
Abstract
Objective
The aim of this study was to evaluate the efficacy and safety of the mesenchymal stem cell (MSC) therapy in patients with ischemic stroke (IS).
Materials and methods
Clinical trials involved in this research were searched from PubMed, Web of Science, Cochrane Library, Embase, Wanfang and CNKI database. Therapeutic effects of MSC therapy were assessed according to National Institutes of Health Stroke Scale (NIHSS), Barthel index (BI), Fugl-Meyer Assessment (FMA) and Functional Independence Measure (FIM), and its safety was evaluated based on adverse events.
Results
This research covered 23 trials including 1,279 IS patients. Based on our analysis, the overall condition of IS patients significantly improved after MSC therapy, indicated by decreased NIHSS and increased BI, FMA and FIM scores. Our analysis also showed that the treatment effects in the MSC transplantation group were superior to those in the control group (routine medication therapy) with statistical significance for NIHSS (1 month after therapy: odds ratio [OR]=−1.92, CI=−3.49 to −0.34, P=0.02; 3 months after therapy: OR=−2.65, CI=−3.40 to −1.90, P<0.00001), BI (1 month after therapy: OR=0.99, CI=0.19–1.79, P=0.02; 6 months after therapy: OR=10.10, CI=3.07–17.14, P=0.005), FMA (3 months after therapy: OR=10.20, CI=3.70–16.70, P=0.002; 6 months after therapy: OR=10.82, CI=6.45–15.18, P<0.00001) and FIM (1 month after therapy: OR=15.61, CI=−0.02 to 31.24, P=0.05; 6 months after therapy: OR=16.56, CI=9.06–24.06, P<0.0001). No serious adverse events were reported during MSC therapy.
Conclusion
MSC therapy is safe and effective in treating IS by improving the neurological deficits, motor function and daily life quality of patients.
Introduction
Stroke is the most lethal and second most incident disease, together with cancer and cardiovascular disease.Citation1,Citation2 Ischemic stroke (IS) and intracerebral hemorrhage account for about 85% and 15%, respectively, of all stroke events.Citation3 The main pathological manifestation of IS is temporary brain tissue ischemia.Citation1 Ischemia results in reduced neuron number and interrupted neural axon network, and formation of a defected environment around the ischemic region, which prohibits brain self-healing, eventually resulting in the permanent loss of nerve tissue or disabled brain function.Citation1,Citation4,Citation5 Over 50,000,000 people are suffering from IS of various degrees in the world.Citation6 The annual mortality rate is close to 10%, and nearly 50% of stroke survivors are left with disabling sequelae.Citation1,Citation2,Citation4 Poststroke rehabilitation therapy is scant, and currently the most efficient medicine for IS in clinical settings is tissue plasminogen activator.Citation1,Citation7 However, it functions mainly at the early stage of ischemia with a short time window, which may increase the risk of cerebral hemorrhage, and therefore, its clinical application is severely limited.Citation7
Stem cell therapy, using hematopoietic stem cells (HSCs),Citation8,Citation9 neural stem cells (NSCs),Citation10,Citation11 endothelial progenitor cells (EPCs)Citation12 and other types of stem cells,Citation13,Citation14 was considered a promising treatment for IS as it may reduce injury and promote rehabilitation after stroke. Mesenchymal stem cells (MSCs) are derived from mesoderm and have the capacity of regeneration and differentiation. MSCs can differentiate into various lineages such as NSCs, which can further differentiate into neurons, astrocytes, oligodendrocytes and so on,Citation4,Citation15,Citation16 with low immunogenicity and high histocompatibility.Citation1,Citation15 Compared with other types of stem cells, such as NSCs, EPCs and HSCs, MSCs are more accessible as they can be easily obtained from umbilical cord, bone marrow, fat and other tissues, and can proliferate rapidly in vitro with little ethical constraints.Citation15 Preliminary preclinical studies using MSCs to treat IS have shown beneficial effects.Citation17–Citation19 In animal models, researchers found the transplanted cells migrated to lesions, secreted neurotrophic factors, remitted inflammatory response and promoted plasticity and revascularization thereby minimizing the damage.Citation18–Citation20
Although both preclinical studies and studies with experimental models regarding MSC transplantation therapies for IS have been carried out,Citation17–Citation19 the clinical application of MSCs still has a long way to go due to its unverified safety and therapeutic effects. To address this issue, we conducted a meta-analysis of published clinical trials treating IS with MSCs, to provide scientific references for upcoming research and future clinical application.
Materials and methods
Search strategy and selection criteria
Studies were identified from PubMed, Web of Science, Cochrane Library, Embase, Wanfang and CNKI database, with key terms (“mesenchymal stem cells” or “MSC”) and (“ischemic stroke” or “cerebral infarction” or “cerebral ischemia” or “brain ischemia”), without language restriction. The last search was performed in October 2017.
Studies were included if they fulfilled the following inclusion criteria: case-controlled trials involving IS patients; participants were diagnosed with IS and without malignant tumor, pregnancy and lactation; and patients in the experimental group received both MSC transplantation and IS routine treatment (RT; including conventional medical therapy and rehabilitation training treatment) combined therapy, and those in control group were treated by RT alone.
Data extraction and quality assessment
All data collection and extraction were performed by two authors (PX and MW) independently. The following information was summarized: author’s names, years of publication, locations, type of IS, samples sizes, patients’ ages, study parameter types, therapeutic regimens, administration routes, MSC dosages and adverse events during the MSC therapy. Trials’ quality was assessed for risk of bias following the instruction of Cochrane Handbook.Citation21
Outcome definition
Treatment efficacy was assessed in terms of National Institutes of Health Stroke Scale (NIHSS), Barthel index (BI), Fugl-Meyer Assessment (FMA) and Functional Independence Measure (FIM). The frequencies of adverse events were gathered and assessed for MSC therapy safety.
