
Abstract
Introduction
The purpose of this study was to compare the value of hematological parameters, neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and mean platelet volume (MPV), as indicators of anterior uveal segment involvement in patients with Behcet’s disease (BD).
Patients and methods
Hospital-based records of a total of 912 patients with BD from the dermatology clinic and healthy volunteers from the checkup clinic were assessed retrospectively. After applying the exclusion criteria of the study, 71 of the BD patients with anterior uveitis, 69 of the BD patients without ophthalmological pathology and 151 healthy volunteers were included in the study. MPV, PLR, and NLR values of patients and healthy volunteers were compared.
Results
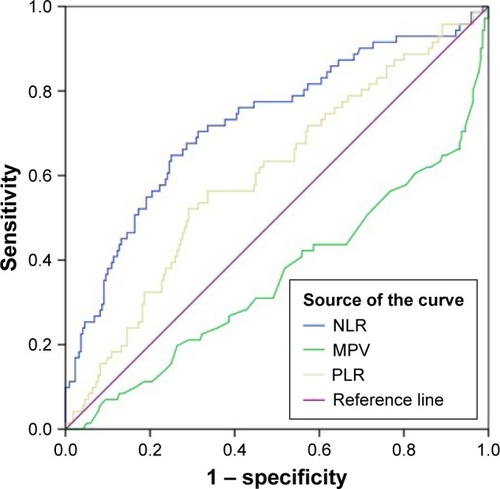
All MPV, PLR, and NLR values of patients who had anterior uveitis were significantly higher than those of other patients and healthy volunteers. Statistically, considering area under curves (ratio): NLR was 0.725 (0.653–0.797), P<0.001; PLR was 0.600 (0.523–0.676), P=0.012, and MPV was 0.358 (0.279–0.437), P<0.001.
Conclusion
MPV, PLR, and NLR are all valuable for assessment of anterior uveal segment involvement in patients with BD. However, the NLR seems to be better than the PLR and MPV for indicating anterior uveitis due to BD.
Keywords:
Introduction
Behcet’s disease (BD) is a multi-systemic disease characterized by oral and genital aphthous ulcers and skin lesions, and it can also involve many organs and systems, such as the eyes and central nervous system.Citation1 BD was first described by Hulusi Behcet in 1937, but the etiopathogenesis of the disease has not yet been fully elucidated.Citation2 Until 2014, many researchers adopted the criteria of the International Study Group, established in 1990, for the diagnosis of BD.Citation3
Bilateral, recurrent, non-granulomatous uveitis is a well-known ocular manifestation of BD. Retinal vasculitis and involvement of the posterior segment (eg, retinal hemorrhage, optic atrophy, hypopyon, and choroiditis) may also be seen in BD.Citation4
There is no specific laboratory test for diagnosing BD. Many studies have been conducted on tests which may reflect disease activation, be helpful in monitoring treatment efficiency, or predict potential complications of BD.Citation5 In the literature, a limited number of studies have attempted to identify an inflammatory marker which can predict uveitis. Türkçü et al reported that initially, mean platelet volume (MPV) was significantly lower in patients with active uveitis than in controls, but the significance disappeared over time.Citation6,Citation7
In general, BD progresses with inflammation, which has been emphasized in the pathogenesis of uveitis. This raises the question of whether inflammation markers can be helpful in identifying patients with uveitis. The platelet-to-lymphocyte ratio (PLR) has been suggested as a predictor of several conditions, especially cancer and the inflammatory conditions discussed in the following sections.Citation8–Citation13 The neutrophil-to-lymphocyte ratio (NLR) has been evaluated in some studies on BD.Citation14 This issue was also researched by our group while studying anterior uveitis related to BD (BD + AU).Citation15
In this study, we investigated the MPV, NLR, and PLR in order to determine which one is best for indicating anterior uveitis in patients with BD.
