
Abstract
Purpose
To determine the predictive values of D-dimer assay, Global Registry of Acute Coronary Events (GRACE) and Thrombolysis in Myocardial Infarction (TIMI) risk scores for adverse outcome in patients with non-ST-segment elevation myocardial infarction (NSTEMI).
Patients and methods
A total of 234 patients (mean age: 57.2±11.7 years, 75.2% were males) hospitalized with NSTEMI were included. Data on D-dimer assay, GRACE and TIMI risk scores were recorded. Logistic regression analysis was conducted to determine the risk factors predicting increased mortality.
Results
Median D-dimer levels were 349.5 (48.0–7,210.0) ng/mL, the average TIMI score was 3.2±1.2 and the GRACE score was 90.4±27.6 with high GRACE scores (>118) in 17.5% of patients. The GRACE score was correlated positively with both the D-dimer assay (r=0.215, P=0.01) and TIMI scores (r=0.504, P=0.000). Multivariate logistic regression analysis revealed that higher creatinine levels (odds ratio =18.465, 95% confidence interval: 1.059–322.084, P=0.046) constituted the only significant predictor of increased mortality risk with no predictive values for age, D-dimer assay, ejection fraction, glucose, hemoglobin A1c, sodium, albumin or total cholesterol levels for mortality.
Conclusion
Serum creatinine levels constituted the sole independent determinant of mortality risk, with no significant values for D-dimer assay, GRACE or TIMI scores for predicting the risk of mortality in NSTEMI patients.
Introduction
Acute coronary syndrome (ACS) is characterized by a spectrum of distinct clinical entities with a common etiology that ranges from unstable angina (UA) to non-ST-segment elevation myocardial infarction (NSTEMI) and ST-segment elevation myocardial infarction depending on the severity.Citation1,Citation2 Despite advances in coronary intervention techniques and equipment, ACS has still been associated with high morbidity and mortality rates.Citation3 This necessitates the use of guideline-recommended clinical risk score calculations for identifying life-threatening adverse cardiac outcomes, particularly in NSTEMI and UA patients, and for determining appropriate treatment and follow-up strategies.Citation4–Citation6
The term “NSTEMI patients” refers to a heterogeneous population of ACS with varying short- and long-term mortality and recurrent adverse cardiac events, emphasizing the crucial role of early risk stratification in these patients.Citation6–Citation8
Thrombolysis in Myocardial Infarction (TIMI)Citation9 risk scores and Global Registry of Acute Coronary Events (GRACE)Citation10 risk scores are amongst the most commonly used risk scores used to enable early risk stratification upon a patient’s admission to a hospital. They are derived from databases from the comprehensive clinical trials involving NSTE-ACS or the entire spectrum of ACS, respectively.Citation6,Citation8–Citation10 The GRACE risk score is the most extensively validated and studied score that is indicated for predicting the risk of ischemic events and that is associated with prognosis in ACS.Citation8,Citation11
Owing to the acute thrombotic occlusion of coronary arteries in the etiology of ACS, and thus ongoing thrombosis in the coronary vessels that consumes platelets and clotting factors,Citation1,Citation4,Citation12,Citation13 D-dimer level, a marker of cross-linked fibrin turnover, has been associated with ischemic heart diseases, with increased levels shown in patients with ACS.Citation13,Citation14
This cross-sectional study was aimed at determining the predictive values of D-dimer assay, GRACE and TIMI scores for adverse outcome in patients with NSTEMI.
Patients and methods
Study population
A total of 234 patients (mean [standard deviation; SD] age: 57.2 [11.7] years, 75.2% were males) hospitalized with the diagnosis of NSTEMI upon their admission to emergency service with chest pain were included in this cross-sectional prospective study conducted at Mehmet Akif Ersoy Thoracic and Cardiovascular Surgery Training and Research Hospital between June 2014 and December 2014. Patients who had acute aortic dissection, known malignancy, venous thromboembolism, pulmonary embolism and chronic kidney failure and who were on erythropoietin therapy were excluded from the study.
Written informed consent was obtained from each subject following a detailed explanation of the objectives and protocol of the study, which was conducted in accordance with the ethical principles stated in the Declaration of Helsinki and approved by the Mehmet Akif Ersoy Thoracic and Cardiovascular Surgery Training and Research Hospital Research Ethics Committee (date of approval: 06/01/2011; protocol number: 46).
