
Abstract
Background
This study investigated the factors associated with coronary artery stenosis in outpatients. Furthermore, the usefulness of maximum carotid intima–media thickness (maximum-IMT) as a surrogate marker of coronary artery stenosis was evaluated.
Methods
We conducted a single-center retrospective study. A total of 601 outpatients (338 males; 263 females; mean age, 69.8±10.0 years) who underwent coronary computed tomography angiography between April 2006 and March 2012 were analyzed. The associations between coronary artery stenosis (≥75%) as determined by coronary computed tomography angiography and clinical and laboratory parameters were evaluated by multivariate logistic regression. Validation of maximum-IMT as measured by ultrasonography as a surrogate marker of coronary artery stenosis was analyzed by receiver operating characteristic (ROC) curve analysis.
Results
The estimated glomerular filtration rate (eGFR: mL/min/1.73 m2) (odds ratio [OR] 0.985, p<0.01), diabetes mellitus (OR 1.98, p<0.05), and maximum-IMT (mm) (OR 1.76, p<0.01) were significantly associated with coronary artery stenosis (≥75%). In analysis of each group categorized by identified factors, such as renal impairment (eGFR <60 mL/min/1.73 m2) and diabetes mellitus, the ROC curve of maximum-IMT was significant in the group of patients with diabetes mellitus without renal impairment (p<0.01) (cutoff value of maximum-IMT, 2.0 mm; sensitivity, 0.74; and specificity, 0.54) but not in other groups.
Conclusion
Renal impairment, diabetes mellitus, and increased maximum-IMT may be significant risk factors of coronary artery stenosis. Maximum-IMT as measured by ultrasonography may be a useful surrogate marker for coronary artery stenosis in patients with diabetes mellitus without renal impairment but not in other patients.
Introduction
Coronary artery disease due to coronary artery stenosis is a major cause of death worldwide, including Japan.Citation1 The severity of coronary artery stenosis correlates with major cardiac events, such as death by cardiovascular disease, myocardial infarction, and unstable angina.Citation2 Therefore, prevention, detection at an early stage, and treatment of coronary artery stenosis are important to protect against development and progression of cardiovascular disease.
Cardiac catheterization is considered as the gold standard for screening of coronary artery stenosis because of its high sensitivity and specificity.Citation3 Additionally, cardiac catheterization subsequently allows performance of coronary intervention if indicated. However, cardiac catheterization is invasive and may have risks of adverse events, including life-threatening thrombosis resulting in cerebral infarction, myocardial infarction and mesenteric artery occlusion, bleeding, and cardiac tamponade by catheter manipulation.Citation4 Therefore, non-invasive examinations for coronary artery stenosis are required.
Coronary computed tomography angiography has recently emerged as a non-invasive imaging modality for assessing coronary artery stenosis. A recent meta-analysis reported that coronary computed tomography angiography has comparable sensitivity and specificity to coronary catheterization.Citation5 However, the indication for coronary computed tomography angiography is limited to patients who are highly suspected as having coronary artery stenosis by symptoms, such as chest pain and tightness, electrocardiographic abnormalities, high risk factors of coronary artery disease because of exposure to contrast agents, and X-ray radiation, which may not be beneficial for patients.Citation6
Recently, several studies reported that carotid intima–media thickness (IMT) as measured by ultrasonography was correlated with systemic atherosclerosisCitation7,Citation8 and coronary artery disease.Citation9,Citation10 Several previous studies have also reported that maximum-IMT is a predictor of coronary artery stenosis in patients with diabetes mellitus.Citation11–Citation13 Evaluation of maximum-IMT as measured by ultrasonography is simple, non-invasive, and repeatable. However, a few studies have examined the utility of maximum-IMT with ultrasonography in various populations, including patients with renal impairment.
Therefore, in this study, we analyzed the association of factors, such as clinical and laboratory parameters, including maximum-IMT as measured by ultrasonography, with coronary artery stenosis in outpatients. Furthermore, we evaluated the usefulness of maximum-IMT as a surrogate marker of coronary artery stenosis in each group categorized by identified risk factors for coronary artery stenosis in outpatients.
Methods
Patients
We retrospectively analyzed clinical and laboratory data of patients who had regularly visited Chiba Prefectural Togane Hospital and underwent coronary computed tomography angiography between April 2006 and March 2012. Coronary computed tomography angiography was performed to examine coronary arteries for the following reasons: chest symptoms, ischemic change on an electrocardiogram, positive exercise stress test, left ventricular wall motion abnormalities on echocardiography, and carotid artery plaques. In all of these patients, carotid artery ultrasonography was routinely performed for screening the severity of systemic atherosclerosis. Exclusion criteria were patients who had known cardiovascular disease and those receiving renal replacement therapy.