Patients and methods
Data were retrospectively gathered from 912 patients presenting to the Kayseri Research and Training Hospital and diagnosed with BD using international diagnostic criteria. Of 912 patients, 217 with anterior uveitis but without ocular signs were considered eligible, as they fulfilled the International Working Group’s criteria for ophthalmological examination.
Exclusion criteria for patients were: if ophthalmologic examination of patients was not performed, eye disease other than anterior uveitis was present, patients with cardiovascular involvement, renal failure, cardiac failure, vascular thrombosis, a history of anticoagulant use, or concurrent infections, due to the potential effects of these conditions on the MPV, PLR, or NLR. These patients were also excluded if active BD findings (arthritis, gastrointestinal system involvement, etc.) were noted, which would cause inflammatory responses in the patient and could alter hematologic parameters. We attempted to exclude patients who were noted to be in the inflammatory process, either independently of the BD or depending on the BD activity. Another exclusion criterion was the timing of blood testing; patients whose blood samples were not collected at the same time as the ophthalmological examination were not included in the study.
Thus, 71 patients with a diagnosis of anterior uveitis (BD + AU) and 69 BD subjects with normal ocular findings (BD) at the time of the blood tests were included in the BD + AU and BD groups, respectively. A third group, the healthy controls, consisted of 151 patients. We carefully screened healthy volunteer patients for chronic liver disease, chronic kidney disease, infectious disease, or chronic illness which could cause inflammation. The group consisting of patients with BD without any ophthalmologic findings was noted as BD. The group consisting of BD patients who had anterior uveitis was classified as BD + AU. Patients were excluded from the study if their tests were not performed simultaneously with anterior uveitis diagnosis. The PLR was determined by dividing the platelet count by the lymphocyte count. The NLR was determined by dividing the neutrophil count by the lymphocyte count.
This study was approved by the Kayseri Training and Research Hospital Ethics Committee. The ethics committee obtained the necessary approvals for the use of medical records of patients and volunteers. Patient consent to review their medical records was not required by the Kayseri Training and Research Hospital Ethics Committee, as all data were de-identified and anonymized.
Statistical analysis
The continuous data were analyzed to find the mean, standard deviation, median, and percentages. Student’s t-test was used to compare continuous variables among the studied groups. The Mann–Whitney U test was used to compare the medians of numerical variables with a skewed distribution. One-way ANOVA and Kruskal–Wallis tests were used to compare the parameters in all three groups according to their distribution. A Bonferroni correction was performed. A chi-square test was used to compare categorical variables. Pearson correlation analysis was used to determine the relationships between the patient and control groups. ROC curves were used to evaluate the performance of variables in indicating the presence of anterior uveitis in BD patients. A P-value of <0.05 was considered to be significant. All statistical analyses were performed using Statistical Package Program for Social Sciences, version 23.0 (IBM Corporation, Armonk, NY, USA).
Results
The mean age was 40.41±14.20 years in the healthy group, 39.44±10.28 years in the BD group, and 37.44±10.82 years in the BD + AU group (P=0.244). Females comprised 23.2% of the BD group, and 76.8% of the patients in the BD + AU group were male (P<0.001). The distribution of the healthy subjects according to sex was 75.6% male/24.4% female. Features of the control and patient groups are summarized in .
Table 1 Comparison between Behcet’s disease groups with and without anterior uveitis
PLR feature
Values of the PLR were significantly different among groups (P=0.040); the mean PLR value was 124.45±33.12 in the healthy controls, 125.15±41.44 in the BD group, and 137.37±38.16 in the BD + AU group. With a Bonferroni correction applied, the difference between the healthy controls and the BD group was not statistically significant (P=1.000), the difference between the healthy controls and the BD + AU group was statistically significant (P=0.043), and the difference between the BD and BD + AU groups was not statistically significant (P=0.145). The AUC (ratio) value of the PLR was 0.600 (0.523–0.676), with P=0.012.
