
Abstract
Type 2 diabetes (T2D) imposes a substantial disease burden, predominantly from cardiovascular disease (CVD), which accounts for >50% of deaths in this population and leads to a 12-year reduction in the life expectancy of a 60-year-old male patient with T2D and CVD compared with the general population. The results from mandatory cardiovascular outcome trials (CVOTs) are therefore of great interest in the field. The Academy for Cardiovascular Risk, Outcomes and Safety Studies in Type 2 Diabetes meeting program aims to bring together experts from several associated disciplines to provide fair and balanced resources for those involved in the management of patients with T2D. This publication represents the opinions of the faculty on the key learnings from the meeting held in Vienna in the spring of 2017. In particular, we detail how data from the EMPA-REG OUTCOME® [cardiovascular outcomes trial of empagliflozin] and Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER®) (liraglutide) CVOTs can be practically interpreted across clinical specialities. It is hoped that this translation of CVOT data will achieve a dual treatment paradigm for the management of both raised glucose levels and CV risk in patients with T2D.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
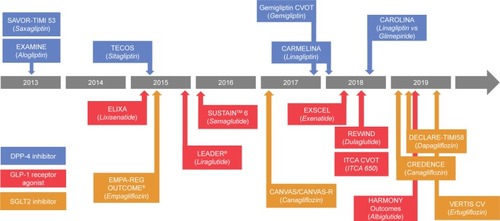
For every 11 adults worldwide, one person is living with diabetes, equating to 415 million people (projected to increase to 642 million by 2040).Citation1 Around 90% of these individuals have type 2 diabetes (T2D).Citation1 T2D represents a substantial disease burden to each patient, often involving multiple comorbidities.Citation2 Cardiovascular disease (CVD) is chief among these, accounting for >50% of deaths in patients with T2D. The life expectancy of a 60-year-old male patient with T2D and CVD is reduced by 12 years compared with the general population.Citation1–Citation3 There are multiple therapeutic agents now available or in the pipeline for the treatment of T2D (), and establishing their cardiovascular (CV) safety has become a key factor in the approval process, with cardiovascular outcomes trials (CVOTs) now being mandatory for all new agents.
Figure 1 Completed and ongoing cardiovascular outcome trials in type 2 diabetes.
Abbreviations: CV, cardiovascular; CVOT, cardiovascular outcome trial; DPP-4, dipeptidyl peptidase 4; GLP-1, glucagon-like peptide 1; SGLT2, sodium/glucose cotransporter 2; CANVAS, Canagliflozin Cardiovascular Assessment Study; CANVAS-R, Study of the Effects of Canagliflozin on Renal Endpoints in Adult Subjects with T2DM; CARMELINA®, Cardiovascular Safety and Renal Microvascular Outcome Study with Linagliptin; CAROLINA®, Cardiovascular Outcome Study of Linagliptin Versus Glimepiride in Patients with Type 2 Diabetes; CREDENCE, Evaluation of the Effects of Canagliflozin on Renal and Cardiovascular Outcomes in Participants with Diabetic Nephropathy; DECLARE-TIMI, Multicenter Trial to Evaluate the Effect of Dapagliflozin on the Incidence of Cardiovascular Events; ELIXA, Evaluation of Lixisenatide in Acute Coronary Syndrome; EXAMINE, Examination of Cardiovascular Outcomes with Alogliptin versus Standard of Care; EXSCEL, The EXenatide Study of Cardiovascular Event Lowering; OMNEON™ [randomized, double-blind, placebo-controlled, multicenter study to assess cardiovascular outcomes following treatment]; REWIND, Researching Cardiovascular Events with a Weekly Incretin in Diabetes; SAVOR-TIMI, Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus–Thrombolysis in Myocardial Infarction; TECOS, Trial Evaluating Cardiovascular Outcomes with Sitagliptin; LEADER®, Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results; EMPA-REG OUTCOME® [cardiovascular outcomes trial of empagliflozin]; SUSTAIN, Trial to Evaluate Cardiovascular and Other Long-term Outcomes With Semaglutide in Subjects with Type 2 Diabetes; T2DM, type 2 diabetes mellitus; 3P-MACE, 3-point major adverse CV events (CV death, nonfatal myocardial infarction or nonfatal stroke); 4P-MACE, 4-point major adverse CV events (CV death, nonfatal myocardial infarction, nonfatal stroke or unstable angina requiring hospitalization).