Study protocol
This study was a single-center, retrospective, cross-sectional study. This study was performed in accordance with the ethical principles contained in the Declaration of Helsinki and was approved by the ethics committee of Chiba Cerebral and Cardiovascular Center. Patients’ consent to review their medical records was not required by the Ethics Committee of Chiba Cerebral and Cardiovascular Center because this study examined a retrospective cohort by analyzing the past medical history. The patients’ data were treated carefully to keep confidentiality. Information on this cohort study, including the patients’ right to opt out, was uploaded to the website of Chiba Cerebral and Cardiovascular Center. Laboratory data obtained within 1 month before coronary computed tomography angiography and carotid ultrasound data obtained within 3 months before and after coronary computed tomography angiography were used for analysis. Significant factors that were associated with coronary artery stenosis were analyzed using multivariate logistic regression analysis. Diagnostic accuracy of maximum-IMT for detecting coronary artery stenosis was analyzed using receiver operating characteristic (ROC) curve analysis.
Laboratory methods
Blood and urinary parameters were determined by the Department of Clinical Laboratory, Chiba Prefectural Togane Hospital. Serum glycated hemoglobin (HbA1c) levels are shown as National Glycohemoglobin Standardization Program values. The estimated glomerular filtration rate (eGFR) was calculated using a modified version of the Modification of Diet in Renal Disease formula of the Japanese Society of Nephrology as follows: eGFR (mL/min/1.73 m2)=194×age−0.287×serum creatinine−1.094 (multiplied by 0.739 for females).Citation14 Hypertension was defined as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg or current use of antihypertensive agents. Diabetes mellitus was defined as HbA1c levels ≥6.5% or use of oral hypoglycemic agents and/or insulin therapy.
Assessment of coronary artery stenosis by coronary computed tomography angiography
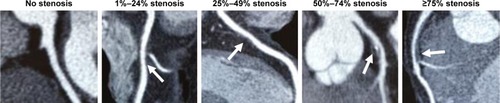
The degree of coronary artery stenosis was assessed by coronary computed tomography angiography using a 256-slice multidetector computed tomography scanner (Brilliance iCT; Phillips Healthcare, Cleveland, OH, USA; slice collimation, 2×128×0.625 mm3; gantry rotation time, 270 ms) at Chiba-Nishi General Hospital (an affiliated hospital of Chiba Prefectural Togane Hospital). Each coronary computed tomography angiography image was analyzed by two or more experienced cardiologists. In the case where cardiologists had different judgments, interpretation of coronary computed tomography angiography was carefully determined by a conference of cardiologists. The severity of coronary artery stenosis was visually categorized as no stenosis, 1%–24% stenosis, 25%–49% stenosis, 50%–74% stenosis, and ≥75% stenosis ().Citation15 Patients with at least one coronary artery stenotic lesion ≥75% were considered to have significant coronary artery stenosis.Citation16
Figure 1 Visual quantitative grading of coronary artery stenosis using coronary computed tomography angiography. The severity of coronary artery stenosis (arrows) was visually categorized as no stenosis, 1%–24% stenosis, 25%–49% stenosis, 50%–74% stenosis, and ≥75% stenosis. Patients with at least one coronary artery stenotic lesion ≥75% were considered to have significant coronary artery stenosis.
Evaluation of maximum-IMT using ultrasonography
Maximum-IMT was measured using B-mode ultrasound imaging with a 12-MHz linear transducer (Aplio TA700; Toshiba, Tokyo, Japan) at Chiba Prefectural Togane Hospital. Carotid IMT was measured as the distance between two parallel echogenic lines representing the lumen–intima interface and media–adventitia interface on the posterior wall of the artery ().Citation17 The maximum-IMT was defined as the greatest carotid IMT in observable areas on both sides of the common carotid artery, carotid bulb, and internal carotid artery (). All scans were performed by experienced laboratory technicians. In analysis of the relationship between maximum-IMT and the prevalence of coronary artery stenosis, maximum-IMT was categorized into the following five grades: <1.1 mm, 1.1–2.0 mm, 2.1–3.0 mm, 3.1–4.0 mm, and ≥4.1 mm. This categorization was based on the finding that maximum-IMT was reported to be less than 1.1 mm in healthy Japanese subjects.Citation18
Figure 2 Longitudinal B-mode ultrasound image of the common carotid artery.