MPV feature
The mean MPV was 9.81±1.11 fl in the healthy control group, 9.35±1.36 fl in the BD group, and 8.97±1.41 fl in the BD + AU groups; the groups were statistically significantly different (P<0.001). With a Bonferroni correction applied, the difference between the healthy controls and the BD group was statistically significant (P=0.032), the difference between the healthy controls and the BD + AU group was statistically significant (P<0.001), and the difference between the BD and BD + AU groups was not statistically significant (P=0.235). The AUC value of the MPV was 0.358 (0.279–0.437), with P<0.001.
NLR feature
When the NLR values of the groups were compared, the median value was 2.37 (0.96–6.36) in the BD + AU group and 1.54 (1.38–1.81) in the BD group. The median NLR of the healthy controls was 1.88 (1.52–2.26). The groups were significantly different (P<0.001). In pair-wise comparisons, the difference between the healthy controls and the BD group was statistically significant (P<0.001), the healthy controls and the BD + AU group were significantly different (P<0.001), and the BD and BD + AU groups were significantly different (P<0.001). The AUC value of the NLR was 0.725 (0.653–0.797), with P<0.001. The NLR of 2.04 had 67.6% sensitivity and 69.1% specificity for anterior uveitis.
ROC analyses were performed to compare the ability of the MPV, PLR, and NLR to indicate anterior uveitis and are summarized in .
Figure 1 Receiver operating characteristic curves for neutrophil to NLR, MPV and PLR.
Abbreviations: MPV, mean platelet volume; PLR, platelet-to-lymphocyte ratio; NLR, neutrophil-to-lymphocyte ratio.
Discussion
In this study, we investigated changes in some hematological parameters which point to inflammation in the context of anterior uveitis, a complication of BD. Male patients represented the majority of the BD + AU group, consistent with previous reports.Citation16 The age of the patients in each of the three groups was similar.
In the pathogenesis of BD, neutrophils are believed to play an important role. It is thought that neutrophil hyper-activation, which can be confirmed by the up-regulation of CD10, CD11a, and CD14 on cell surfaces, plays an important role in the pathogenesis of BD by increasing chemotaxis, phagocytosis, superoxide generation, and myeloperoxidase levels.Citation17–Citation21 In BD, pro-inflammatory cytokines secreted by T cells or APCs, such as TNF-α, IL-8, IFN-γ, or G-CSF, seem to be responsible for the priming of neutrophils, but the underlying mechanism is not yet clear.Citation22,Citation23 Current data suggest that platelets interact with endothelial cells and leukocytes, leading to release of inflammatory substances which cause monocyte adhesion and transmigration.Citation24,Citation25
The NLR, PLR, and MPV have been investigated to find out which of them is most valuable in the diagnosis of BD + AU. We did not find any other studies which had investigated these values for anterior uveitis before we completed our study and submitted it for publication. However, there have been recent closed-design studies examining BD and ocular complications. For the sake of clarity, we will discuss them under separate headings for each parameter.
MPV
The MPV is a direct indicator of platelet function and exhibits an inverse correlation with platelet count.Citation26 As stated in the introduction, changes in the MPV in many different conditions have been researched. While the MPV was not found to be associated with disease and/or disease activity in some of these conditions, it is increased or decreased in others. An increased MPV has been associated with increased thrombotic disposition.Citation27 Also, a reduced MPV has been found in patients with rheumatoid arthritis, ankylosing spondylitis, and systemic lupus erythematosus arthritis when compared to controls.Citation28,Citation29 A higher MPV in patients with active BD has also been reported.Citation30 The role of the MPV in differentiation between BD and recurrent oral aphthous ulcers was also investigated, but no evidence for the effectiveness of the MPV in such differentiation could be obtained.Citation23 In a recent study, Türkçü et al examined the MPV in 36 BD patients with ocular findings and found no significant change.Citation6 However, in a very recent study from Turkey, MPV and severity of BD were found to be correlated with each other.Citation31 In that study, complications were evaluated as a whole (eg, arthritis and complications of the eyes, large vessels, and central nervous system).