Assessments
Data on demographics (age, sex), smoking status, diabetes history, previous cardiac interventions, current infarct type and treatment approach (coronary artery bypass grafting [CABG], percutaneous coronary intervention [PCI], medical treatment), the use of acetylsalicylic acid in the last week, pain in the last 24 h, vital signs (heart rate [beats per minute, or bpm], diastolic and systolic blood pressure [BP]), routine blood biochemistry and hemogram analysis, and D-dimer assay, GRACE and TIMI risk scores were recorded for each patient at the time of hospitalization. Patients were diagnosed with hypertension, with systolic BP ≥140 mmHg and diastolic BP ≥90 mmHg, or they were under treatment with antihypertensive medications. Diabetes was defined as a state with a fasting plasma sugar level ≥126 mg/dL, a random glucose level ≥200 mg/dL or the ongoing treatment of diabetes.Citation15,Citation16 Cardiac death was evaluated during 14-month follow-up. The relation of D-dimer levels with GRACE and TIMI risk scores was analyzed. Demographic and laboratory parameters were evaluated with respect to GRACE scores (high vs low) and outcome (survivors vs non-survivors). Logistic regression analysis was conducted to determine the risk factors predicting high GRACE scores and mortality.
Diagnosis of acute NSTEMI
NSTEMI was defined by electrocardiographic prominent T-wave inversion and/or the positive biomarkers of necrosis (eg, troponin, CK-MB) in the absence of ST-segment elevation and in an appropriate clinical setting (an anginal equivalent or chest discomfort).Citation17
Calculation of GRACE risk score
The GRACE risk score was calculated based on age, heart rate, systolic BP, baseline creatinine level, history of congestive heart failure, in-hospital PCI, history of MI, ST-segment depression on admission electrocardiography (ECG) and elevated cardiac enzyme or marker levels.Citation10,Citation18 Plasma 99th percentile reference limits for T troponin (ng/mL) were used in consideration of the elevated cardiac marker. ST-segment depression was defined as decreased ST segment: 0.5 mV below the isoelectric line in any ECG lead. To examine the adverse outcome for different ranges of the GRACE score, patients were divided into two subgroups: one for low GRACE risk score (≤118) and the other for high GRACE risk score (>118).
Calculation of TIMI score
The TIMI risk score was calculated based on seven independent risk factors for UA/NSTEMI, including age >65 years, ≥3 coronary artery disease (CAD) risk factors, documented CAD at catheterization (>50% stenosis), ST-segment deviation >0.5 mm, ≥2 angina episodes in the prior 24 h, aspirin within the prior week and elevated cardiac biomarkers.Citation9
D-dimer assay
Serum D-dimer levels were measured via particle-enhanced immunoturbidimetric methods using commercial kits (Roche Diagnostics, Mannheim, Germany) with the aid of a Roche Cobas 6000 c501 analyzer (Roche Diagnostics) based on a reference range of <500 ng/mL.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics (IBM Corp. Released 2012, IBM SPSS Statistics for Windows, version 21.0. Armonk, NY: IBM Corp). A chi-square test was used for the comparison of categorical variables, whereas numeric variables were analyzed using the independent samples t-test. Correlation analysis was performed via Pearson’s correlation analysis. Logistic regression analysis was performed for the determinants of risk for a high GRACE score and mortality using the enter method. Data were expressed as “mean (SD)”, minimum–maximum and n (%), where appropriate. P<0.05 was considered statistically significant.
Results
Demographic and clinical characteristics and laboratory findings
Active smoking was noted in 46.2% of patients, and diabetes mellitus was evident in 47.9%. The majority (80.3%) of patients had no history of previous cardiac intervention, whereas multi-vessel disease was evident during hospitalization in 57.7% of patients and was treated with PCI (44.4%), CABG (20.1%) and medical group (35.5%). After 14-month of follow-up, mortality occurred in 11 (4.7%) patients ().
Table 1 Demographic and clinical characteristics and laboratory findings
The data on routine blood biochemistry findings are summarized in . Median D-dimer levels were 349.5 (48.0–7,210.0) ng/mL, the average TIMI score was 3.2 (1.2) and the GRACE score was 90.4 (27.6) with the identification of high GRACE scores (>118) in 17.5% of patients ().
