
Abstract
Background
Arterial stiffness (AS) can be determined by some noninvasive tests such as pulse wave velocity (PWV). Atherosclerosis is also detectable by some ultrasonographic techniques such as color M-mode-derived propagation velocity measured along the origin of the descending aorta (AVP).
Aim
The aim of the study was to find out a possible relationship between atherosclerosis and AVP and whether AVP can be used as a parameter of AS.
Materials and methods
The study group was composed of 134 people from routine screening examination who were ≥40 years old, completely healthy, and without any known disease and use of any drug. PWV has been determined to show aortic stiffness, and carotid artery intima– media thickness (CIMT) was measured for subclinical atherosclerosis. AVP values were obtained from all participants, and correlations were calculated between these parameters and age.
Results
AVP decreased (r=−0.902, P<0.001) and PWV increased (r=0.854, P<0.001) significantly with increasing age. CIMT also increased with aging (r=0.518, P<0.001). There were significant correlations between AVP and PWV (r=−0.832, P<0.001) and AVP and CIMT (r=−0.345, P<0.001).
Conclusion
Transthoracic echocardiographic determination of AVP can be used as a simple measurement of AS and correlates well with PWV, age, and CIMT in healthy people.
Introduction
Cardiovascular diseases (CVD) are the main cause of morbidity and mortality in many countries.Citation1 Life expectancy has been increased, and as such, increasing age has become a major problem in the recent decades because advancing age has been found to be one of the most important risk factors for CVD.Citation1 Aging may increase the risk of developing CVD causing arterial dysfunction.Citation2
Pulse wave velocity (PWV) is used as a gold-standard noninvasive measurement of arterial stiffness (AS). It has been proved to be independently related to mortality in normal populationCitation3–Citation5 and several diseases such as essential hypertension,Citation6 type 2 diabetes,Citation7 and end-stage renal disease (ESRD).Citation8–Citation10 Other measurements for AS, including aortic distensibility, aortic strain, and carotid femoralCitation11 or aortofemoral PWV,Citation12 are not routinely used in clinical practice since they are difficult to perform and time consuming.
The carotid artery intima–media thickness (CIMT) is strongly correlated with the presence and extent of CVDCitation13,Citation14 and associated with cardiovascular and cerebrovascular events.Citation15 Besides, aortic PWV and CIMT have found to be significantly correlated with each other in several studies.Citation16,Citation17
Color M-mode-derived propagation velocity measured along the origin of the descending aorta (AVP) has been also shown to be associated with presence and severity of atherosclerosis in patients with coronary artery disease,Citation12 type 2 diabetes mellitus,Citation18 and coronary slow flow.Citation19 It has been thought in these studies that a decrease in the flow propagation speed within the arterial lumen may reflect the increased aortic resistance due to atherosclerosis.
The aim of this study was to investigate the relationship between AVP and subclinical atherosclerosis and whether AVP can be used as a parameter of aortic stiffness.
Materials and methods
The study group was composed of 134 people from routine screening examination who were ≥40 years old, completely healthy, non-smoker, and without any known disease and use of any drug. Four participants were excluded due to imaging problems. All the 130 participants included in our study had normal sinus rhythm ECG, and echocardiographic images were of sufficient quality. The study was approved by the local ethics committee of Ordu University Medical School. All participants were informed about the study and provided their written consents. Complete blood count and some biochemical markers have been obtained from patients. Peripheral blood was drawn from a vein into sterile tubes, one of which was containing ethylenediamine tetra-acetic acid,Citation20,Citation21 and these samples underwent glucose, creatinine, and lipid profile measured by standard methods. Complete blood counts were measured by an automated hematology analyzer.
Transthoracic echocardiographic examination
Echocardiographic examination was performed by two experienced echocardiographers who were blinded to the clinical data. Three measures by each observer in each of 10 randomly selected patients were used to calculate inter-observer variability and 3 measures by the same observer from the same 10 randomly selected patients were used to calculate intra-observer variability.