It is important to note that the current study focuses only on anterior uveitis, and the sample size is larger than previous studies. In both the BD and BD + AU groups, the MPV values were found to be low even though they were not statistically different from the healthy group. However, the difference between the median MPV in the BD and BD + AU groups was not statistically significant. As was concluded in a previous study, we found no relationship between the MPV and anterior uveitis.Citation6
PLR
In recent years, the PLR has emerged as a marker which can be readily used for several diseases. Studies indicate a significant increase in the PLR in cardiovascular and oncologic diseases. In a recent study, it was shown that the PLR is a prognostic factor in non-ST-elevation myocardial infarction.Citation32 A number of studies, including the study conducted by Smith et al, have shown that the PLR is a prognostic factor in periampullary pancreatic carcinoma.Citation8 Asher et al reported that the PLR is a novel marker which may predict ovarian cancer.Citation9 In a recent study, the PLR was found to be significantly higher in dipper than in non-dipper hypertension.Citation10 A study by Gary et al concluded that an increased PLR is associated with critical ischemia of the extremities in patients with peripheral arterial occlusive disease.Citation11 Recently, a study from Turkey reported that the PLR is associated with the coronary slow flow phenomenon.Citation12 We found that the PLR value was significantly higher in the BD + AU group than in the healthy group. There was no significant difference between the BD and BD + AU groups or between the BD and healthy control groups.
NLR
The NLR is accepted as an indicator of worsening or recurrence of chronic diseases. In the literature, an increased NLR is mostly used as a negative prognostic factor in cardiovascular diseases and cancers.Citation33–Citation35 It has also been investigated in respiratory system diseases, pulmonary tuberculosis, and serious infections and found to be higher in all of them.Citation36–Citation38 Similarly, systemic inflammation has been reported as a significant factor in metabolic syndromes, including obesity and diabetes mellitus.Citation39,Citation40 Cananzi et al reviewed recent evidence that immunological phenomena may explain the unexpected positive response rate in patients with advanced disease. A simple estimation of the NLR has been advocated as a prognostic marker for several cancers; eg, it is useful in metastatic melanoma.Citation41 In the recent study by our group, we showed that the NLR changes significantly in patients with anterior uveitis.Citation15 Similarly in a recent study, Balkarli et al concluded that NLR may be a simple, inexpensive, and convenient diagnostic marker of active BD.Citation42 And recently, Yüksel et al concluded that NLR levels were higher in patients with active ocular BD compared to the inactive ocular BD group.Citation43
As a limitation, since it was a retrospective study, it was not possible to report clearly the treatments applied to the subjects.
In this study, the ability of the NLR to indicate anterior uveitis in BD patients was much stronger than other markers. In one of our previous publications we saw that the NLR changed significantly in the BD and BD + AU groups. The median NLR values of patients in the BD group were higher than the median values in healthy volunteers, which is consistent with the literature.Citation14 Similarly, the median NLR values in the BD + AU group were higher than in the normal healthy volunteers. Our previous work on NLR did not have this result.
We used ROC curves to compare the ability of the MPV, PLR, and NLR to indicate anterior uveitis. When the AUC is evaluated, it is seen that the NLR is better as an indicator. On the other hand, the ability of the PLR to demonstrate anterior uveitis was found to be better than that of the MPV, but neither was statistically significant.
Conclusion
No specific tests can directly diagnose BD or its complications. Several studies have focused on the parameters which could solve this problem. The PLR and MPV have been compared, as well as the NLR, which is known to predict anterior uveitis; the NLR was found to be a better marker for detection of anterior uveitis in patients with BD than the MPV or PLR. For clinicians, one of the consequences of these results is that when they witness changes in these parameters, they should consider that one of the causes of the developing inflammation could be an anterior uveitis attack.
Disclosure
The authors report no conflicts of interest in this work.