Abbreviation: IMT, intima–media thickness.

Statistical analysis
Statistical analysis was performed using JMP 11 (SAS Institute Inc., Cary, NC, USA). Data are expressed as mean±standard deviation for continuous variables and as counts and percentages for categorical variables. Comparisons of component ratios were performed using Fisher’s exact test. Comparisons of clinical parameters between the two groups were performed using the Mann–Whitney U-test. Logistic regression analysis was used to detect significant predictors of coronary artery stenosis. Parameters that were significantly associated with coronary artery stenosis in univariate logistic regression analysis were included in multivariate logistic regression analysis. The relationship between the category of maximum-IMT and the prevalence of coronary artery stenosis was evaluated by Fisher’s exact test. The ability of maximum-IMT to predict coronary artery stenosis was examined by ROC curve analysis. The area under the ROC curve and sensitivity and specificity were calculated for detecting coronary artery stenosis. For all tests, p-values less than 0.05 were considered statistically significant.
Results
Patients’ characteristics
Patients’ characteristics and medications are shown in . A flow diagram of analyzed patients is shown in . A total of 601 patients (338 males, 263 females, mean age: 69.8±10.0 years) underwent coronary computed tomography angiography during the observation period. The reasons for undergoing coronary computed tomography angiography were chest symptoms in 80 (13.3%) patients, electrocardiographic abnormalities in 49 (8.2%) patients, cardiac wall motion abnormalities on an echocardiogram in 169 (28.1%) patients, and carotid artery plaques in 303 (50.4%) patients. Coronary computed tomography angiography showed that 167 (27.8%) patients had coronary artery stenosis of ≥75%. Among these 167 patients, 158 (94.6%) underwent coronary angiography. Finally, 136 (81.4%) patients underwent per-cutaneous coronary intervention and seven (4.2%) received coronary artery bypass graft surgery ().
Figure 3 Flow diagram of the analyzed patients.
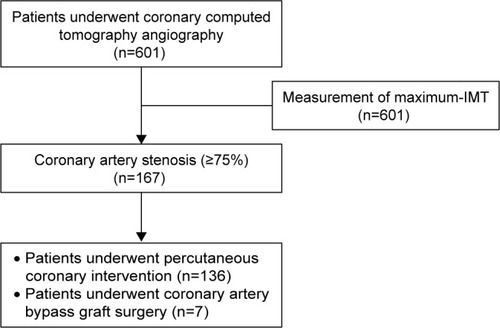
Table 1 Patients’ characteristics (n=601)
Factors associated with coronary artery stenosis
Multivariate logistic regression analysis showed that an eGFR (odds ratio [OR] 0.985, 95% confidence interval [CI] 0.975–0.996; p<0.01), diabetes mellitus (OR 1.98, 95% CI 1.14–3.53; p<0.05), and maximum-IMT (OR 1.76, 95% CI 1.30–2.40; p<0.05) were significant factors associated with coronary artery stenosis (≥75%) in all patients (). The OR of coronary artery stenosis (≥75%) was shown to be increased by 1.76-fold for every 1 mm increase in maximum-IMT ().
Table 2 Univariate and multivariate logistic regression analyses of the variables associated with the presence of coronary artery stenosis of ≥75% in all patients (n=167)
Relationship between maximum-IMT and the prevalence of coronary artery stenosis in each group categorized by renal impairment and diabetes mellitus
The degree of maximum-IMT in all of the patients is shown in . eGFR, diabetes mellitus, and maximum-IMT were significant factors associated with coronary artery stenosis (≥75%). Therefore, validation of maximum-IMT as a surrogate marker of coronary artery stenosis was conducted in each group categorized by the presence or absence of renal impairment (cutoff value: eGFR, 60 mL/min/1.73 m2) and diabetes mellitus. Patients’ characteristics categorized by the presence or absence of diabetes mellitus and renal impairment are shown in . The degree of maximum-IMT was significantly associated with coronary artery stenosis in the group of patients with diabetes mellitus (+)/renal impairment (−) (p<0.001), but no association was observed in other groups (). Notably, the prevalence of coronary artery stenosis increased to approximately 50%, even in the lower grade of maximum-IMT thickness in patients with diabetes mellitus and renal impairment ().