Correlation among D-dimer assay, GRACE and TIMI scores
The GRACE score was correlated positively with both D-dimer assay (r=0.215, P=0.01) and TIMI scores (r=0.504, P=0.000). D-dimer assay and TIMI scores were also positively correlated (r=0.253, P=0.000) ().
Table 2 Correlation between D-dimer, GRACE and TIMI scores
Demographic and laboratory parameters in patients with high vs low GRACE scores
More high than low GRACE scores were associated with older age (72.2 [6.5] years vs 54.1 [10.0] years, P=0.000), a higher percentage of non-smokers (43.9% vs 24.4%, P=0.038), a higher mean D-dimer assay (1,157.7 [1,537.7] ng/mL vs 572.4 [865.3] ng/mL, P=0.001), higher TIMI scores (4.1 [1.2] vs 2.9 [1.1], P<0.001) and higher levels for heart rate (86.5 [23.9] bpm vs 75.5 [16.3] bpm, P=0.000) and creatinine levels (1.0 [0.3] mg/dL vs 0.9 [0.2] mg/dL, P=0.002), as opposed to a lower diastolic BP (74.7 [14.5] mmHg vs 81.4 [14.2] mmHg, P=0.011) as well as lower albumin (3.9 [0.4] g/dL vs 4.3 [0.3] g/dL, P=0.000), triglyceride (147.7 [115.3] mg/dL vs 232.0 [177.0] mg/dL, P=0.033) and hematocrit levels (39.1 [5.6]% vs 43.9 [5.2]%, P=0.000) ().
Table 3 Demographic and laboratory parameters in patients with high vs low GRACE scores
Demographic and laboratory parameters in survivors vs non-survivors
After an average of 15.4 and 14.8 months of follow-up, respectively, more non-survivors than survivors had older age (64.3 [8.5] years vs 56.9 [11.8] years, P=0.041) and higher levels recorded for D-dimer assay (1,568.1 [1,489.0] ng/mL vs 632.5 [995.4] ng/mL, P=0.003), glucose (242.5 [249.1] mg/dL vs 144.6 [68.9] mg/dL, P=0.000), hemoglobin A1c (HbA1c) (8.1 [3.9]% vs 6.6 [1.6]%, P=0.006) and creatinine (1.2 [0.3] mg/dL vs 0.9 [0.3] mg/dL, P=0.000), whereas they had lower levels recorded for the ejection fraction (44.5 [13.6]% vs 53.5 [10.0]%, P=0.007), albumin (3.8 [0.5] g/dL vs 4.2 [0.4] g/dL, P=0.001) and total cholesterol (161.1 [39.9] mg/dL vs 201.1 [47.6] mg/dL, P=0.010). No difference was noted between survivors and non-survivors with respect to GRACE and TIMI scores ().
Table 4 Demographic and laboratory parameters in survivors vs non-survivors
Logistic regression analysis for risk factors predicting mortality
Multivariate logistic regression analysis revealed that higher creatinine levels (odds ratio =18.465, 95% confidence interval [CI]: 1.059–322.084, P=0.046) constituted the only significant predictor of increased mortality risk with no predictive values for age, D-dimer assay, ejection fraction, glucose, HbA1c, sodium, albumin or total cholesterol levels for mortality ().
Table 5 Logistic regression analysis for risk factors predicting mortality
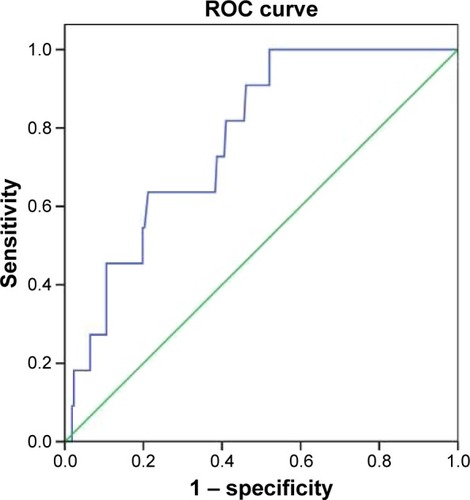
In a receiver operating characteristic (ROC) curve analysis, the area under the ROC curve for D-dimer assay to discriminate non-survivors from survivors in NSTEMI was 0.77 (95% CI: 0.66–0.88, P=0.002), and the optimal cutoff value was 648 ng/mL. Sensitivity and specificity with a cutoff value of 648 ng/mL were 64% and 79%, respectively ().