Statistical analysis
This meta-analysis was performed using Review Manager 5.3 (Cochrane Collaboration). The therapeutic efficacy was evaluated by odds ratio (OR) and presented with 95% CI. P<0.05 indicates differences with statistical significance. The appropriate analysis model was determined by analyzing the heterogeneity between trials by Cochran’s Q test.Citation22 Studies with I2<50% or P>0.1 were considered homogenous.
Publication bias was evaluated based on funnel plots. Sensitivity analysis on subgroups was also performed to assess the impact of MSC types, cell administration methods and patients’ characteristics on clinical outcomes.
Results
Search results
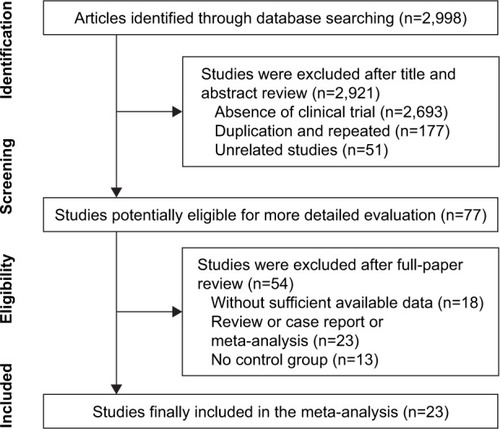
A total of 2,998 articles were initially identified, and 2,921 were excluded for lacking clinical trials (n=2,693), duplication and repetition (n=177) or being unrelated (n=51). The later detailed assessment further excluded 18 articles with insufficient data, 23 reviews or case reports or meta-analyses and 13 articles without control group. A total of 23 trialsCitation23–Citation45 with 1,279 IS patients were finally identified meeting the restrict inclusion criteria of this research ().
Figure 1 Flow diagram of the selection process.
Study and patient characteristics
After selection, all included trials were found to have been conducted in Asia. Two studies were conducted in Korea,Citation23,Citation35 two in IndiaCitation24,Citation25 and the rest of the included studies in China. MSCs were obtained from bone marrow in 18 studies,Citation23–Citation30,Citation32, Citation35–Citation37,Citation40–Citation45 from umbilical cord in three studiesCitation33,Citation34,Citation38 and from umbilical cord blood in two studies.Citation31,Citation39 Cells were administered through peripheral vein in 14 studies,Citation23–Citation27, Citation30,Citation32,Citation34,Citation35,Citation37,Citation40–Citation43 subarachnoid in five studies,Citation28,Citation29,Citation36,Citation44,Citation45 intrathecal in three studiesCitation31,Citation33,Citation39 and intracarotid artery in one study.Citation38 In total, 625 IS patients accepted MSC and RT combined therapy, and 654 patients were treated by RT alone. Detailed information about the involved studies and participants is summarized in and .
Table 1 Clinical information from the eligible trials in the meta-analysis
Table 2 Information of MSC therapy
Quality assessment
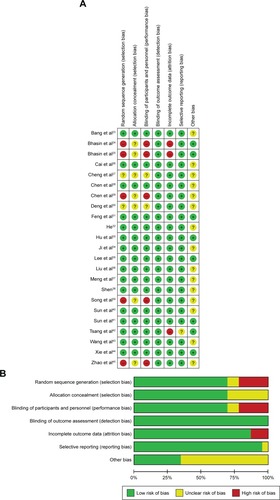
Bias risk of involved trials is shown in . Sixteen studies were determined as low risk, five researches were not truly randomized controlled trials and the other two studies did not have clear illustration of randomization procedures. Seven trials did not provide clear description of allocation and performance concealment. All the included studies were free of detection risk. Three trials missing the follow-up study were considered as high risk, and one study with selective reporting was considered as unclear risk.
Figure 2 (A) Risk-of-bias summary: review of authors’ judgments about each risk-of-bias item for included studies. (B) Risk-of-bias graph: review of authors’ judgments about each risk-of-bias item presented as percentages across all included studies.
Therapeutic efficacy assessments
Effectiveness of MSCs assessed by the NIHSS score
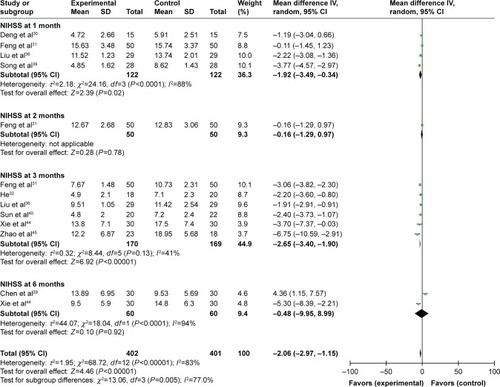
The analysis of involved trials showed that after MSC therapy, the NIHSS score was reduced in the first, second, third and sixth month after treatment (1 month: OR=−5.20, CI=−6.52 to −3.87, P<0.00001; 2 months: OR=−6.46, CI=−7.86 to −5.06, P<0.00001; 3 months: OR=−7.50, CI=−9.59 to −5.40, P<0.00001; 6 months: OR=−9.19, CI=−11.77 to −6.60, P<0.00001; Figure S1). As shown in , compared to the control group, the NIHSS score of the experimental group was lower in the first (OR=−1.92, CI=−3.49 to −0.34, P=0.02) and third month (OR=−2.65, CI=−3.40 to −1.90, P<0.00001).