Figure 4 Associations between the degree of maximum-IMT and the prevalence of coronary artery stenosis (≥75%) as determined with coronary computed tomography angiography in each group categorized by the presence or absence of diabetes mellitus and renal impairment.
Abbreviation: IMT, intima–media thickness.
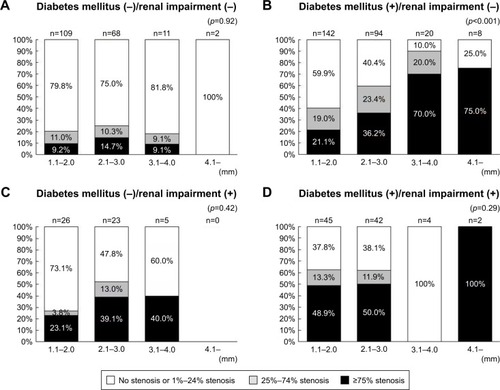
Table 3 Degree of maximum-IMT
Table 4 Patients’ characteristics categorized by the presence or absence of diabetes mellitus and renal impairment
Diagnostic accuracy of maximum-IMT thickness for detecting coronary artery stenosis
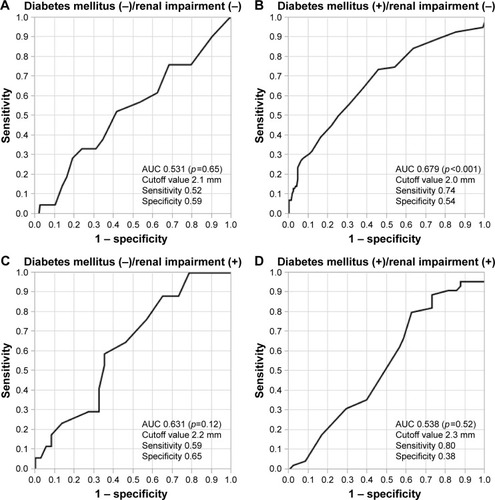
The ROC curve of maximum-IMT thickness for detecting coronary artery stenosis was significant in the group of patients with diabetes mellitus (+)/renal impairment (−) (p<0.001, ). In this group, the area under the curve (AUC) for maximum-IMT thickness for predicting coronary artery stenosis was 0.679 (95% CI 0.607–0.750) and the cutoff value with the greatest sensitivity and specificity for maximum-IMT thickness was 2.0 mm (sensitivity, 0.74; specificity, 0.54) (). ROC curves of maximum-IMT thickness for detecting coronary artery stenosis were not significant in other groups of patients, such as those with diabetes mellitus (−)/renal impairment (−), diabetes mellitus (−)/renal impairment (+), and diabetes mellitus (+)/renal impairment (+) ().
Figure 5 ROC analysis for predicting coronary artery stenosis of ≥75% for each group categorized by the presence or absence of diabetes mellitus and renal impairment.
Abbreviations: AUC, area under the curve; ROC, receiver operating characteristic.
Discussion
In this study, we investigated the factors that are associated with coronary artery stenosis and validation of maximum-IMT as measured by ultrasonography as a surrogate marker of coronary artery stenosis. We found that renal impairment (decreased eGFR), diabetes mellitus, and increased maximum-IMT were significantly associated with coronary artery stenosis (≥75%) as assessed by coronary computed tomography angiography. We also found that the degree of maximum-IMT was associated with the prevalence of coronary artery stenosis (≥75%) in patients with diabetes mellitus without renal impairment but not in other groups of patients. These results suggested that maximum-IMT as measured by ultrasonography could be a surrogate marker for coronary artery stenosis in ≥75% in patients with diabetes mellitus without renal impairment.