Figure 1 Receiver operating characteristic (ROC) curve analysis for area under ROC curve and optimal cutoff value of D-dimer to discriminate non-survivors from survivors in non-ST-segment elevation myocardial infarction.
Discussion
Our findings in a cohort of NSTEMI patients composed predominantly of males and patients with no history of previous coronary intervention revealed the diagnosis of multi-vessel disease (57.7%), the implementation of PCI/CABG (60.0%) during hospitalization in most of the patients and a mortality rate of 4.7% within an average of 14.8 months post-discharge. Older age, higher D-dimer assay and creatinine levels, and lower albumin levels were associated with both higher GRACE scores and mortality risk in the univariate analysis, whereas, except for the creatinine levels that predicted increased mortality per se, none of them was found to be a significant determinant of mortality risk in the multivariate analysis.
Amongst the variables associated with non-survivors in the univariate analysis (older age, higher levels for D-dimer assay, glucose, HbA1c and creatinine, and lower levels for the ejection fraction, albumin and total cholesterol), only higher creatinine levels predicted the increased risk for mortality in our cohort. This seems consistent with data on the prognostic importance of an elevated initial serum creatinine upon admission and the independent predictive values of renal impairment for higher in-hospital and short-term mortality among ACS patients, regardless of the subset, that were reported in past studies.Citation19–Citation22
Older age, poor glycemic control, a low ejection fraction and hypoalbuminemia along with high serum creatinine were found to be more common among non-survivors than survivors based on univariate analysis in our cohort. This seems consistent with data from past studies indicating a higher likelihood of renal impairment among older patients with comorbid hypertension, diabetes mellitus and cardiac failure, along with a stronger predictive value of even mild renal impairment for mortality and adverse cardiovascular outcome in ACS patients with left ventricular impairment.Citation20–Citation23
The predictive value of the GRACE risk score has been validated in NSTEMI by several long-term studies,Citation6,Citation8,Citation20,Citation23,Citation24 although it has also been shown that the GRACE risk score accurately discriminates survivors from non-survivors over the longer term in all subsets of ACS patients.Citation6,Citation18,Citation20,Citation25,Citation26 However, although high D-dimer levels, older age, high creatinine levels and low albumin levels were commonly noted in patients with high GRACE scores, as well as among non-survivors, no significant difference was noted between non-survivors and survivors with respect to GRACE scores in our cohort.
More females than males were reported to have a higher likelihood of presenting with atypical symptoms and more unfavorable baseline characteristics, such as higher GRACE scores, older age, a lower ejection fraction, a higher rate of heart failure, hypertension, diabetes and renal dysfunction upon admission, as associated with worse prognosis of ACS and a higher mortality rate among females.Citation27–Citation29 Hence, it is worth noting that, despite male predominance, no sex influence was noted on GRACE scores or mortality risk in our cohort.
D-dimer levels, which were positively correlated with both GRACE and TIMI scores, were significantly higher in patients with high GRACE scores and in non-survivors, along with the optimal cutoff value of 648 ng/mL identified for discriminating non-survivors from survivors in our cohort. Accordingly, the significantly higher levels of D-dimer reported in ACS patients than in the controls have been indicated to reflect the pro-coagulant state associated independently with recurrent coronary events in past studies.Citation13,Citation14,Citation30 Thus, although our findings on univariate analysis support the potential role of D-dimer assay in diagnosis, risk stratification and all-cause mortality risk prediction among ACS patients,Citation14,Citation31,Citation32 multivariate analysis revealed no predictive value of D-dimer assay either for a high GRACE score or mortality risk in our cohort of NSTEMI patients.