Figure 3 Forest plot of the comparison of NIHSS scores between the experimental and control groups.
Abbreviations: IV, inverse variance; NIHSS, National Institutes of Health Stroke Scale; RT, routine treatment; MSC, mesenchymal stem cell.
Effectiveness of MSCs assessed by the BI score
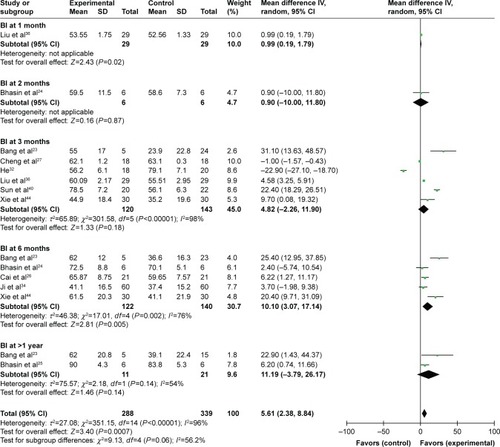
The postoperative BI score was increased after combined therapy in the first, second, third and sixth month and after 12 months (1 month: OR=30.14, CI=29.34–30.94, P<0.00001; 2 months: OR=15.50, CI=2.99–28.01, P=0.02; 3 months: OR=29.66, CI=24.12–35.20, P<0.00001; 6 months: OR=27.76, CI=13.24–42.28, P=0.0002; after 1 year: OR=45.79, CI=37.32–54.25, P<0.00001; Figure S2). In the comparison between patients treated by combined therapy and RT alone, the BI score in the combined therapy group was higher in the first and sixth month (1 month: OR=0.99, CI=0.19–1.79, P=0.02; 6 months: OR=10.10, CI=3.07–17.14, P=0.005; ).
Figure 4 Forest plot of the comparison of the BI scores between the experimental and control groups.
Abbreviations: IV, inverse variance; B1, Barthel index; RT, routine treatment; MSC, mesenchymal stem cell.
Effectiveness of MSCs assessed by the FMA score
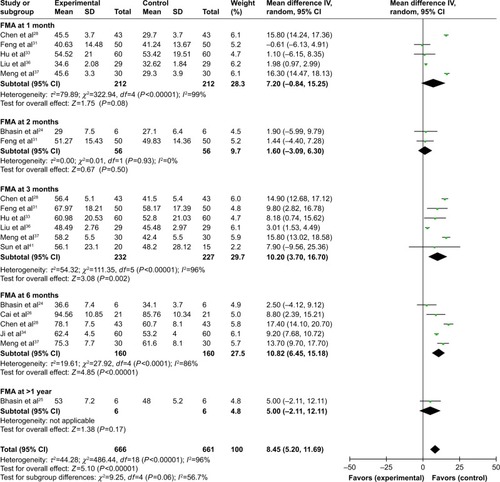
The FMA score after combined therapy was significantly increased in the first, second, third and sixth month, and after 12 months (1 month: OR=15.49, CI=7.51–23.47, P=0.0001; 2 months: OR=18.46, CI=7.11–29.82, P=0.001; 3 months: OR=27.00, CI=19.78–34.23, P<0.00001; 6 months: OR=39.26, CI=25.85–52.67, P<0.00001; after 1 year: OR=36.40, CI=29.31–43.49, P<0.00001; Figure S3). A comparison between the two groups indicated a significantly increased FMA score in the third and sixth month postoperation in the combined therapy group (3 months: OR=10.20, CI=3.70–16.70, P=0.002; 6 months: OR=10.82, CI=6.45–15.18, P<0.00001; ).
Figure 5 Forest plot of the comparison of FMA scores between the experimental and control groups.
Abbreviations: IV, inverse variance; FMA, Fugl-Meyer Assessment; RT, routine treatment; MSC, mesenchymal stem cell.
Effectiveness of MSCs assessed by the FIM score
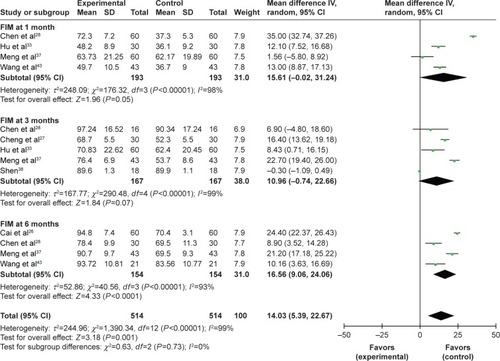
As shown in , the FIM score was increased after combined therapy, especially in the first, third and sixth month postoperation (1 month: OR=24.47, CI=7.14–41.80, P=0.006; 3 months: OR=24.05, CI=6.56–41.54, P=0.007; 6 months: OR=48.13, CI=32.04–64.23, P<0.00001; Figure S4). Meanwhile, the FIM score in the combined therapy group was higher than that of the control group in the first and sixth month (1 month: OR=15.61, CI=−0.02 to 31.24, P=0.05; 6 months: OR=16.56, CI=9.06–24.06, P<0.0001; ).
Figure 6 Forest plot of the comparison of the FIM scores between the experimental and control groups.
Abbreviations: IV, inverse variance; FIM, Functional Independence Measure; RT, routine treatment; MSC, mesenchymal stem cell.