References
- BolsterMBMKSAP 15 Medical Knowledge Self-assessment Program: RheumatologyPhiladelphia, PAAmerican College of Physicians2009
- BehçetHMattesonELOn relapsing, aphthous ulcers of the mouth, eye and genitalia caused by a virus. 1937Clin Exp Rheumatol2010284 Suppl 60S2S5
- No authors listedCriteria for diagnosis of Behçet’s disease. International Study Group for Behçet’s DiseaseLancet19903358697107810801970380
- JabsDANussenblattRBRosenbaumJTStandardization of Uveitis Nomenclature (SUN) Working GroupStandardization of uveitis nomenclature for reporting clinical data. Results of the First International WorkshopAm J Ophthalmol2005140350951616196117
- AvciAAvciDSerum prolactin levels in Behçet’s disease. Is there a relationship between Behçet’s disease and prolactin as in other autoimmune diseases?Acta Dermatovenerol Croat2013211525323683488
- TürkcüFMYükselHSahinAMean platelet volume in pseudoexfoliation syndrome and glaucomaEur J Ophthalmol2014241717523813107
- RicartJMEspanaFNavarroSTodolíJMiguel De la FuenteJVayáAMean platelet volume does not seem to relate to thrombosis or posterior uveitis in Behçet’s diseaseClin Hemorheol Microcirc2013541515722750994
- SmithRABosonnetLGhanehPThe platelet lymphocyte ratio improves the predictive value of serum CA19-9 levels in determining patient selection for staging laparoscopy in suspected periampullary cancerSurgery2008143565866618436014
- AsherVLeeJInnamaaABaliAPreoperative platelet lymphocyte ratio as an independent prognostic marker in ovarian cancerClin Transl Oncol201113749950321775277
- SunbulMGerinFDurmusENeutrophil to lymphocyte and platelet to lymphocyte ratio in patients with dipper versus non-dipper hypertensionClin Exp Hypertens201436421722123786430
- GaryTPichlerMBelajKPlatelet-to-lymphocyte ratio: a novel marker for critical limb ischemia in peripheral arterial occlusive disease patientsPLoS One201387e6768823844064
- OylumluMDoğanAOylumluMRelationship between platelet to lymphocyte ratio and coronary slow flowAnatol J Cardiol201515539139525430406
- GürlerAİdilABoyvatAÇalışkanDThe evaluation of age at onset of the first symptom according to sex in the 2175 Behçet’s Patients followed up between 1976 and 1997 at Ankara University Multidisciplinary Behçet’s Disease CenterTurkiye Klinikleri Journal of Dermatology2000108386 Turkish
- RifaiogluENBülbül SenBEkizÖCigdem DogramaciANeutrophil to lymphocyte ratio in Behçet’s disease as a marker of disease activityActa Dermatovenerol Alp Pannonica Adriat2014234656725527038
- AvciAAvciDCinarSLEffect of anterior uveitis in neutrophil to lymphocyte ratioInternational Eye Science2016164
- Abu-AmeerhMAMohammedSFMohammadMTAbabnehOHAl-BdourMDOcular manifestations of Behçet’s disease in Jordanian patientsSaudi J Ophthalmol201327424725124371419
- KobayashiMItoMNakagawaANeutrophil and endothelial cell activation in the vasa vasorum in vasculo-Behcet’s diseaseHistopathology200036436237110759951
- Eksioglu-DemiralpEDireskeneliHKibarogluAYavuzSErgunTAkogluTNeutrophil activation in Behcet’s diseaseClin Exp Rheumatol2001195 Suppl 24S19S2411760393
- ZierhutMMizukiNOhnoSImmunology and functional genomics of Behçet’s diseaseCell Mol Life Sci20036091903192214523551
- BecattiMEmmiGSilvestriENeutrophil activation promotes fibrinogen oxidation and thrombus formation in Behçet diseaseCirculation2016133330231126585672
- PaySŞimşekIErdemHDinçAImmunopathogenesis of Behcet’s disease with special emphasize on the possible role of antigen presenting cellsRheumatol Int200727541742417171346