No increased CV risk was observed in the three CVOTs that had been reported at the time of this meeting and statistical superiority was demonstrated in two of them:Citation4–Citation7 EMPA-REG OUTCOME® [cardiovascular outcomes trial of empagliflozin], which investigated the sodium/glucose cotransporter 2 (SGLT2) inhibitor empagliflozin, and Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER®), which investigated the glucagon-like peptide 1 (GLP-1) receptor agonist liraglutide. Significant protection for certain CV outcomes was reported in these two CVOTs (Box 1 and ), enabling physicians to both control glucose levels and lower CV risk with a single agent. In addition, the SUSTAIN™-6 non-inferiority study of semaglutide reported some positive results, although further study will need to be performed to demonstrate superiority. In addition, semaglutide is not currently licenced; therefore, the results were not discussed in any depth at this particular meeting. Since the meeting, the results of the Canagliflozin Cardiovascular Assessment Study of the SGLT2 inhibitor canagliflozin have been published, which also showed a statistically significant benefit for 3-point major adverse CV events.Citation8 A further publication is in preparation following a subsequent meeting to discuss these results. Overall, the CVOT results have the potential to enable a profound shift in clinical practices across the T2D-related specialities, such as endocrinology, cardiology, and nephrology.
Table 1 Positive CVOT studies in T2D -percentage reduction in key outcomes
The Academy for Cardiovascular Risk, Outcomes and Safety Studies in Type 2 Diabetes program was initiated with the aim of providing education and resources for health care professionals managing patients with T2D within the Central and East European region. A range of tools and information has been developed in collaboration with an expert steering committee, including primary and specialist care experts from cardiology, endocrinology, diabetology, and nephrology, to provide fair and balanced resources that are aligned to the needs and challenges facing health care practitioners (HCPs) involved in the management of patients with T2D (available at Academy for Cardiovascular Risks, Outcomes and Safety Studies in Type 2 Diabetes (T2D), 2017; https://www.across-t2d.com). The steering committee also provides guidance on the interpretation and communication of clinical data and, where applicable, provides guidance on regional/national adaptation of the international recommendations. A series of biannual Scientific Exchange Meetings across Latin America, Europe, and Asia has also allowed direct peer-to-peer communication and education, with the most recent being held in Vienna in the spring of 2017 (March 22–24). The specified educational aims of the Vienna meeting were:
review areas of outstanding unmet medical needs in the management of patients with T2D;
consider the impact of the published CVOTs on clinical practice and treatment recommendations;
discuss and address safety topics of the SGLT2 inhibitor class and interpret the CVOT data for clinical practice through case discussions.
EMPA-REG OUTCOME® (empagliflozin):
Death from CV causes:
3.7% vs 5.9% in the placebo group; HR, 0.62; 95% CI 0.49–0.77; p<0.001
Hospitalization for HF:
2.7% vs 4.1%; HR, 0.62; 95% CI 0.49–0.77; p<0.001
Death from any cause:
5.7% vs 8.3%; HR, 0.68; 95% CI 0.57–0.82; p<0.001
LEADER® (liraglutide):
Death from CV causes:
4.7% vs 6.0% in the placebo group; HR, 0.78%; 95% CI 0.66–0.93; p=0.007
Death from any cause:
8.2% vs 9.6%; HR, 0.85; 95% CI 0.74–0.97; p=0.02
Abbreviations: CI, confidence interval; CV, cardiovascular; CVOT, cardiovascular outcomes trial; HF, heart failure; HR, hazard ratio; EMPA-REG OUTCOME®, [cardiovascular outcomes trial of empagliflozin]; LEADER®, Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results.
This publication represents the opinions of the faculty on the key learnings from the meeting, detailing how the discussions of CVOT data have led to insights into the practical application of these data across clinical specialities for the treatment of both raised glucose levels and CV risk in patients with T2D within the region.