Adverse event assessment
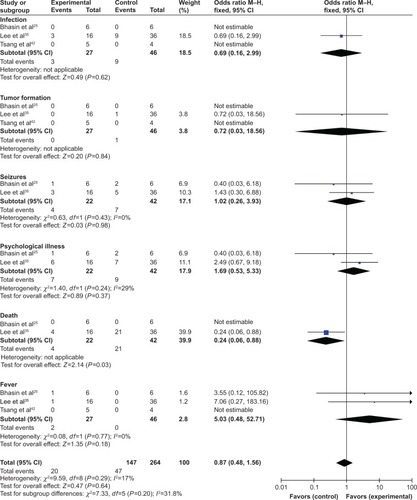
We evaluated the safety of MSC therapy in this meta-analysis. The most common side effects of MSC treatment were headache and fever, which usually subsided within 24 hours without treatment. No serious adverse events were reported in the involved studies (). However, the incidence of side effects in experimental and control groups was not compared in most included trials. Three studiesCitation25,Citation35,Citation42 conducted the comparison of adverse events including infection, tumor formation, seizures, psychological illness, death and fever. Except death, no significant difference was found for other indicators between the two groups (infection: OR=0.69, CI=0.16–2.99, P=0.62; tumor formation: OR=0.72, CI=0.03–18.56, P=0.84; seizures: OR=1.02, CI=0.26–3.93, P=0.98; psychological illness: OR=1.69, CI=0.53–5.33, P=0.37; death: OR=0.24, CI=0.06–0.88, P=0.03; fever: OR=5.03, CI=0.48–52.71, P=0.18; ).
Figure 7 Forest plot of the comparison of adverse events between the experimental and control groups.
Abbreviations: M–H, Mantel–Haenszel; RT, routine treatment; MSC, mesenchymal stem cell.
Publication bias
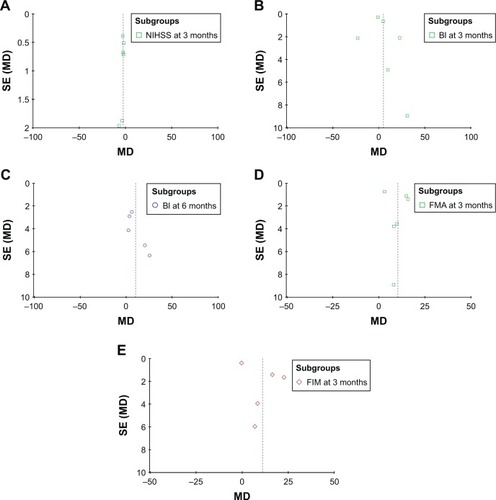
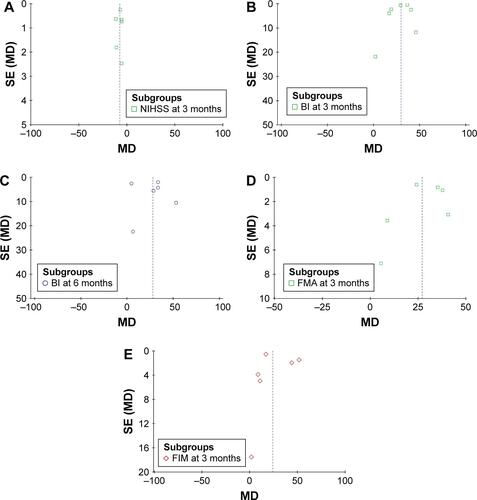
Based on the NIHSS,Citation31,Citation32,Citation36,Citation40,Citation44,Citation45 BI,Citation23,Citation24,Citation26,Citation27,Citation32,Citation34,Citation36,Citation40,Citation42,Citation44 FMACitation28,Citation31,Citation33,Citation36,Citation37,Citation41 and FIMCitation27,Citation28,Citation33,Citation37,Citation38,Citation42 data, funnel plots were drawn for the studies. The funnel plots were symmetrical, indicating no existence of publication bias ( and S5).
Figure 8 Funnel plot of the NIHSS (A), BI (B and C), FMA (D) and FIM (E) scores between the experimental and control groups.
Abbreviations: SE, standard error; MD, mean difference; NIHSS, National Institutes of Health Stroke Scale; BI, Barthel index; FMA, Fugl-Meyer Assessment; FIM, Functional Independence Measure.
Sensitivity analysis
To further evaluate the effects of clinical variables including cell types and different administration routes on clinical efficacy of patients with different characteristics, we performed subgroup analysis. Results showed that MSC therapy was more effective when infusion was performed through vein, and autogenous MSCs were superior to those derived from other sources, indicated by increased BI, FMA and FIM scores ().
Table 3 Subgroup analyses of NIHSS, BI, FMA and FIM between the experimental and control groups
Discussion
MSC transfusion has been considered as a promising option to treat IS due to its unique biological characteristics. Transfused MSCs can migrate to infarction area and induce angiogenesis,Citation46,Citation47 reduce neuron apoptosis,Citation48,Citation49 enhance axonal regeneration and rebuild synapses. Upon stimulating the release of cytokines and neurotrophic factors,Citation3,Citation50 such as brain-derived neurotrophic factor,Citation3 basic fibroblast growth factorCitation15 and vascular endothelial growth factor,Citation3,Citation51 MSCs also promote the differentiation of endogenous neural stem and progenitor cells. Most importantly, the low immunogenicity of MSCs reduces the possibility of graft-versus-host reaction.Citation1,Citation15
In recent years, several studies reported that MSC therapy is a safe and feasible treatment option for IS,Citation23–Citation45 but different clinical protocols among studies may bring different therapeutic effects. In this study, we performed an extensive and systematic analysis of published clinical trials to assure statistical reliability. Our meta-analysis revealed that compared to IS patients treated by RT alone, those treated by MSC and RT combined therapy exhibited more favorable therapeutic efficacy, indicated by decreased NIHSS and increased BI, FMA and FIM scores.