The TIMI scores were correlated positively with both D-dimer levels and GRACE scores, whereas they did not differ between non-survivors and survivors and had no predictive value for higher GRACE scores or increased mortality risk. This seems consistent with the association of TIMI scores with the lowest discriminatory accuracy to predict death as compared with the GRACE and Platelet glycoprotein IIb/IIIa in Unstable angina: Receptor Suppression Using Integrilin therapy (PURSUIT) scores reported on a consecutive NSTE-ACS cohort.Citation8
A lower ejection fraction in non-survivors than in survivors in our cohort supports the likelihood of future complications due to a high risk of cardiac events, including not only recurrent myocardial ischemic events but also heart failure and arrhythmias among patients with NSTEMI.Citation6
Higher rates for CABG/PCI among patients with high GRACE scores in our cohort seem notable considering that patients with PCI who present with NSTEMI have very high GRACE scores and represent a very high-risk patient population regarding mortality.Citation5 The exclusion or underpresentation of NSTEMI patients with prior coronary intervention in clinical trials has prevented the determination of best management strategy in these patients.Citation5 It should be noted that only one fifth of our cohort was composed of NSTEMI patients with prior coronary intervention.Citation5
The main limitation of our study was its small sample size, which precludes us from reaching a more definitive conclusion regarding the predictive values of D-dimer assay, GRACE and TIMI scores for adverse outcome in patients with NSTEMI and making a significant contribution to the refining of risk scores. The restriction of outcome to mortality is another limitation, which also results from small sample size. Since there was no myocardial infarction or coronary revascularization recorded in our cohort during study period, we could not assess the overall major adverse cardiac events risk, but could assess only mortality risk associated with elevated D-dimer for NSTEMI patients. The use of major adverse cardiac events as the outcome for D-dimer may have provided more opportunity to assess the risk associated with elevated D-dimer for NSTEMI patients. Still, evidence from this study may contribute to meta-analysis and systematic reviews, and it may form a basis for further larger-scale studies on the validity of the GRACE risk scale and risk stratification score for predicting the risk of mortality among patients with NSTEMI.
Conclusion
In conclusion, our findings in a cohort of NSTEMI patients revealed a positive correlation among TIMI scores, GRACE scores and D-dimer levels. Although higher D-dimer levels were noted in non-survivors than in survivors, and although both D-dimer levels and TIMI scores were higher in patients with high GRACE scores, serum creatinine levels constituted the sole independent determinant of mortality risk, with no significant values of D-dimer levels or of GRACE or TIMI scores to predict the risk of mortality in NSTEMI patients. Larger-scale multicenter investigations with long-term follow-up are required to address the validity of the GRACE risk scale as well as to determine the ideal risk stratification score for predicting the risk of mortality upon admission among patients with NSTE-ACS.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- KushnerFGHandMSmithSCJr2009 focused updates: ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice GuidelinesJ Am Coll Cardiol2009542205224119942100
- BraunwaldEAntmanEMBeasleyJWAmerican College of CardiologyAmerican Heart AssociationCommittee on the Management of Patients With Unstable Angina. ACC/AHA 2002 guideline update for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction – summary article: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee on the Management of Patients with Unstable Angina)J Am Coll Cardiol2002401366137412383588
- MurrayCJLopezADMortality by cause for eight regions of the world: Global Burden of Disease StudyLancet1997349126912769142060
- RoffiMPatronoCColletJP2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC)Eur Heart J20163726731526320110
- AsrarUIHaqMRuddNMianMPredictors and outcomes of early coronary angiography in patients with prior coronary artery bypass surgery presenting with non-ST elevation myocardial infarctionOpen Heart20041e000059
- ShaikhMKHanifBShaikhKKhanWParkashJValidation of Grace Risk Score in predicting in-hospital mortality in patients with non ST-elevation myocardial infarction and unstable anginaJ Pak Med Assoc20146480781125255591
- van DomburgRTvan Miltenburg-van ZijlAJVeerhoekRJSimoonsMLUnstable angina: good long-term outcome after a complicated early courseJ Am Coll Cardiol199831153415399626831
- de Araújo GonçalvesPFerreiraJAguiarCSeabra-GomesRTIMI, PURSUIT, and GRACE risk scores: sustained prognostic value and interaction with revascularization in NSTE-ACSEur Heart J20052686587215764619