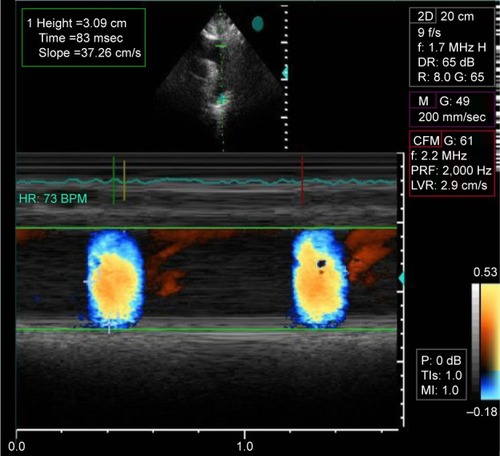
The patients were at rest and in the left lateral decubitus position. A commercially available echocardiographic device (Vivid 5S; General Electric, Chicago, IL, USA) with a 3.0 MHz rectangular (linear-array) transducer was used for echocardiographic examinations. Color M-mode Doppler measurements from suprasternal window at supine position were recorded with the cursor parallel to main flow of direction in descending aorta. Color Doppler Nyquist limit was set at 30–50 cm/s, and an M-mode spatio-temporal velocity map similar to the flame shape was obtained switching to M-mode with recorder sweep rate of 200 mm/s (). If the slope of flame was not clear, the aliasing velocity was changed using baseline shifting until isovelocity slope was clearly delineated. Dividing the distance between points corresponding to the beginning and end of the propagation slope by the duration between corresponding time points, aortic flow propagation velocity was calculated. As a result, velocity at which the flow is propagating down the artery was measured as AVP. Mean of at least three measurements was recorded as AVP value.
Figure 1 Measurement of color M-mode derived propagation velocity measured along the origin of the descending aorta (AVP).
Abbreviations: DR, deceleration rate; CFM, color flow mapping; PRF, pulse repetition velocity; LVR, left ventricular remodeling.
PWV
Carotid femoral PWV was measured according to current guidelinesCitation22 using the Complior device (Alam Medical, Vincennes, France). Pulsed-wave Doppler recordings were obtained from the descending thoracic artery at the origin of the subclavian artery and the left common femoral artery in supine position. Wavefront arrival at each location was defined by extrapolation of the ascending Doppler flow profile to the baseline using the electrocardiographic R wave as a time reference. Dividing the distance (measured on the body surface using a tape measure) by the time delay between two points, the descending aortofemoral PWV was calculated.Citation23 To cover a complete respiratory cycle, the mean of five successive readings was used in the analysis.
CIMT measurements
The subjects’ bilateral common carotid arteries were scanned longitudinally with a 7 MHz transducer attached to an available machine (Vivid 5S; General Electric). Indicating the border between the distal common carotid artery and the carotid bulb, the bulb dilation served as a landmark. Distal segment of the common carotid artery, 1–2 cm proximal to the carotid bulb, was used to obtain images. Intima and media lines were identified as two bright echogenic lines in the arterial wall. The intima–media thickness was measured as the distance between these lines. Images showing the maximum intima–media thickness were stored in a digitized fashion, and CIMT measurements were obtained offline. The mean of the measurements from both common carotid arteries was used for analysis. CIMT measurements did not include the plaques, defined as an endoluminal protrusion of the arterial lumen of ≥0.5 mm or localized ≥50% thickening of the intima compared to the rest of the wall.
Statistical analysis
Quantitative variables are expressed as mean ± standard deviation and qualitative variables as numbers and percentages. Pearson’s correlation analysis was used for correlation measurements where necessary. SPSS for Windows, version IBM 22.0, was used for the statistical tests. Statistically significance was considered if P<0.05 was found.
Results
The baseline characteristics of the patients are summarized in .
Table 1 Clinical and echocardiographic characteristics of study population
Both the inter-observer variability and intra-observer variability for all the echocardiographic measurements were measured <10%.
With increasing age, early diastolic flow (E), E/A ratio, and atrial contraction signal (A) decreased significantly (r=−0.293, P=0.001; r=−0.239, P=0.006; and r=187, P=0.033). Deceleration time (DT) and isovolumetric relaxation time (IVRT) significantly increased with increasing age (r=0.232, P=0.008 and r=0.339, P<0.001).
AVP decreased (r=−0.902, P<0.001) and PWV increased (r=0.854, P<0.001) significantly with increasing age. CIMT also increased with aging (r=0.518, P<0.001).