T2D is a chronic and complex condition requiring a duality of treatment: CV benefits together with glucose-lowering benefits in microvascular outcomes. It is more imperative that the benefits of collaboration and awareness between specialities are recognized, leading to more effective treatment for the patient across multiple T2D morbidities.
CV morbidity and mortality remain the biggest burden of the disease, although advances in glucose-lowering therapies have decreased microvascular complications over the past decade.Citation9–Citation15 Furthermore, we have come to understand that renal protection should also be an integral part of the newly emerging treatment paradigm, being intricately linked to the effects of T2D. Renal and cardiac factors are closely linked, and acute or chronic disorders in one frequently induce dysfunction in the other. Elderly patients with chronic kidney disease are also more likely to die of heart disease than to advance to end-stage renal disease and dialysis.Citation16,Citation17
The renal sub-analyses of the EMPA-REG OUTCOME study indicated that, in addition to the overall study data showing no adverse renal effects from empagliflozin, there were also significant renoprotective outcomes for patients with both new onset and established renal disease.Citation6,Citation18
In this landscape of T2D comorbidities, the potential for combining glucose lowering with protection against CVD, as well as new and worsening nephropathy and proteinuria, is welcome for both physicians and patients. Indeed, the ability to treat on more than one disease front was seen by delegates as a novel addition to the treatment paradigm, and communication of this paradigm, both directly to colleagues and through guidelines, was a key message from the meeting discussions.
The positive CVOT results set the scene for an update to the treatment paradigm
The empagliflozin CVOT EMPA-REG OUTCOME was a pioneer study within the CVOT landscape, being among the first published, and the first to demonstrate cardioprotection. As such, the positive CV outcomes reported in this trial have set the scene for the new treatment approach of combining glucose lowering with protection against CVD.Citation19 Direct comparison cannot be made between EMPA-REG OUTCOME and the liraglutide CVOT LEADER, given that they were not head-to-head studies and had some variation between their study populations and certain outcome measures. Nevertheless, as both these CVOTs reported positive CV outcomes, it is useful to consider the main results of each ( and Box 1).
In patients with T2D and established CVD, the addition of empagliflozin to standard of care reduced CV mortality and hospitalization for heart failure (HF), and improved overall survival compared with placebo. The overall safety profile of empagliflozin was consistent with that observed in previous clinical trials and the current label information.Citation6,Citation19,Citation20
In patients with T2D and established CVD or at high CV risk, the addition of liraglutide to standard of care reduced CV mortality and improved overall survival. The most common adverse events leading to discontinuation of liraglutide were gastrointestinal events.Citation5
From the physicians’ perspective, empagliflozin and liraglutide currently represent two agents with the most robust available data for use in the treatment pathway as an add-on therapy to metformin for patients with T2D and established CVD. This has particularly been recognized for empagliflozin, with both US and European Union (EU) regulators approving changes to the product label that emphasize the importance of the CV benefits of the drug. The indication information in the US label now contains the statement “Jardiance is a SGLT2 inhibitor indicated: As an adjunct to diet and exercise to improve glycaemic control in adults with T2D. To reduce the risk of CV death in adult patients with T2D and established CVD”.Citation21,Citation22 The EU label update reinforces the concept that both improvement of glycemic control and reduction of CV morbidity and mortality are an integral part of the treatment of T2D. Across Europe and globally, international and local guidelines have been updated to include recommendations based on CVOT data, most notably data from EMPA-REG OUTCOME.Citation23–Citation28 This is also true for the European Society of Cardiology (ESC) guidelines, further enhancing the perception among physicians that these agents are now firmly positioned in the treatment pathway.Citation29–Citation31
Empagliflozin safety profile
A discussion point of particular significance at the meeting was the question of safety of some SGLT2 inhibitors. Concerns that have been raised in the past include risks of ketoacidosis, osteoporosis, urinary tract infections, hypoglycemic episodes, urinary and genital tract infections, kidney disease, and amputations.Citation6,Citation18,Citation32,Citation33 However, data from EMPA-REG OUTCOME have shown that empagliflozin was not associated with a serious adverse event signal compared with placebo.Citation4,Citation19,Citation34 For example, the study found no increased risk of adverse renal outcomes or bone fracture, despite the concerns that have been raised with other SGLT2 inhibitors.Citation4,Citation19,Citation34 Reassuringly, genital infections, which are easily self-treated by over-the-counter medications, were the only adverse events to show a significant increase over placebo.Citation19
Initial concerns raised by nephrologists regarding the kidney targeting mode of action (MoA) of empagliflozin, as an SGLT2 inhibitor, have therefore largely been assuaged, and nephrologists now have a positive opinion of empagliflozin based on the renal sub-analyses of EMPA-REG OUTCOME, which showed that patients who received empagliflozin in addition to standard of care had a significantly lower risk of progression of kidney disease, either as new or worsening nephropathy.Citation6,Citation18
The safety data in EMPA-REG OUTCOME also demonstrate that, conceptually, it may not be necessary to understand the intricacies of the MoA of empagliflozin – as yet not fully understood – given that there is now reassurance from safety data, combined with proven efficacy.Citation3,Citation20 After all, metformin was, and is, still prescribed almost universally without such an understanding.