MSC therapy has been applied to treat refractory diseases for years with satisfied safety record,Citation52–Citation55 and our analysis showed that MSCs were safe in treating IS as well. No serious adverse events have been reported during MSC therapy. Most common side effects, including fever and headache, usually resolved naturally. However, relevant studies were insufficient, and the potential long-term toxicity and the risk of tumor formation are unknown, which usually take years to occur. More research evidence will be required to support the safety of combined therapy.
Therapeutic effects of MSC therapy may be affected by infusion routes, cell dosages, cell types and patients’ characteristics. We found that intravenous infusion is generally superior to subarachnoid injection in therapeutic effects, but there were also contradicted conclusions drawn from different researches. There are articles that claimed that local subarachnoid injection may deliver a larger number of transplanted MSCs to the stroke lesion thereby promoting nerve recovery and regeneration.Citation2,Citation56 However, the different routes of cell infusion did not make big difference in other researches,Citation57 which speculated that MSCs treat IS through releasing growth factors and antiapoptotic factors instead of homing to the nerve system.Citation3,Citation58 The treatment effect varies at different time points of detection, and dosages of transfused MSCs are a key factor in therapeutic strategy optimization. There are studies that showed that increased number of infused cells contributed to favorable clinical efficacy,Citation57 but currently published literature is still not sufficient to perform reliable statistical analysis. Sources of MSC may also associate with treatment outcomes. Based on our extracted data, autogenous MSCs were associated with increased BI and FIM score, indicating a better therapeutic effect than allogenic MSCs for IS. However, our data were not sufficient, and more research evidence is needed to support this conclusion. The optimal conduction time of cell delivery is also undetermined yet. Preclinical studies showed that early intervention leads to an obvious relief of neurological defects.Citation2,Citation59 Our subgroup analysis suggested no significant difference in outcomes between the acute and chronic phases of stroke.
Limitations
There are some limitations in this analysis. First of all, the numbers of involved studies and patients were small and the follow-up period was short, which may cause publication bias. Second, all trials included in this paper were mainly conducted in Asian countries. There were indeed several trials conducted in non-Asian countries included upon the first retrieve. However, no paper meeting our inclusion criteria has been produced based on these trials, and studies were excluded due to insufficient data, and being case reports, unrelated to MSC therapy or without control group. We will keep paying close attention to global studies in this field and carry out further analyses in our later studies. Third, our data were partly extracted from published papers rather than original patient records, which means we were not able to avoid the analytical bias based on the information presented in them. In addition, different trials evaluated the treatment efficacy by different outcomes, which have to be summarized using various scales when assessed in this study, leading to small sample sizes in each statistical analysis. Due to above limitations, future studies and generated data will be valuable to further verify the safety and efficacy of MSC therapy.
Conclusion
In summary, our analysis verified the safety and efficacy of MSC therapy for IS. It significantly mitigated neurological defects and improved life quality of IS patients, without causing serious adverse events. Therefore, MSC therapy is a promising treatment option for IS patients.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Supplementary materials
Figure S1 Forest plot of the comparison of NIHSS scores pre-and post-therapy.
Note: The random-effects meta-analysis model (inverse variance method) was used.
Abbreviations: IV, inverse variance; NIHSS, National Institutes of Health Stroke Scale.
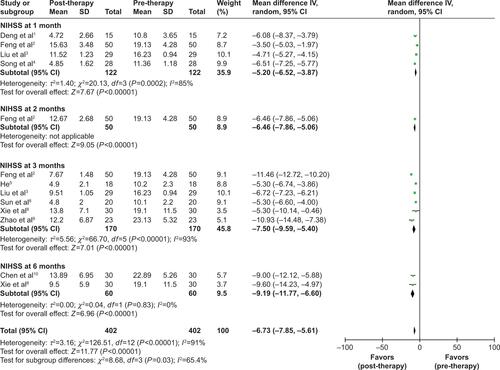
Figure S2 Forest plot of the comparison of BI scores pre- and post-therapy.
Note: The random-effects meta-analysis model (inverse variance method) was used.
Abbreviations: IV, inverse variance; BI, Barthel index.
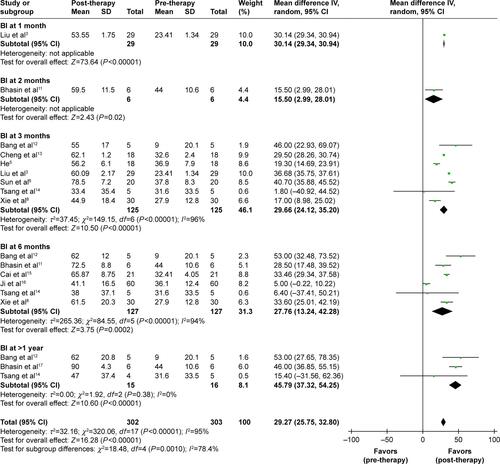
Figure S3 Forest plot of the comparison of FMA scores pre- and post-therapy.
Note: The random-effects meta-analysis model (inverse variance method) was used.
Abbreviations: IV, inverse variance; FMA, Fugl-Meyer Assessment.