Several studies have reported that renal impairment and diabetes mellitus are strong risk factors for cardiovascular disease. Diabetes mellitus increases the risk of cardiovascular disease by 3-fold compared with the general population.Citation19 The degree of renal impairment is associated with an increase in the prevalence of cardiovascular disease.Citation20,Citation21 Additionally, diabetes mellitus and renal impairment synergistically increase the risk for developing cardiovascular disease.Citation22 In our study, diabetes mellitus and renal impairment (decreased eGFR) were significant risk factors for coronary artery stenosis (≥75%). These results are consistent with previous resultsCitation19–Citation22 and suggest that coronary artery stenosis of these patients should be carefully monitored. In this study, 85.6% (143/156) of patients who had coronary artery stenosis (≥75%) that was detected by coronary computed tomography angiography required catheter intervention. This finding indicates that computed tomography angiography has high sensitivity and specificity for screening coronary artery stenosis as previously reported.Citation5
Maximum-IMT is an established surrogate maker of atherosclerosis.Citation7,Citation8 Several studies have also reported that increased maximum-IMT is significantly associated with the prevalence coronary artery stenosis in patients with diabetes mellitus.Citation11–Citation13 In these studies, the AUCs of maximum-IMT as measured by ultrasonography for the presence of coronary artery stenosis were reported to be 0.71–0.73.Citation11–Citation13 In the present study, the AUC of maximum-IMT in the group of patients with diabetes mellitus without renal impairment was 0.68, which is comparable with the results of previous studies.Citation11–Citation13 Taken together, these findings suggest that maximum-IMT as measured by ultrasonography is a useful surrogate marker of coronary artery stenosis in patients with diabetes mellitus without renal impairment. However, the degree of maximum-IMT was not associated with the prevalence of coronary artery stenosis (≥75%) in patients with diabetes mellitus (−)/renal impairment (−), diabetes mellitus (−)/renal impairment (+), and diabetes mellitus (+)/renal impairment (+). Regardless of a lower category of maximum-IMT, a high prevalence of coronary artery stenosis was observed in patients with diabetes mellitus (+)/renal impairment (+). Physicians should note this discrepancy between coronary artery stenosis and maximum-IMT when they care for patients with diabetes mellitus and renal impairment. Monckeberg’s sclerosis, which is characterized by vascular medial hyperplasia, sclerosis, and calcification, is frequently observed.Citation23 A previous study showed that a reduced eGFR was associated with increased carotid arterial stiffness without progression of intimal disease, such as increased IMT or plaque formation.Citation24 Additionally, the eGFR is not associated with an increased IMT after adjusting for traditional cardiovascular disease risk factors.Citation25,Citation26 Taken together, these findings suggest that maximum-IMT is not a useful surrogate marker of coronary artery stenosis in patients with renal impairment. Diabetes mellitus and renal impairment synergistically increase the risk of coronary artery stenosis by different mechanisms. Further studies to investigate the mechanism of development coronal artery stenosis and maximum-IMT in diabetes mellitus with renal impairment are required.
This study has several advantages compared with previous studies.Citation11–Citation13 First, our sample size was larger than that of previous studies.Citation11–Citation13 Second, this study analyzed a diverse patient population, including patients with/without diabetes mellitus and those with/without renal impairment. However, previous studies that investigated associations between maximum-IMT and coronary artery stenosis only included patients with diabetes mellitus without renal impairment.Citation11–Citation13 Therefore, the results of this study may be more helpful in the clinical setting.
There are several limitations in this study. First, this was a single-center, retrospective, observational study, which may have been subjected to patient selection bias. Second, all of the participants were Japanese patients from a single center, which might limit the possibility of generalizing our findings. Third, many of the patients’ baseline characteristics, including age and sex, were significantly different among the four groups. Fourth, manual measurement of IMT might have caused variation and affected the results of this study. Therefore, the possibility that these differences might affect study results cannot be excluded. Further prospective, multicenter, multiethnic studies are required to generalize our findings.
Conclusion
Renal impairment, diabetes mellitus, and increased maximum-IMT as measured by ultrasonography may be significant risk factors of coronary artery stenosis in outpatients. Maximum-IMT may also be a useful surrogate marker to predict the presence of coronary artery stenosis in patients with diabetes mellitus without renal impairment but not in other patients.