Is there a class effect?
Guidelines such as those authored by the American Diabetes Association or ESC recognize the importance of recommending only those molecules that have demonstrated CV protection in a CVOT, and not extending this recommendation automatically to other molecules in the same class.Citation29,Citation30,Citation35 At the time of writing this manuscript, empagliflozin and liraglutide were the only approved antidiabetic agents to have demonstrated CV protection in CVOTs. Differentiating data on safety and side effects demonstrate that an overall class effect of SGLT2 inhibitors has not yet been shown. Although molecules of dapagliflozin and canagliflozin are similar to those of empagliflozin, small differences in the molecular structure can potentially lead to critical differences in function. For example, the molecular differences beween the hormones testosterone and estradiol are substantially smaller than the differences between empagliflozin molecule and the other two members of the class (National Center for Biotechnology Information PubChem Compound Database: compound identity [CID] =6013; CID =5757; CID =11949646; CID =9887712; CID =24812758). Furthermore, CVOT results have been mixed between different GLP-1 receptor agonists and dipeptidyl peptidase 4 (DPP-4) inhibitors, which supports the notion that data from one drug cannot necessarily be extrapolated to drugs in the same class.Citation5,Citation36–Citation39 Although the SGLT2 inhibitors may seem to be similar to one another in terms of efficacy and safety,Citation40–Citation44 a CVOT is needed to define the CV effects of the other members.
The value of SGLT2 inhibitors in patients with lower CV risk
It is noteworthy that uptake of the SGLT2 inhibitor class to date has been lower than might have been expected considering the excellent efficacy and reassuring safety data for empaglifozin. One of the explanations put forward for why the use of SGLT2 inhibitors as second-line therapy after metformin is much less compared with DPP-4 inhibitors is the assumption that glucose-lowering drugs cannot change CV morbidity/mortality when used in patients with early T2D who present with a low CV/renal risk. DPP-4 inhibitors have been in use for almost 10 years and are very well-tolerated, so any shift toward the use of SGLT2 inhibitors (in particular, to empagliflozin) is more often seen in patients with established CVD. Recently, three observational studies (THIN, NORDIC, and CVD-REAL) reported analyses of the effect of SGLT2 inhibitors in patients with T2D and low CV risk.Citation41–Citation43 A similar trend to EMPA-REG OUTCOME was shown in THIN and CVD-REAL, suggesting that all-cause mortality and hospitalization for HF may be statistically lower when SGLT2 inhibitors were initiated compared with other glucose-lowering drugs, even in patients with low CV risk. However, as the event rates in these studies were very low (<1.0%) and the 95% confidence intervals were wide, these data can only be considered as relatively low level. In the NORDIC study, the use of new glucose-lowering drugs (the SGLT2 inhibitor dapagliflozin and DPP-4 inhibitors) was compared with the administration of insulin, which, in Sweden, is used comparatively early in the disease. Mortality was significantly lower when dapagliflozin or DPP-4 inhibitors were used compared with insulin, and a direct comparison of the SGLT2 inhibitor versus the DPP-4 inhibitors showed superiority of the former for all endpoints analyzed.Citation44 The observational design and the lack of randomization cannot totally exclude a prescription bias, that is, preferred use of SGLT2 inhibitors in patients with a lower risk, as this was not documented in the comparison. Despite these limitations and the differences in the background treatment and predominant use of different SGLT2 inhibitors in the US compared with Europe, a similar risk reduction was seen across all six countries involved in CVD-REAL. These well-performed observational studies, which trend in the same direction, add to the emerging view that SGLT2 inhibitors are the drug of choice in the majority of patients with T2D and either established CVD or CV risk factors. However, only prospective, well-performed CVOTs such as EMPA-REG OUTCOME can offer robust evidence of significant CV benefits.