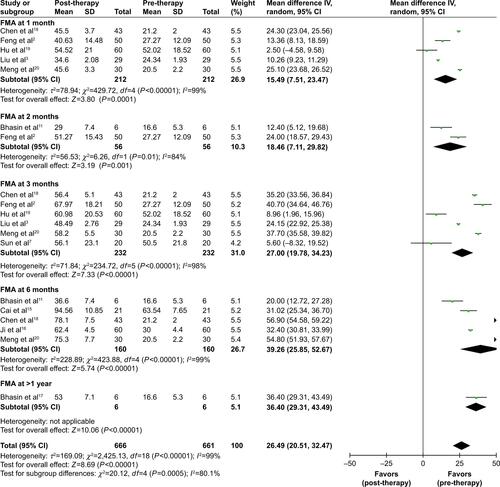
Figure S4 Forest plot of the comparison of FIM scores in pre- and post-therapy.
Note: The random-effects meta-analysis model (inverse variance method) was used.
Abbreviations: IV, inverse variance; FIM, Functional Independence Measure.
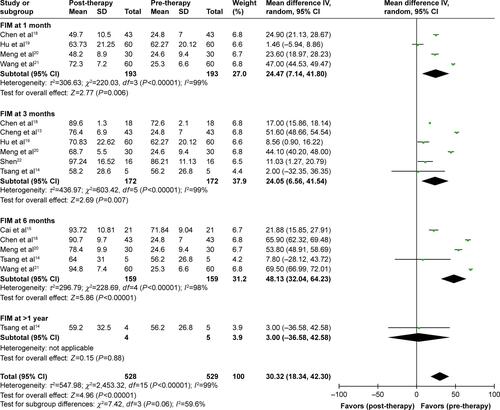
Figure S5 Funnel plot of the NIHSS (A), BI (B and C), FMA (D) and FIM (E) scores pre- and post-therapy.
Note: Parameters were discussed in over five studies which were included in bias analyses.
Abbreviations: SE, standard error; MD, mean deviation; NIHSS, National Institutes of Health Stroke Scale; BI, Barthel index; FMA, Fugl-Meyer Assessment; FIM, Functional Independence Measure.
References
- DengYGZhangZPYuWClinical efficacy of salvia miltiorrhiza injection combined with marrow stem cells in treatment of cerebral infarctionPract J Cardiac Cereb Pneumal Vasc Dis2012203424425
- FengYTianGPLiLZhouJEffect of human umbilical cord blood-derived mesenchymal stem cells in the treatment of cerebral infarctionPract J Cardiac Cereb Pneumal Vasc Dis20142212830
- LiuDHHanBJHongSSTransplanting autologous mesenchymal nerve stem cells in the treatment of cerebral infarctionChin J Phys Med Rehabil2014366425428
- SongCWWangPHuXQClinical efficacy of umbilical cord blood mesenchymal stem cells transplantation in the treatment of cerebral infarctionJ Clin Ration Drug Use2013626970
- HeZDThe functional mechanism of mesenchymal stem cell transplantation therapy for patients with cerebral infarctionAsia Pac Tradit Med2012812126127
- SunHBXiaSMYangSSThe clinical effect of rhG-CSF combined transplantation of autologous bone marrow mesenchymal stem cells on acute cerebral infarctionJ Chin Phys2008104441443
- SunSCWangCLuoJSBone marrow mesenchymal stem cell transplantation improved the neurological function of 35 patients with sequelae of strokeChina Med Eng20132161417
- XieXFLiuSYJinGHQuXHZhangKNWuXMClinical analysis of autologous bone marrow mesenchymal stem cell transplantation for treating cerebral infarctionLab Med Clin2014112129555957
- ZhaoXLWangYZhangCXTanJStudy of bone marrow mesenchymal stem cells in the treatment of strokeGlobal Chin Med20136S2157
- ChenWMZouQYLuJJReinfusion of autologous bone marrow mesenchymal stem cells for treatment of stroke in 30 casesChin J Tissue Eng Res2012163260716075
- BhasinAPadma SrivastavaMVMohantySBhatiaRKumaranSSBoseSStem cell therapy: a clinical trial of strokeClin Neurol Neurosurg201311571003100823183251
- BangOYLeeJSLeePHLeeGAutologous mesenchymal stem cell transplantation in stroke patientsAnn Neurol200557687488215929052
- ChengYWangDLiuHBBone marrow mesenchymal stem cells transplantation in the recovery phase of ischemic cerebral stroke patientsChin J Transplant201373141144
- TsangKSNgCPSZhuXLPhase I/II randomized controlled trial of autologous bone marrow-derived mesenchymal stem cell therapy for chronic strokeWorld J Stem Cells20179813314328928910
- CaiMSShenCLZengLHHuangXQSongCWEffect of stem cell transplantation on serum homocysteine, CRP and BDNF in patients with ischemic strokeChin J Biochem Pharm20153599193
- JiXZhaoHTZhangXBClinical analysis of mesenchymal stem cells for treatment of stroke in 60 casesJ Xianning Univ20122613132
- BhasinAKumaranSSBhatiaRMohantySSrivastavaMVPSafety and feasibility of autologous mesenchymal stem cell transplantation in chronic stroke in Indian patients. A four-year follow upJ Stem Cells Regen Med2017131141928684893
- ChenWDLiJTZhangXBClinical analysis of bone marrow mesenchymal stem cells transplantation in the treatment of cerebral infarctionJilin Med J201233214522
- HuQCaoMYLiRFJiangHWGeLTSafety and efficacy on the treatment of cerebral infarction with umbilical cord mesenchymal stem cellsMed J Wuhan Univ20133415770
- MengXGZhuSWGaoHTreatment of cerebral infarction using autologous marrow mesenchymal stem cells transplantation: a six-month follow-upJ Clin Rehabil Tissue Eng Res2009133263746378
- WangXZhangZBJiaFRYangHA clinical study on treatment of cerebral infarction using autologous marrow mesenchymal stem cells intervening transplantationJilin Med J2014352237239
- ShenDPUmbilical cord mesenchymal stem cell early single transplantation in treatment of neurological recovery in acute cerebral infarctionChin J Trauma Disabil Med20152322628
Disclosure
The authors report no conflicts of interest in this work.