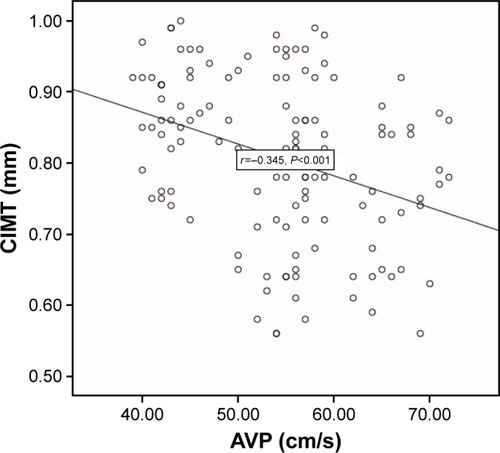
There were significant correlations between AVP and PWV (r=−0.832, P<0.001) (), AVP and age (r=−0.902, P<0.001) (), AVP and CIMT (r=−0.345, P<0.001) (), PWV and age (r=0.854, P<0.001), and PWV and CIMT (r=0.424, P<0.001).
Figure 2 Scatter plot of AVP for PWV measurements.
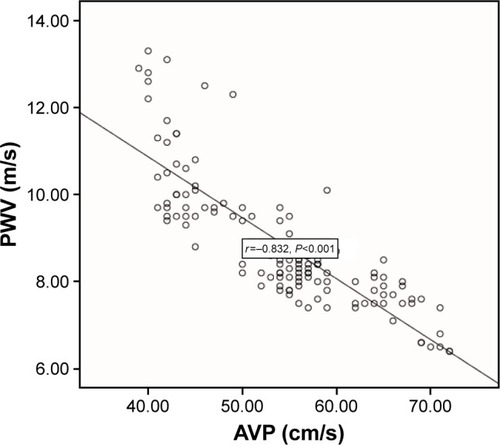
Figure 3 Scatter plot of AVP measurements for age.
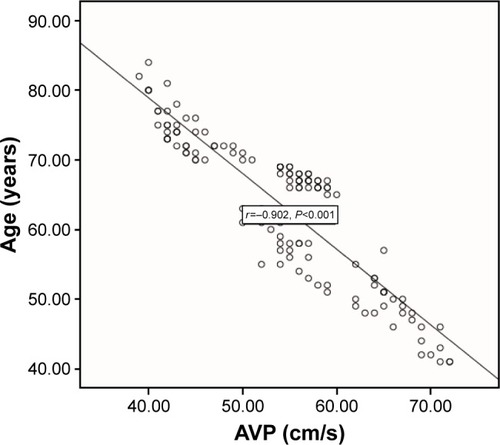
Figure 4 Scatter plot of AVP for CIMT measurements.
Discussion
In this study, we have found that AVP measured by transthoracic echocardiography is decreased in elderly people and significantly correlated with PWV and CIMT.
As a marker of vascular aging, AS is regarded to be a major risk factor for atherosclerotic events and CVDs. Besides, AS has been found to be associated with several cardiovascular risk factors including diabetes mellitus, obesity, smoking, hypercholesterolemia, hypertension, and advanced age.Citation6 Aortic distensibility and aortic strain decrease in parallel to the increase in the extent and the severity of the atherosclerosis. Tunica media thicken and get stiffer with the progression of atherosclerosis. Some noninvasive methods such as AVP in our study may demonstrate the atherosclerotic disease before it becomes clinically important. The arterial resistance increases as the arterial wall gets thick and stiff and the increase in arterial resistance decreases the flow and thus AVP.
In this study, we found that CIMT values increased with aging. This is an expected finding, since both AS and atherosclerosis increase with age. CIMT has been shown as an independent risk factor for coronary artery disease, and carotid atherosclerosis usually develops in concordance with coronary atherosclerosis and severity of coronary artery disease increases significantly with elevated CIMT.Citation24–Citation27 CIMT measurements have been demonstrated to facilitate the risk stratification of CAD in asymptomatic patients.Citation28 Besides, AVP, a newly discovered parameter, was signifi-cantly associated with CIMT in our study and decreasing with aging in concordance with increasing of CIMT.
Atherosclerosis can also be demonstrated by color M-mode propagation velocity measured along the origin of the descending thoracic aorta.Citation23 In patients with significant subclinical atherosclerosisCitation18 or coronary atherosclerosis,Citation29 AVP and CIMT have been demonstrated to be significantly associated with each other. In a recent study, Güneş et alCitation12 have found that AVP was the most significant predictor of coronary artery disease and significantly correlated with aortic stiffness measurements including aortic strain, aortic distensibility, and aortofemoral PWV. These findings show that the AVP could be used as an indicator of AS. In this study, we have demonstrated for the first time that AVP increases with age and AVP is significantly correlated with PWV and CIMT, which are indicators of aortic stiffness and atherosclerosis in healthy population.