HF and subclinical HF are among the earliest CV complications seen during the follow-up of patients with T2D who had not exhibited evidence of CVD at baseline,Citation45 which may explain the positive CV outcomes with the early use of SGLT2 inhibitors that was observed in the real-world studies. Furthermore, as HF is associated with the highest mortality rates in patients with T2D,Citation20 the potential benefits of SGLT2 inhibitors in reducing the risk of HF could explain the reduction in mortality. It is important, therefore, to emphasize to prescribers the potential benefit to patients at all stages of T2D. To this end, continued education and support for both primary and specialist HCPs are desirable. Although endocrinologists and cardiologists both currently prescribe empagliflozin, they often operate quite separately, whereas increased collaboration may lead to improved outcomes by treating the whole disease and by increasing awareness of when cross-referring would be beneficial for the patient.Citation46
Maximizing efficacy
Although numerous international and regional guidelines have been updated to include the prescribing of antidiabetic agents based on CVOT data, a majority recommend a free choice of agents after metformin. There is, however, a perceived need for more specific direction toward those agents that may be most suitable for particular patients. A simple-to-use intuitive format, rather than an exhaustive narrative, would be of the greatest use – what may be referred to perhaps as “smart guidelines”. Indeed, the Canadian, Swiss, and Russian guidelines include a concise algorithm/table format, and discussion at the meeting showed that these were well-received by faculty and delegates alike. A clear pathway, with guidance on the place of each agent within it, would be a valuable support tool for endocrinologists, cardiologists, and primary care physicians (PCPs) alike.
Perceived barriers to prescribing SGLT2 inhibitors include concerns about publicized adverse events, reimbursement issues, discrepancies in guidelines, lack of regular local updates (eg, reluctance to update the guidelines further until there is more evidence on class effects for SGLT2 inhibitors), and, significantly, inertia. In the workshop sessions in particular, where smaller group sizes allowed more in-depth discussion, an unwillingness among attending physicians’ peers to change their habitual practice of prescribing well-used or cheaper drugs, such as metformin or sulfonylureas (SUs), was discussed. In addition, hospital payers resist reimbursing the newer agents until SUs have been tried. To overcome these barriers, it was felt that a program of education was needed, ideally led by local physician advocates. By sharing safety and efficacy data from the CVOT studies that show the dual benefits of antidiabetic agents that can both lower glucose levels and reduce CV risk in patients with T2D, it is hoped that physicians’ inertia to changing prescription habits will be overcome, leading to increased pressure on payers to release reimbursement.
Although the prime impetus for change may come from education, collaboration can also be a great influencer. T2D does not exist in isolation from other morbidities, and it is clear that the complexity of the disease means that it is often encountered by specialists from outside the diabetes therapy area, such as those in the fields of cardiology and nephrology. During the course of any one person’s journey with T2D, a series of specialists can be encountered, including PCPs, diabetologists, internalists, cardiologists, nephrologists, ophthalmologists, diabetes nurses/educators, and even orthopedists and surgeons. It is important that all physicians who deal frequently with patients with T2D are in possession of the most suitable therapies for each individual patient. As the complexity of T2D can often lead to patients suffering from multiple morbidities, it is not desirable for each specialism to focus on only one aspect (such as diabetologists on HbA1c, cardiologists on blood pressure, or nephrologists on estimated glomerular filtration rate). Instead, cross-collaboration may help to treat the whole disease more effectively, in addition to increasing awareness of when it is appropriate to refer a patient from one specialism to the other. By working together, and by considering the new dual paradigm explored at this meeting, the concerns of both diabetologists and cardiologists can be addressed using a single antidiabetic agent.
