomarker for risk stratification in patients with HF.
Our results showed that higher circulating copeptin levels at baseline were significantly associated with the increased risk of all-cause death in patients with HF, with a pooled SMD (difference of mean copeptin level between death group and survival group/pooled SD) of 1.19. Overall, the risk of death from all causes in patients with HF increased 3% for per unit (1 pmol/L) increase in baseline copeptin level and >200% for 10-fold copeptin increase. Meanwhile, compared to the group with lower copeptin level, the patients with HF with higher circulating copeptin levels were at a 1.69 times higher risk from all-cause death. Subgroup analyses also presented several important findings. In the subgroup analysis based on mortality and female percentage, the lower mortality group (<30%) revealed a more prominent association as well as the higher female proportion group (≥30%). Furthermore, when analyzing according to the sample size, a more extrusive association was found in studies with subjects <200 compared to studies with subjects ≥200. As small studies with limited sample sizes were more likely to report larger beneficial effects,Citation33 multicenter studies with large sample size were desired to evaluate a more accurate estimate about the association between copeptin and all-cause mortality in patients with HF.
Although some credible findings have been achieved, some limitations of our meta-analysis should be declared in this article. First, we restricted our study to all-cause mortality rather than HF related morbidity or mortality, which might show different relationship with copeptin. Second, we did not extract the original data from the eligible studies, which restricts further statistical estimate of circulating copeptin levels in the evaluation of the prognostic accuracy in the receiver operating characteristic curve after HF. Third, merely crude RR (HR) could be achieved from some included studies. Therefore, the confounding factors of the different studies could not be adequately accounted for in the current analysis. Finally, publication bias might be a key element, for negative studies seemed to be more difficult to publish and have less impact; thus, the insufficiency of negative studies might influence the results of our meta-analyses.Citation13
Conclusion
The results of our study indicated a prognostic role of copeptin that higher circulating copeptin levels were positively associated with the risk of all-cause mortality in patients with HF. Thus, in patients with HF, we recommended using copeptin as a new prognostic biomarker to provide better information not only in decision making for treatment but also in the prediction of clinical outcome. Since the exact mechanism of this association between copeptin and mortality in patients with HF is not fully understood, future well-designed studies with large sample size are required.
Acknowledgments
The authors highly appreciate the support from all the participants.
Disclosure
The authors report no conflicts of interest in this work.
References
- MozaffarianDBenjaminEJGoASHeart Disease and Stroke Statistics-2016 Update: a Report From the American Heart AssociationCirculation20161334e38e6026673558
- ChowdhuryPKehlDChoudharyRMaiselAThe use of biomarkers in the patient with heart failureCurr Cardiol Rep201315637223644993
- BallingLGustafssonFCopeptin as a biomarker in heart failureBiomark Med20148684185425224940
- HolwerdaDAA glycopeptide from the posterior lobe of pig pituitaries. I. Isolation and characterizationEur J Biochem19722833343395079944
- DunserMWWenzelVMayrAJHasibederWRManagement of vasodilatory shock: defining the role of arginine vasopressinDrugs200363323725612534330
- ZhangRLiuJZhangYLiuQLiTChengLAssociation between circulating copeptin level and mortality risk in patients with intracerebral hemorrhage: a systemic review and meta-analysisMol Neurobiol Epub201615
- BolignanoDCabassiAFiaccadoriECopeptin (CTproAVP), a new tool for understanding the role of vasopressin in pathophysiologyClin Chem Lab Med201452101447145624940718
- ViasusDDel Rio-PertuzGSimonettiAFBiomarkers for predicting short-term mortality in community-acquired pneumonia: a systematic review and meta-analysisJ Infect201672327328226777314
- RaskovalovaTTwerenboldRCollinsonPODiagnostic accuracy of combined cardiac troponin and copeptin assessment for early rule-out of myocardial infarction: a systematic review and meta-analysisEur Heart J Acute Cardiovasc Care201431182724562800
- TheiladeSRosenlundSHansenTWGotzeJPerssonFRossingPIncreased copeptin in plasma predicts mortality and renal outcome in patients with type 1 diabetesDiabetologia201558S541S542
- ThenCKowallBLechnerAPlasma copeptin is associated with type 2 diabetes in men but not in women in the population-based KORA F4 studyActa Diabetol201552110311225011650
- RamalhoAASilvaDCortez-DiasNCopeptin predicts long term prognosis in patients with worsening heart failureEur J Heart Fail201416276
- ChoiKSKimHJChunHJPrognostic role of copeptin after stroke: a systematic review and meta-analysis of observational studiesSci Rep201551166526119473
- De MarchisGMKatanMWeckACopeptin and risk stratification in patients with ischemic stroke and transient ischemic attack: the CoRisk studyInt J Stroke20138321421822336226
- PurroyFSuarezICambraySFarreJSanahujaJBenabdelhakICopeptin improves the prognostic models of early subsequent stroke after a transient ischemic attackInt J Stroke20151025124206581
- StroupDFBerlinJAMortonSCMeta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of Observational Studies in Epidemiology (MOOSE) groupJAMA2000283152008201210789670