This study revealed that AVP was correlated with PWV, CIMT, and age, all of which are predictors of subclinical atherosclerosis. Thus, we can say that AVP may be regarded as one of the important measures of atherosclerosis. Besides, PWV is the golden standard method for detection of aortic stiffness. Aortic stiffness can be also measured by several methods including aortic compliance, distensibility, augmentation index, and pulse pressure. Including PWV, these methods are usually difficult to perform and time consuming in daily practice.Citation30–Citation34 However, measurement of AVP that is significantly correlated with PWV is easy compared to these methods for detection of aortic stiffness, and it does not carry additional costs for daily practice.
AVP is the flow propagation in aorta and may be influenced by the kinetic energy dispersion of pulsatile blood. A measurement of pulse propagation along the great vessel wall, pulse pressure has not been found to be correlated with age and AVP in our study. As a result, we did not think that flow propagation affected our results. This may be due to the exclusion of patients with hypertension that may affect flow propagation.
Limitations
Limited echocardiographic image quality may be an obstacle to the measurement of AVP and the reproducibility of the acquisition, and reading of the methods may constitute a limitation. Measurements may also be affected by aortic anatomy and loading conditions. Our study population has a small size that might have biased the statistical results. Large population studies are needed to confirm the applicability of AVP measurements as a screening method.
Conclusion
Measurement of AVP is noninvasive, practical, quantitative, safe, simple, and reproducible, which promotes its application in clinical and scientific research. In this study, we have demonstrated for the first time that AVP decreases with age and AVP is significantly correlated with PWV and CIMT that are indicators of aortic stiffness and atherosclerosis in healthy population. Therefore, AVP measurements can be easily applicable in clinical practice as an indicator of atherosclerosis and aortic stiffness in healthy population.
Disclosure
The authors report no conflicts of interest in this work.
References
- Lloyd-JonesDAdamsRJBrownTMHeart disease and stroke statistics–2010 update: a report from the American Heart AssociationCirculation2010121e46e21520019324
- LakattaEGLevyDArterial and cardiac aging: major shareholders in cardiovascular disease enterprises: part I: aging arteries: a ‘set up’ for vascular diseaseCirculation200310713914612515756
- ShokawaTImazuMYamamotoHPulse wave velocity predicts cardiovascular mortality: findings from the Hawaii-Los Angeles-Hiroshima StudyCirc J20056925926415731528
- Willum-HansenTStaessenJATorp-PedersenCPrognostic value of aortic pulse wave velocity as an index of arterial stiffness in the general populationCirculation2006113566467016461839
- MitchellGFHwangSJVasanRSArterial stiffness and cardiovascular events: the Framingham Heart StudyCirculation2010121450551120083680
- LaurentSBoutouyriePAsmarRAortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patientsHypertension20013751236124111358934
- CruickshankKRisteLAndersonSGWrightJSDunnGGoslingRGAortic pulse wave velocity and its relationship to mortality in diabetes and glucose intolerance: an integrated index of cardiovascular function?Circulation2002106162085209012379578
- BlacherJGuerinAPPannierBMarchaisSJSafarMELondonGMImpact of aortic stiffness on survival in end-stage renal diseaseCirculation199999182434243910318666
- GuerinAPBlacherJPannierBMarchaisSJSafarMELondonGMImpact of aortic stiffness attenuation on survival of patients with end-stage renal failureCirculation2001103798799211181474
- ShojiTEmotoMShinoharaKDiabetes mellitus, aortic stiffness and cardiovascular mortality in end-stage renal diseaseJ Am Soc Nephrol200112102117212411562410
- LaurentSCockcroftJVan BortelLEuropean Network for non-invasive investigation of large arteries. Expert consensus document on arterial stiffness: methodological issues and clinical applicationsEur Heart J200627212588260517000623
- GüneşYTuncerMYildirimMGüntekinUGümrükçüoğluHASahinMA novel echocardiographic method for the prediction of coronary artery diseaseMed Sci Monit2008149MT42MT4618758427