- KawakamiTOhashiSKawaYElevated serum granulocyte colony-stimulating factor levels in patients with active phase of sweet syndrome and patients with active Behçet disease: implication in neutrophil apoptosis dysfunctionArch Dermatol2004140557057415148101
- EkizOBaltaISenBBRifaiogluENErginCBaltaSDemirkolSMean platelet volume in recurrent aphthous stomatitis and Behçet diseaseAngiology201465216116523766348
- LindemanSKramerBSeizerPGawazMPlatelets, inflammation and atherosclerosisJ Thromb Haemost20075Suppl 120321117635728
- GürsoyOMKarakoyunSKalçikMUsefulness of novel hematologic inflammatory parameters to predict prosthetic mitral valve thrombosisAm J Cardiol2014113586086424411287
- ThreatteGAUsefulness of the mean platelet volumeClin Lab Med19931349379508313690
- AcikgozNKarincaogluYErmisNIncreased mean platelet volume in Behçet’s disease with thrombotic tendencyTohoku J Exp Med2010221211912320484842
- KisacikBTufanAKalyoncuUMean platelet volume (MPV) as an inflammatory marker in ankylosing spondylitis and rheumatoid arthritisJoint Bone Spine200875329129418403245
- YukselOHelvaciKBasarOAn overlooked indicator of disease activity in ulcerative colitis: mean platelet volumePlatelets200920427728119459134
- UzkeserHHalilogluSCayirYIs mean platelet volume a new activity criterion in Behçet’s disease?Blood Coagul Fibrinolysis201526783683926196194
- AlanSTunaSTürkoğluEBThe relation of neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and mean platelet volume with the presence and severity of Behçet’s syndromeKaohsiung J Med Sci2015311262663126709224
- AzabBShahNAkermanMMcGinnJTJrValue of platelet/lymphocyte ratio as a predictor of all-cause mortality after non-ST-elevation myocardial infarctionJ Thromb Thrombolysis201234332633422466812
- KoideNSaitoHSuzukiAClinicopathologic features and histochemical analyses of proliferative activity and angiogenesis in small cell carcinoma of the esophagusJ Gastroenterol2007421293293818085349
- BrennerBTangLHShiaJKlimstraDSKelsenDPSmall cell carcinomas of the gastrointestinal tract: clinicopathological features and treatment approachSemin Oncol2007341435017270665
- TamhaneUUAnejaSMontgomeryDRogersEKEagleKAGurmHSAssociation between admission neutrophil to lymphocyte ratio and outcomes in patients with acute coronary syndromeAm J Cardiol2008102665365718773982
- ZahorecRRatio of neutrophil to lymphocyte counts – rapid and simple parameter of systemic inflammation and stress in critically illBratisl Lek Listy2001102151411723675
- KnausWADraperEAWagnerDPZimmermanJEAPACHE II: a severity of disease classification systemCrit Care Med198513108188293928249
- VincentJLMorenoRTakalaJThe SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care MedicineIntensive Care Med19962277077108844239
- NakanishiNSatoMShiraiKSuzukiKTataraKWhite blood cell count as a risk factor for hypertension; a study of Japanese male office workersJ Hypertens200220585185712011644
- MarslandALMcCafferyJMMuldoonMFManuckSBSystemic inflammation and the metabolic syndrome among middle-aged community volunteersMetabolism201059121801180820619428
- CananziFCDalgleishAMudanSSurgical management of intraab-dominal metastases from melanoma: role of the neutrophil to lymphocyte ratio as a potential prognostic factorWorld J Surg20143861542155024366277
- BalkarliAKucukABaburHErbasanFNeutrophil/lymphocyte ratio and mean platelet volume in Behçet’s diseaseEur Rev Med Pharmacol Sci201620143045305027460734
- YukselMYildizAOylumluMNovel markers of endothelial dysfunction and inflammation in Behçet’s disease patients with ocular involvement: epicardial fat thickness, carotid intima media thickness, serum ADMA level, and neutrophil-to-lymphocyte ratioClin Rheumatol201635370170825744156