We should note that the discussions that took place at this meeting were of an informal, qualititative nature. The limitations of such a structure mean that quantitative analyses were not appropriate; so this report represents the opinions of the faculty, rather than a formal recommendation.
Conclusion
It is apparent that T2D is a complex disease, requiring a multifactorial approach to achieve the best outcomes. With more than half of all patients with T2D still dying from CVD, it is clear that the whole disease needs to be treated: both CV risk and glucose levels. Risk factors such as unhealthy lifestyles (notably poor-quality diet, physical inactivity, and smoking) and hypertension need to be addressed, and a simpler therapy regimen instigated that can provide treatment suitable for all patients, for example, patients with hepatic or renal insufficiency or HF. So far, empagliflozin is the only drug that has emerged with proven efficacy and safety across all these aspects. In addition, empagliflozin is the first antidiabetic agent to be supported by health authorities and official guidelines for the dual use of glucose lowering and reducing CV risk. In the future, HCPs working with patients with T2D will need to consider how best to work together to maximize the benefits seen from this important addition to the pharmaceutical armamentarium.
Acknowledgments
Editorial support was provided by Julia Coleman of Fortis Pharma Communications, with financial support by Boehringer Ingelheim. The opinions expressed are entirely the authors’ own and the only involvement of Boehringer Ingelheim was to look through the manuscript for accuracy.
Disclosure
GS has received research grants and honoraria for speaking from Abbot, Amgen, Andromeda, AstraZeneca, Bayer, Boehringer Ingelheim, BMS, DeveloGen, Eli Lilly, GSK, Janssen, Merck, MSD, Novartis, Novo Nordisk, Pfizer, Roche, Sanofi-Aventis, Serono, Servier, and Takeda, and has served as principal investigator in >40 studies.
KK has received honoraria for speaking and consultancy from AstraZeneca, BMS, Boehringer Ingelheim, Janssen, Lilly, MSD, Novartis, Novo Nordisk, and Sanofi. He has received research support from AstraZeneca, Boehringer Ingelheim, Lilly, MSD, Novartis, Novo Nordisk, Roche, and Sanofi.
CL has received honoraria for speaking and consultancy from Boehringer Ingelheim, MSD, Boston Scientific, Medtronic, AstraZeneca, Bendit, Healthwatch, Cordio, and CardiaX.
MB has received research grants from Boehringer Ingelheim AG, Bayer, Pfizer, Actelion, Medtronic, Chemocentryx, Amgen, and honoraria for speaking from Menarini, Sankyo, Servier, Boehringer Ingelheim, and Amgen.
HD has received research grants and honoraria for speaking and consultancy from Merck, MSD, Pfizer, Sanofi-Aventis, AstraZeneca, Bayer, Takeda, Daiichi-Sankyo, Novartis, Boehringer Ingelheim, Amgen, BMS, Abbott, Janssen-Cilag, and Genericon.
MP has received honoraria for speaking and consultancy from Abbott, AstraZeneca, Boehringer Ingelheim, Dexcom, Eli Lilly, Medtronic, Novo Nordisk, Roche, Sanofi, Servier, and Takeda.
The authors report no other conflicts of interest in this work.