Acknowledgments
The authors would like to thank all medical staff of Chiba Prefectural Togane Hospital for their excellent medical care. We thank Ellen Knapp, PhD, from Edanz Group (www.edanzediting.com/ac) for editing a draft of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
- Sanchis-GomarFPerez-QuilisCLeischikRLuciaAEpidemiology of coronary heart disease and acute coronary syndromeAnn Transl Med201641325627500157
- HultenEACarbonaroSPetrilloSPMitchellJDVillinesTCPrognostic value of cardiac computed tomography angiography: a systematic review and meta-analysisJ Am Coll Cardiol201157101237124721145688
- JiangpingSZheZWeiWAssessment of coronary artery stenosis by coronary angiography: a head-to-head comparison with pathological coronary artery anatomyCirc Cardiovasc Interv20136326226823696600
- TavakolMAshrafSBrenerSJRisks and complications of coronary angiography: a comprehensive reviewGlob J Health Sci201241659322980117
- OllendorfDAKubaMPearsonSDThe diagnostic performance of multi-slice coronary computed tomographic angiography: a systematic reviewJ Gen Intern Med201126330731621063800
- SchroederSAchenbachSBengelFWorking Group Nuclear Cardiology and Cardiac CTEuropean Society of CardiologyEuropean Council of Nuclear CardiologyCardiac computed tomography: indications, applications, limitations, and training requirements: report of a Writing Group deployed by the Working Group Nuclear Cardiology and Cardiac CT of the European Society of Cardiology and the European Council of Nuclear CardiologyEur Heart J200829453155618084017
- LorenzMWMarkusHSBotsMLRosvallMSitzerMPrediction of clinical cardiovascular events with carotid intima-media thickness: a systematic review and meta-analysisCirculation2007115445946717242284
- LorenzMWPolakJFKavousiMCarotid intima-media thickness progression to predict cardiovascular events in the general population (the PROG-IMT collaborative project): a meta-analysis of individual participant dataLancet201237998312053206222541275
- PolakJFSzkloMO’LearyDHAssociations of coronary heart disease with common carotid artery near and far wall intima-media thickness: the multi-ethnic study of atherosclerosisJ Am Soc Echocardiogr20152891114112125944425
- PolakJFO’LearyDHEdge-detected common carotid artery intima-media thickness and incident coronary heart disease in the multi-ethnic study of atherosclerosisJ Am Heart Assoc201546e00149226077584
- IrieYSakamotoKKuboFAssociation of coronary artery stenosis with carotid atherosclerosis in asymptomatic type 2 diabetic patientsJ Atheroscler Thromb201118433734421224524
- IrieYKatakamiNKanetoHMaximum carotid intima-media thickness improves the prediction ability of coronary artery stenosis in type 2 diabetic patients without history of coronary artery diseaseAtherosclerosis2012221243844422321873
- FujiharaKSuzukiHSatoACarotid artery plaque and LDL-to-HDL cholesterol ratio predict atherosclerotic status in coronary arteries in asymptomatic patients with type 2 diabetes mellitusJ Atheroscler Thromb201320545246423363982
- MatsuoSImaiEHorioMRevised equations for estimated GFR from serum creatinine in JapanAm J Kidney Dis200953698299219339088
- KasamiRKanetoHKatakamiNRelationship between carotid intima-media thickness and the presence and extent of coronary stenosis in type 2 diabetic patients with carotid atherosclerosis but without history of coronary artery diseaseDiabetes Care201134246847021270201
- ChangHJChungNClinical perspective of coronary computed tomographic angiography in diagnosis of coronary artery diseaseCirc J201175224625221258164
- PignoliPTremoliEPoliAOrestePPaolettiRIntimal plus medial thickness of the arterial wall: a direct measurement with ultrasound imagingCirculation1986746139914063536154
- KawamoriRYamasakiYMatsushimaHPrevalence of carotid atherosclerosis in diabetic patients. Ultrasound high-resolution B-mode imaging on carotid arteriesDiabetes Care19921510129012941425091
- FujishimaMKiyoharaYKatoIDiabetes and cardiovascular disease in a prospective population survey in Japan: the Hisayama StudyDiabetes199645Suppl 3S14S16
- NakanoTNinomiyaTSumiyoshiSAssociation of kidney function with coronary atherosclerosis and calcification in autopsy samples from Japanese elders: the Hisayama studyAm J Kidney Dis2010551213019765871
- ChoIMinHSChunEJCoronary atherosclerosis detected by coronary CT angiography in asymptomatic subjects with early chronic kidney diseaseAtherosclerosis2010208240641119781704
- TonelliMMuntnerPLloydARisk of coronary events in people with chronic kidney disease compared with those with diabetes: a population-level cohort studyLancet2012380984480781422717317
- McCulloughPAAgrawalVDanielewiczEAbelaGSAccelerated atherosclerotic calcification and Monckeberg’s sclerosis: a continuum of advanced vascular pathology in chronic kidney diseaseClin J Am Soc Nephrol2008361585159818667741
- MakitaSAbikoANaganumaYNagaiMNakamuraMChronic kidney disease is associated with increased carotid artery stiffness without morphological changes in participants of health check-up programsAtherosclerosis2010213130631020832066
- ZhangLZhaoFYangYAssociation between carotid artery intima-media thickness and early-stage CKD in a Chinese populationAm J Kidney Dis200749678679217533021
- IshizakaYIshizakaNTaniMRelationship between albuminuria, low eGFR, and carotid atherosclerosis in Japanese womenKidney Blood Press Res200831316417018477851