References
- ChenLZhangGKhanAAGuoXGuYClinical efficacy and meta-analysis of stem cell therapies for patients with brain ischemiaStem Cells Int20162016612957927656217
- KumarAPrasadMJaliVPBone marrow mononuclear cell therapy in ischaemic stroke: a systematic reviewActa Neurol Scand2017135549650627558274
- CaoWLiPEffectiveness and safety of autologous bone marrow stromal cells transplantation after ischemic stroke: a meta-analysisMed Sci Monit2015212190219526215395
- ReisCWilkinsonMReisHA look into stem cell therapy: exploring the options for treatment of ischemic strokeStem Cells Int20172017326735229201059
- HsuanYCLinCHChangCPLinMTMesenchymal stem cell-based treatments for stroke, neural trauma, and heat strokeBrain Behav2016610e0052627781140
- ZhouMWangHZhuJCause-specific mortality for 240 causes in China during 1990–2013: a systematic subnational analysis for the Global Burden of Disease Study 2013Lancet20163871001525127226510778
- CramerSCStradlingDBrownDMOrganization of a United States county system for comprehensive acute stroke careStroke20124341089109322282882
- BanerjeeSBentleyPHamadyMIntra-arterial immunoselected CD34+ stem cells for acute ischemic strokeStem Cells Transl Med20143111322133025107583
- BoySSauerbruchSKraemerMMobilisation of hematopoietic CD34+ precursor cells in patients with acute stroke is safe – results of an open-labeled non randomized phase I/II trialPLoS One201168e2309921887230
- KalladkaDSindenJPollockKHuman neural stem cells in patients with chronic ischaemic stroke (PISCES): a phase 1, first-in-man studyLancet20163881004678779627497862
- QiaoLYHuangFJZhaoMA two-year follow-up study of cotransplantation with neural stem/progenitor cells and mesenchymal stromal cells in ischemic stroke patientsCell Transplant201423Suppl 1S65S7225333752
- LiaoSLuoCCaoBEndothelial progenitor cells for ischemic stroke: update on basic research and applicationStem Cells Int20172017219343228900446
- HessDCWechslerLRClarkWMSafety and efficacy of multipotent adult progenitor cells in acute ischaemic stroke (MASTERS): a randomised, double-blind, placebo-controlled, phase 2 trialLancet Neurol201716536036828320635
- PrasadKSharmaAGargAIntravenous autologous bone marrow mononuclear stem cell therapy for ischemic stroke: a multicentric, randomized trialStroke201445123618362425378424
- ZhouCYangBTianYImmunomodulatory effect of human umbilical cord Wharton’s jelly-derived mesenchymal stem cells on lymphocytesCell Immunol20112721333822004796
- GhorbaniSTiraihiTSoleimaniMDifferentiation of mesenchymal stem cells into neuron-like cells using composite 3D scaffold combined with valproic acid inductionJ Biomater Appl201832670271529169271
- SarmahDAgrawalVRanePMesenchymal stem cell therapy in ischemic stroke: a meta-analysis of preclinical studiesClin Pharmacol Ther Epub2017111
- SammaliEAliaCVeglianteGIntravenous infusion of human bone marrow mesenchymal stromal cells promotes functional recovery and neuroplasticity after ischemic stroke in miceSci Rep201771696228761170
- SasakiYSasakiMKataoka-SasakiYSynergic effects of rehabilitation and intravenous infusion of mesenchymal stem cells after stroke in ratsPhys Ther201696111791179827174259
- Rosado-de-CastroPHPimentel-CoelhoPMda FonsecaLMde FreitasGRMendez-OteroRThe rise of cell therapy trials for stroke: review of published and registered studiesStem Cells Dev201322152095211123509917
- ZengXZhangYKwongJSThe methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: a systematic reviewJ Evid Based Med20158121025594108
- JacksonDWhiteIRRileyRDQuantifying the impact of between-study heterogeneity in multivariate meta-analysesStat Med201231293805382022763950
- BangOYLeeJSLeePHLeeGAutologous mesenchymal stem cell transplantation in stroke patientsAnn Neurol200557687488215929052
- BhasinAPadma SrivastavaMVMohantySBhatiaRKumaranSSBoseSStem cell therapy: a clinical trial of strokeClin Neurol Neurosurg201311571003100823183251
- BhasinAKumaranSSBhatiaRMohantySSrivastavaMVPSafety and feasibility of autologous mesenchymal stem cell transplantation in chronic stroke in Indian patients. A four-year follow upJ Stem Cells Regen Med2017131141928684893
- CaiMSShenCLZengLHHuangXQSongCWEffect of stem cell transplantation on serum homocysteine, CRP and BDNF in patients with ischemic strokeChin J Biochem Pharm20153599193
- ChengYWangDLiuHBBone marrow mesenchymal stem cells transplantation in the recovery phase of ischemic cerebral stroke patientsChin J Transplant201373141144
- ChenWDLiJTZhangXBClinical analysis of bone marrow mesenchymal stem cells transplantation in the treatment of cerebral infarctionJilin Med J201233214522
- ChenWMZouQYLuJJReinfusion of autologous bone marrow mesenchymal stem cells for treatment of stroke in 30 casesChin J Tissue Eng Res2012163260716075
- DengYGZhangZPYuWClinical efficacy of salvia miltiorrhiza injection combined with marrow stem cells in treatment of cerebral infarctionPract J Cardiac Cereb Pneumal Vasc Dis2012203424425