References
- International Diabetes FederationIDF Diabetes Atlas7th ed20151140 Available from: http://www.diabetesatlas.org/Accessed October 10, 2017
- SeshasaiSRKKaptogeSThompsonAEmerging Risk Factors CollaborationDiabetes mellitus, fasting glucose, and risk of cause-specific deathN Engl J Med2011364982984121366474
- SchernthanerGJarvisSLotanCPráznýMWannerCWascherTCAdvances in the management of cardiovascular risk for patients with type 2 diabetes: perspectives from the Academy for Cardiovascular Risk, Outcomes and Safety Studies in Type 2 DiabetesTher Clin Risk Manag201713697928144148
- ZinmanBInzucchiSELachinJMRationale, design, and baseline characteristics of a randomized, placebo-controlled cardiovascular outcome trial of empagliflozin (EMPA-REG OUTCOME™)Cardiovasc Diabetol201413110224943000
- MarsoSPDanielsGHBrown-FrandsenKLiraglutide and cardiovascular outcomes in type 2 diabetesN Engl J Med2016375431132227295427
- WannerCInzucchiSELachinJMEmpagliflozin and progression of kidney disease in type 2 diabetesN Engl J Med2016375432333427299675
- MarsoSPBainSCConsoliASemaglutide and cardiovascular outcomes in patients with type 2 diabetesN Engl J Med2016375191834184427633186
- NealBPerkovicVMahaffeyKWCanagliflozin and cardiovascular and renal events in type 2 diabetesN Engl J Med2017377764465728605608
- PatelAMacMahonSChalmersJADVANCE Collaborative GroupIntensive blood glucose control and vascular outcomes in patients with type 2 diabetesN Engl J Med2008358242560257218539916
- BergenstalRMBaileyCJKendallDMType 2 diabetes: assessing the relative risks and benefits of glucose-lowering medicationsAm J Med20101234374
- UKPDS Study GroupIntensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33)Lancet199835291318378539742976
- HaywardRAReavenPDWiitalaWLFollow-up of glycemic control and cardiovascular outcomes in type 2 diabetesN Engl J Med2015372232197220626039600
- Ismail-BeigiFGenuthSClinical implications of the ACCORD trialJ Clin Endocrinol Metab2012971414822049171
- Ismail-BeigiFCravenTBanerjiMAEffect of intensive treatment of hyperglycaemia on microvascular outcomes in type 2 diabetes: an analysis of the ACCORD randomised trialLancet2010376973941943020594588
- ZoungasSChalmersJNealBFollow-up of blood-pressure lowering and glucose control in type 2 diabetesN Engl J Med2014371151392140625234206
- DalrympleLSKatzRKestenbaumBChronic kidney disease and the risk of end-stage renal disease versus deathJ Gen Intern Med201126437938520853156
- RoncoCHaapioMHouseAAAnavekarNBellomoRCardiorenal syndromeJ Am Coll Cardiol200852191527153919007588
- WakisakaMLetter to the editor on: Wanner C, Inzucchi SE, Zinman B. Empagliflozin and progression of kidney disease in type 2 diabetesN Engl J Med2016375181799180227806237
- ZinmanBWannerCLachinJMEmpagliflozin, cardiovascular outcomes, and mortality in type 2 diabetesN Engl J Med2015373222117212826378978
- FitchettDZinmanBWannerCHeart failure outcomes with empagliflozin in patients with type 2 diabetes at high cardiovascular risk: results of the EMPA-REG OUTCOME® trialEur Heart J201637191526153426819227
- Jardiance 10 mg and 25 mg film-coated tablets [prescribing information]. (eMC) Print friendly, 2017GermanyBoehringer Ingelheim Limited
- Jardiance [prescribing information]Ingelheim am RheinGermanyBoehringer Ingelheim International GmbH2016134
- LehmannRBiandaTBrändleMMesures Visant Contrôle De La Glycémie Chez Les Patients Atteints De Diabète Sucré De Type 2. [Recommendations of SGED/SSED: Measures for blood glucose control in patients with type 2 diabetes mellitus]2016117BadenSociété Suisse d’Endocrinologie et de Diabétologie French. Available from: http://sgedssed.ch/fr/informations-pour-professionnels/lignes-directrices/Accessed October 10, 2017
- LehmannRBiandaTBrändleMEmpfehlungen der SGED/SSED: Massnahmen zur Blutzuckerkontrolle bei Patienten mit Diabetes mellitus Typ 2. [Recommendations of SGED/SSED: Measures for blood glucose control in patients with type 2 diabetes mellitus]2016116BadenSchweizerische Gesellschaft für Endokrinologie und Diabetologie German. Available from: http://sgedssed.ch/informationen-fuer-fachpersonen/richtlinien-guidelines/Accessed October 10, 2017