- WoffordJLKahlFRHowardGRMcKinneyWMTooleJFCrouseJR3rdRelation of extent of extracranial carotid artery atherosclerosis as measured by B-mode ultrasound to the extent of coronary atherosclerosisArterioscler Thromb1991116178617941931880
- CravenTERyuJEEspelandMAEvaluation of the associations between carotid artery atherosclerosis and coronary artery stenosis. A case-control studyCirculation1990824123012422205416
- BotsMLHoesAWKoudstaalPJHofmanAGrobbeeDECommon carotid intima-media thickness and risk of stroke and myocardial infarction: the Rotterdam StudyCirculation1997965143214379315528
- van PopeleNMGrobbeeDEBotsMLAssociation between arterial stiffness and atherosclerosis: the Rotterdam StudyStroke200132245446011157182
- MackeyRHSutton-TyrrellKVaitkeviciusPVCorrelates of aortic stiffness in elderly individuals: a subgroup of the Cardiovascular Health StudyAm J Hypertens2002151 pt 1162311824854
- SimsekHSahinMGunesYDoganAGumrukcuogluHATuncerMA novel echocardiographic method for the detection of subclinical atherosclerosis in newly diagnosed, untreated type 2 diabetesEchocardiography201330664464823347332
- SimsekHSahinMGunesYA novel echocardiographic method as an indicator of endothelial dysfunction in patients with coronary slow flowEur Rev Med Pharmacol Sci201317568969323543453
- LiuOLiJRGongMXuMDuJZhangHJGenetic analysis of six SNPs in candidate genes associated with high cross-race risk of development of thoracic aortic aneurysms and dissections in Chinese Han populationActa Pharmacol Sin201031101376138020871623
- WangXLLiuOQinYWZhangHJLvYAssociation of the polymorphisms of MMP-9 and TIMP-3 genes with thoracic aortic dissection in Chinese Han populationActa Pharmacol Sin201435335135524487965
- van BortelLMLaurentSBoutouyriePArtery SocietyEuropean Society of Hypertension Working Group on Vascular Structure and FunctionEuropean Network for Noninvasive Investigation of Large ArteriesExpert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocityJ Hypertens201230344544822278144
- GunesYTuncerMGuntekinUThe relation between the color M-mode propagation velocity of the descending aorta and coronary and carotid atherosclerosis and flow-mediated dilatationEchocardiography201027330030520486958
- Kablak-ZiembickaAPrzewlockiTPieniazekPThe role of carotid intima-media thickness assessment in cardiovascular risk evaluation in patients with polyvascular atherosclerosisAtherosclerosis2010209112513019762025
- Kabłak-ZiembickaAPrzewłockiTStępieńERelationship between carotid intima-media thickness, cytokines, atherosclerosis extent and a two-year cardiovascular risk in patients with arteriosclerosisKardiol Pol201169101024103122006602
- JohnstonSCZhangHMessinaLMLawtonMTDeanDChlamydia pneumoniae burden in carotid arteries is associated with upregulation of plaque interleukin-6 and elevated C-reactive protein in serumArterioscler Thromb Vasc Biol200525122648265316210572
- ChamblessLEFolsonARCheqqLXCarotid wall thickness is predictive of incident clinical stroke: the Atherosclerosis Risk in Communities (ARIC) studyAm J Epidemiol2000151547848710707916
- ZanchettiAHennigMHollweckRBaseline values but not treatment-induced changes in carotid intima-media thickness predict incident cardiovascular events in treated hypertensive patients: findings in the European Lacidipine Study on Atherosclerosis (ELSA)Circulation2009120121084109019738145
- SezginATSigirciABarutcuIVascular endothelial function in patients with slow coronary flowCoron Artery Dis200314215516112655279
- NicholsWWClinical measurement of arterial stiffness obtained from noninvasive pressure waveformsAm J Hypertens2005181 pt 23S10S Review15683725
- WeberTAuerJO’RourkeMFArterial stiffness, wave reflections, and the risk of coronary artery diseaseCirculation2004109218418914662706
- WoodmanRJWattsGFMeasurement and application of arterial stiffness in clinical research: focus on new methodologies and diabetes mellitusMed Sci Monit200395RA81RA89 Review12761466
- LacombeFDartADewarEJenningsGCameronJLauferEArterial elastic properties in man: a comparison of echo-Doppler indices of aortic stiffnessEur Heart J1992138104010451505552
- OliverJJWebbDJNoninvasive assessment of arterial stiffness and risk of atherosclerotic eventsArterioscler Thromb Vasc Biol200323455456612615661