- StangACritical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analysesEur J Epidemiol201025960360520652370
- HigginsJPGreenSCochrane Handbook for Systematic Review of Interventions, Version 5.1.0CopenhagenThe Nordic Cochrane Center20112011
- HigginsJPThompsonSGDeeksJJAltmanDGMeasuring inconsistency in meta-analysesBMJ2003327741455756012958120
- DerSimonianRLairdNMeta-analysis in clinical trialsControl Clin Trials1986731771883802833
- MorgenthalerNGStruckJJochbergerSDunserMWCopeptin: clinical use of a new biomarkerTrends Endocrinol Metab2008192434918291667
- Serradeil-Le GalCWagnonJValetteGNonpeptide vasopressin receptor antagonists: development of selective and orally active V1a, V2 and V1b receptor ligandsProg Brain Res200213919721012436936
- ChatterjeeKNeurohormonal activation in congestive heart failure and the role of vasopressinAm J Cardiol2005959A8B13B15619386
- BaumannGDingmanJFDistribution, blood transport, and degradation of antidiuretic hormone in manJ Clin Invest1976575110911161262458
- RobertsonGLMahrEAAtharSSinhaTDevelopment and clinical application of a new method for the radioimmunoassay of arginine vasopressin in human plasmaJ Clin Invest1973529234023524727463
- JernbergTStridsbergMLindahlBUsefulness of plasma N-terminal proatrial natriuretic peptide (proANP) as an early predictor of outcome in unstable angina pectoris or non-ST-elevation acute myocardial infarctionAm J Cardiol2002891646611779526
- NickelCHBingisserRMorgenthalerNGThe role of copeptin as a diagnostic and prognostic biomarker for risk stratification in the emergency departmentBMC Med201210722264220
- VoorsAAvon HaehlingSAnkerSDC-terminal provasopressin (copeptin) is a strong prognostic marker in patients with heart failure after an acute myocardial infarction: results from the OPTIMAAL studyEur Heart J200930101187119419346228
- MassonSLatiniRCarbonieriEThe predictive value of stable precursor fragments of vasoactive peptides in patients with chronic heart failure: data from the GISSI-heart failure (GISSI-HF) trialEur J Heart Fail201012433834720097683
- TentzerisIJaraiRFarhanSComplementary role of copeptin and high-sensitivity troponin in predicting outcome in patients with stable chronic heart failureEur J Heart Fail201113772673321616953
- MillerWLGrillDEStruckJJaffeASAssociation of hyponatremia and elevated copeptin with death and need for transplantation in ambulatory patients with chronic heart failureAm J Cardiol2013111688088523276468
- SunHSunTMaBPrediction of all-cause mortality with copeptin in cardio-cerebrovascular patients: a meta-analysis of prospective studiesPeptides20156991825849342
- ZhangZXuXNiHSmall studies may overestimate the effect sizes in critical care meta-analyses: a meta-epidemiological studyCrit Care2013171R223302257
- StoiserBMortlDHulsmannMCopeptin, a fragment of the vasopressin precursor, as a novel predictor of outcome in heart failureEur J Clin Invest2006361177177817032344
- GegenhuberAStruckJDieplingerBComparative evaluation of B-type natriuretic peptide, mid-regional pro-A-type natriuretic peptide, mid-regional pro-adrenomedullin, and copeptin to predict 1-year mortality in patients with acute destabilized heart failureJ Card Fail2007131424917339002
- NeuholdSHuelsmannMStrunkGComparison of copeptin, B-type natriuretic peptide, and amino-terminal pro-B-type natriuretic peptide in patients with chronic heart failure: prediction of death at different stages of the diseaseJ Am Coll Cardiol200852426627218634981
- MillerWLHartmanKAHodgeDOResponse of novel biomarkers to BNP infusion in patients with decompensated heart failure: a multimarker paradigmJ Cardiovasc Transl Res20092452653520560012
- NeuholdSHuelsmannMStrunkGPrognostic value of emerging neurohormones in chronic heart failure during optimization of heart failure-specific therapyClin Chem201056112112619884490
- PotockiMBreidthardtTMuellerACopeptin and risk stratification in patients with acute dyspneaCrit Care2010146R21321106053
- AlehagenUDahlstromURehfeldJFGoetzeJPAssociation of copeptin and N-terminal proBNP concentrations with risk of cardiovascular death in older patients with symptoms of heart failureJAMA2011305202088209521610241
- MaiselAXueYShahKIncreased 90-day mortality in patients with acute heart failure with elevated copeptin secondary results from the biomarkers in acute heart failure (BACH) studyCirc Heart Fail20114561362021765124
- PeacockWFNowakRChristensonRShort-term mortality risk in emergency department acute heart failureAcad Emerg Med201118994795821906204
- BallingLKistorpCSchouMPlasma copeptin levels and prediction of outcome in heart failure outpatients: relation to hyponatremia and loop diuretic dosesJ Card Fail201218535135822555263
- BosselmannHEgstrupMRossingKPrognostic significance of cardiovascular biomarkers and renal dysfunction in outpatients with systolic heart failure: a long term follow-up studyInt J Cardiol2013170220220724182673
- HolmstromASigurjonsdottirRHammarstenOPetzoldMGustafssonDFuMLXAn integrated multiple marker modality is superior to NT-proBNP alone in prognostic prediction in all-cause mortality in a prospective cohort of elderly heart failure patientsEur Geriatr Med201346365371
- PozsonyiZForheczZGombosTKaradiIJanoskutiLProhaszkaZCopeptin (C-terminal pro arginine-vasopressin) is an independent long-term prognostic marker in heart failure with reduced ejection fractionHeart Lung Circ201524435936725618448
- Long-haiWQi-songCFangXIAChaoFHai-junHEPingZPrognostic value of copeptin, big endothelin-1 and N-terminal pro-brain natriuretic peptide in patients with chronic heart failureMod Lab Med2015301646771