- ŠkrhaJPelikánováTKvapilMČeská diabetologická společnostCzech Diabetes Society Recommended treatment for type 2 diabetes mellitusPrague2016115 Czech
- Austrian Diabetes Society (ODG) and the Austrian Lipid ConsensusCo-ordinated by Clodi M. and Toplak H. Diabetes mellitus – Instructions for practice. Revised and extended version 2016. Wiener klinische wochenschriftThe Central European Journal of Medicine2016128S37S228 German
- Canadian Diabetes Association Clinical Practice Guidelines Expert CommitteePharmacologic management of type 2 diabetes: 2016 interim updateCan J Diabetes201640648448627912867
- DedovIIShestakovaMVMayorovAYStandards of specialized diabetes careDiabetes Mellitus2017201S1121
- PiepoliMFHoesAWAgewallS2016 European guidelines on cardiovascular disease prevention in clinical practiceEur Heart J201637292315238127222591
- PonikowskiPVoorsAAAnkerSD2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failureEur Heart J201637272129220027206819
- RoffiMPatronoCColletJ-P2015 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC)Eur Heart J201637326731526320110
- FDAFDA drug safety communication: FDA revises label of diabetes drug canagliflozin (Invokana, Invokamet) to include updates on bone fracture risk and new information on decreased bone mineral density2015 Available from: http://www.fda.gov/Drugs/DrugSafety/ucm461449.htmAccessed April 27, 2017
- PRAC, Committee PRAPRAC recommendation, EMA/76661/20172017 Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Referrals_document/SGLT2_inhibitors_Canagliflozin_20/Recommendation_provided_by_Pharmacovigilance_Risk_Assessment_Committee/WC500221431.pdfAccessed April 27, 2017
- KohlerSPatelSDeFronzoRASafety and tolerability of combinations of empagliflozin/linagliptin for 52 weeks in subjects with type 2 diabetes2015 Available from: http://www.easdvirtualmeeting.org/resources/safety-and-tolerability-of-combinations-of-empagliflozin-linagliptin-for-52-weeks-in-subjects-with-type-2-diabetes--3Accessed October 10, 2017
- Standards of medical care in diabetes-2017: summary of revisionsDiabetes Care201740Suppl 1S4S527979887
- GreenJBBethelMAArmstrongPWEffect of sitagliptin on cardiovascular outcomes in type 2 diabetesN Engl J Med2015373323224226052984
- PfefferMAClaggettBDiazRLixisenatide in patients with type 2 diabetes and acute coronary syndromeN Engl J Med2015373232247225726630143
- SciricaBMBhattDLBraunwaldESaxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitusN Engl J Med2013369141317132623992601
- WhiteWBCannonCPHellerSRAlogliptin after acute coronary syndrome in patients with type 2 diabetesN Engl J Med2013369141327133523992602
- SonessonCJohanssonPAJohnssonEGause-NilssonICardiovascular effects of dapagliflozin in patients with type 2 diabetes and different risk categories: a meta-analysisCardiovasc Diabetol2016153726895767
- KosiborodMCavenderMAFuAZLower risk of heart failure and death in patients initiated on SGLT-2 inhibitors versus other glucose-lowering drugs: the CVD-REAL studyCirculation Epub2017518
- NyströmTBodegårdJNathansonDThuressonMNorhammarAErikssonJWNovel oral glucose-lowering drugs are associated with lower risk of all-cause mortality, cardiovascular events and severe hypoglycaemia compared with insulin in patients with type 2 diabetesDiabetes Obes Metab20173561364
- ToulisKAWillisBHMarshallTAll-cause mortality in patients with diabetes under treatment with dapagliflozin: a population-based, open-cohort study in the health improvement network databaseJ Clin Endocrinol Metab201710251719172528323967
- BirkelandKIJorgensenMECarstensenBCardiovascular mortality and morbidity in patients with type 2 diabetes following initiation of sodium-glucose co-transporter-2 inhibitors versus other glucose-lowering drugs (CVD-REAL Nordic): a multinational observational analysisLancet Diabetes Endocrinol20175970971728781064
- ShahADLangenbergCRapsomanikiEType 2 diabetes and incidence of cardiovascular diseases: a cohort study in 1.9 million peopleLancet Diabetes Endocrinol20153210511325466521
- ScheenAJDiabetes: time for reconciliation between cardiologists and diabetologistsNat Rev Cardiol201613950951027411401