- AntmanEMCohenMBerninkPJThe TIMI risk score for unstable angina/non-ST elevation MI: a method for prognostication and therapeutic decision makingJAMA200028483584210938172
- GrangerCBGoldbergRJDabbousOHGlobal Registry of Acute Coronary Events InvestigatorsPredictors of hospital mortality in the global registry of acute coronary eventsArch Intern Med20031632345235314581255
- D’AscenzoFBiondi-ZoccaiGMorettiCTIMI, GRACE and alternative risk scores in acute coronary syndromes: a meta-analysis of 40 derivation studies on 216,552 patients and of 42 validation studies on 31,625 patientsContemp Clin Trials20123350751422265976
- JneidHAndersonJLWrightRSAmerican College of Cardiology FoundationAmerican Heart Association Task Force on Practice Guidelines2012 ACCF/AHA focused update of the guideline for the management of patients with unstable angina/non-ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice GuidelinesCirculation201212687591022800849
- FowkesFGLoweGDHousleyECross-linked fibrin degradation products, progression of peripheral arterial disease, and risk of coronary heart diseaseLancet199334284868100915
- NichenametlaGThomasVSEvaluation of serum pregnancy associated plasma protein-A & Plasma D-Dimer in acute coronary syndromeJ Clin Diagn Res201610BC01BC03
- LiuOLiJRGongMXuMDuJZhangHJGenetic analysis of six SNPs in candidate genes associated with high cross-race risk of development of thoracic aortic aneurysms and dissections in Chinese Han populationActa Pharmacol Sin2010311376138020871623
- WangXLLiuOQinYWZhangHJLvYAssociation of the polymorphisms of MMP-9 and TIMP-3 genes with thoracic aortic dissection in Chinese Han populationActa Pharmacol Sin20143535135524487965
- de Araújo GoncalvesPFerreiraJAguiarCSeabra-GomesRTIMI, PURSUIT, and GRACE risk scores: sustained prognostic value and interaction with revascularization in NSTE-ACSEur Heart J20052686587215764619
- EagleKALimMJDabbousOHGRACE InvestigatorsA validated prediction model for all forms of acute coronary syndrome: estimating the risk of 6-month postdischarge death in an international registryJAMA20042912727273315187054
- OmerGGokhanAAdemUSabriDKorhanSRelation of the aortic stiffness with the GRACE risk score in patients with the non ST-segment elevation myocardial infarctionInt J Clin Exp Med201473030303625356178
- TangEWWongCKHerbisonPGlobal Registry of Acute Coronary Events (GRACE) hospital discharge risk score accurately predicts long-term mortality post acute coronary syndromeAm Heart J2007153293517174633
- SantopintoJJFoxKAGoldbergRJCreatinine clearance and adverse hospital outcomes in patients with acute coronary syndromes: findings from the Global Registry of Acute Coronary Events (GRACE)Heart2003891003100812923009
- Al SuwaidiJReddanDNWilliamsKPrognostic implications of abnormalities in renal function in patients with acute coronary syndromesCirculation200210697498012186803
- AnavekarNSMcMurrayJJVelazquezEJRelation between renal dysfunction and cardiovascular outcomes after myocardial infarctionN Engl J Med20043511285129515385655
- BradshawPJKoDTNewmanAMDonovanLRTuJVValidity of the GRACE (Global Registry of Acute Coronary Events) acute coronary syndrome prediction model for six month post-discharge death in an independent data setHeart20069290590916387810
- FoxKADabbousOHGoldbergRJPrediction of risk of death and myocardial infarction in the six months after presentation with acute coronary syndrome: prospective multinational observational study (GRACE)BMJ2006333109117032691
- ElbarouniBGoodmanSGYanRTCanadian Global Registry of Acute Coronary Events (GRACE/GRACE(2)) InvestigatorsValidation of the Global Registry of Acute Coronary Event (GRACE) risk score for in-hospital mortality in patients with acute coronary syndrome in CanadaAm Heart J200915839239919699862
- NewmanJDDavidsonKWYeSShafferJAShimboDMuntnerPGender differences in calls to 9-1-1 during an acute coronary syndromeAm J Cardiol2013111586223040599
- Cabrerizo-GarcíaJLPérez-CalvoJIZalba-EtayoBInfluence of gender on prognosis of acute coronary syndromesRev Port Cardiol201534435025578946
- PoonSGoodmanSGYanRTBridging the gender gap: insights from a contemporary analysis of sex-related differences in the treatment and outcomes of patients with acute coronary syndromesAm Heart J2012163667322172438
- MossAJGoldsteinREMarderVJThrombogenic factors and recurrent coronary eventsCirculation1999992517252210330382
- OrakMUstündağMGüloğluCAlyanOSayhanMBThe role of serum D-dimer level in the diagnosis of patients admitted to the emergency department complaining of chest painJ Int Med Res2010381772177921309492
- MjelvaØRPönitzVBrügger-AndersenTGrundtHStainesHNilsenDWLong-term prognostic utility of pentraxin 3 and D-dimer as compared to high-sensitivity C-reactive protein and B-type natriuretic peptide in suspected acute coronary syndromeEur J Prev Cardiol2016231130114026635361