- FengYTianGPLiLZhouJEffect of human umbilical cord blood-derived mesenchymal stem cells in the treatment of cerebral infarctionPract J Cardiac Cereb Pneumal Vasc Dis20142212830
- HeZDThe functional mechanism of mesenchymal stem cell transplantation therapy for patients with cerebral infarctionAsia Pac Tradit Med2012812126127
- HuQCaoMYLiRFJiangHWGeLTSafety and efficacy on the treatment of cerebral infarction with umbilical cord mesenchymal stem cellsMed J Wuhan Univ20133415770
- JiXZhaoHTZhangXBClinical analysis of mesenchymal stem cells for treatment of stroke in 60 casesJ Xianning Univ20122613132
- LeeJSHongJMMoonGJLeePHAhnYHBangOYA long-term follow-up study of intravenous autologous mesenchymal stem cell transplantation in patients with ischemic strokeStem Cells20102861099110620506226
- LiuDHHanBJHongSSTransplanting autologous mesenchymal nerve stem cells in the treatment of cerebral infarctionChin J Phys Med Rehabil2014366425428
- MengXGZhuSWGaoHTreatment of cerebral infarction using autologous marrow mesenchymal stem cells transplantation: a six-month follow-upJ Clin Rehabil Tissue Eng Res2009133263746378
- ShenDPUmbilical cord mesenchymal stem cell early single transplantation in treatment of neurological recovery in acute cerebral infarctionChin J Trauma Disabil Med20152322628
- SongCWWangPHuXQClinical efficacy of umbilical cord blood mesenchymal stem cells transplantation in the treatment of cerebral infarctionJ Clin Ration Drug Use2013626970
- SunHBXiaSMYangSSThe clinical effect of rhG-CSF combined transplantation of autologous bone marrow mesenchymal stem cells on acute cerebral infarctionJ Chin Phys2008104441443
- SunSCWangCLuoJSBone marrow mesenchymal stem cell transplantation improved the neurological function of 35 patients with sequelae of strokeChina Med Eng20132161417
- TsangKSNgCPSZhuXLPhase I/II randomized controlled trial of autologous bone marrow-derived mesenchymal stem cell therapy for chronic strokeWorld J Stem Cells20179813314328928910
- WangXZhangZBJiaFRYangHA clinical study on treatment of cerebral infarction using autologous marrow mesenchymal stem cells intervening transplantationJilin Med J2014352237239
- XieXFLiuSYJinGHQuXHZhangKNWuXMClinical analysis of autologous bone marrow mesenchymal stem cell transplantation for treating cerebral infarctionLab Med Clin2014112129555957
- ZhaoXLWangYZhangCXTanJStudy of bone marrow mesenchymal stem cells in the treatment of strokeGlobal Chin Med20136S2157
- BorlonganCVGloverLETajiriNKanekoYFreemanTBThe great migration of bone marrow-derived stem cells toward the ischemic brain: therapeutic implications for stroke and other neurological disordersProg Neurobiol201195221322821903148
- ZacharekAShehadahAChenJComparison of bone marrow stromal cells derived from stroke and normal rats for stroke treatmentStroke201041352453020056925
- WakabayashiKNagaiASheikhAMTransplantation of human mesenchymal stem cells promotes functional improvement and increased expression of neurotrophic factors in a rat focal cerebral ischemia modelJ Neurosci Res20108851017102519885863
- LanzaCMorandoSVociANeuroprotective mesenchymal stem cells are endowed with a potent antioxidant effect in vivoJ Neurochem200911051674168419619133
- HokariMKurodaSShichinoheHYanoSHidaKIwasakiYBone marrow stromal cells protect and repair damaged neurons through multiple mechanismsJ Neurosci Res20088651024103518030676
- OndaTHonmouOHaradaKHoukinKHamadaHKocsisJDTherapeutic benefits by human mesenchymal stem cells (hMSCs) and Ang-1 gene-modified hMSCs after cerebral ischemiaJ Cereb Blood Flow Metab200828232934017637706
- LinBLChenJFQiuWHAllogeneic bone marrow-derived mesenchymal stromal cells for hepatitis B virus-related acute-on-chronic liver failure: a randomized controlled trialHepatology201766120921928370357
- AhnSYChangYSKimJHSungSIParkWSTwo-year follow-up outcomes of premature infants enrolled in the phase I trial of mesenchymal stem cells transplantation for bronchopulmonary dysplasiaJ Pediatr201718549.e254.e228341525
- ZhangYCLiuWFuBSTherapeutic potentials of umbilical cord-derived mesenchymal stromal cells for ischemic-type biliary lesions following liver transplantationCytotherapy201719219419927964826
- WangHLiYWuQXuCLiuQCombination of butylphthalide with umbilical mesenchymal stem cells for the treatment of delayed encephalopathy after carbon monoxide poisoningMedicine20169549e541227930518
- LosordoDWHenryTDDavidsonCIntramyocardial, autologous CD34+ cell therapy for refractory anginaCirc Res2011109442843621737787
- JeongHYimHWChoYSEfficacy and safety of stem cell therapies for patients with stroke: a systematic review and single arm meta-analysisInt J Stem Cells201472636925473443
- WanHLiFZhuLWangJYangZPanYUpdate on therapeutic mechanism for bone marrow stromal cells in ischemic strokeJ Mol Neurosci201452217718524048741
- YangBStrongRSharmaSTherapeutic time window and dose response of autologous bone marrow mononuclear cells for ischemic strokeJ Neurosci Res201189683383921412816