
Abstract
Background
The aim of this study was to investigate the union time of acute middle-third scaphoid fractures following treatments and to analyze the effect of different factors on late union.
Patients and methods
We retrospectively reviewed patients with acute middle-third scaphoid fracture at our institution between January 2013 and December 2017. Patient demographics, fracture characteristics, and treatment strategy, such as age, gender, body mass index, habit of smoking, sides of injury, dominant hand, ulnar variance, multiple fractures, and treatment methods, were investigated. Univariate and multivariate analyses were used to identify possible predictive factors.
Results
A total of 132 patients with scaphoid fracture were included in our study. Operation was performed in 67 patients (50.8%), and conservative treatment was performed in the other 65 patients (49.2%). The union time was 7.2±0.5 weeks. In the multivariate logistic regression analysis, late diagnosis (odds ratio, 1.247; 95% CI, 1.022–1.521) and conservative treatment method (odds ratio, 1.615; 95% CI, 1.031–2.528) were identified as 2 independent predictors of late union in scaphoid fractures patients. Other parameters were not demonstrated to be predictive factors.
Conclusion
Late diagnosis and conservative treatment were two factors associated with late union. Long time of follow-up is necessary for patient with these factors.
Background
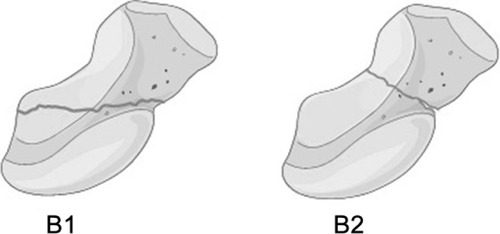
As the keystone for wrist stability by connecting the proximal row of carpal bones to the distal row, the scaphoid is the most commonly fractured carpal bone in active adolescents and young adults. It is estimated to account for up to 90% of carpal fractures and 2%–7% of all fractures,Citation1,Citation2 and the annual incidence is about 3.8–4.3 fractures per 10,000 people.Citation3,Citation4 Fractures are generally described as proximal-third, middle-third, or distal-third according to the site of fracture line. Among them, the middle-third is the most common site of fracture, accounting for ~75% of scaphoid fracture.Citation5 Classification of scaphoid fractures is essential for surgeons to guide treatment and to evaluate prognosis. According to the Herbert classification, acute middle-third fractures of the scaphoid can be classified into B1 (distal oblique fractures) and B2 (complete waist fractures) types.Citation6
Traditionally, nondisplaced and minimally displaced scaphoid fractures were considered to be stable, and cast immobilization was regarded as the first choice of treatment. Several studies have demonstrated satisfactory healing rates in association with conservative treatment for these fractures, ranging from 90% to 100%.Citation2,Citation7,Citation8 In recent years, as the patients’ expectations increase significantly, surgeons have been prone to choose early surgical treatment for these kinds of fractures. Due to the delicate vascular supply, injury to the scaphoid or its attachments may lead to severe long-term complications, such as bone nonunion and delay in union.Citation9,Citation10 Though risk factors for the development of nonunion have been well studied in previous literatures,Citation11,Citation12 little information is available regarding factors influencing time to healing.
We hypothesized that multiple factors might be associated with time to union of acute middle-third scaphoid fractures. The purpose of this study was to detect the union time of acute middle-third scaphoid fractures following conservative and surgical treatment and to analyze the effect of patient demographics, fracture characteristics, and treatment strategy on the union time.
Patients and methods
Patient population
All patients with an acute middle-third scaphoid fracture (within 4 weeks) who were referred to our hospital from January 2013 to December 2017 were considered for participation in this retrospective study. The inclusion criteria were adolescent (≥16 years old) and adult patients with type B1 or B2 scaphoid fractures according to the Herbert classification ().Citation6 Besides, only those with nondis-placed or minimally displaced fractures (<1 mm) as seen on plain radiographs were included. Patients with a history of previous scaphoid fractures and those with fractures that had occurred more than 4 weeks before treatment were excluded. The ethics committee of the Third Hospital of Hebei Medical University approved this research and waived the informed consent because this was a retrospective observational study, and all data were collected and analyzed anonymously.
Figure 1 The Herbert classification of middle-third fractures: B1 distal oblique fracture and B2 complete waist fracture.
Treatment strategy
Initially, patients underwent wrist radiographs to determine fracture site, presence of displacement, ulnar variance, and multiple fractures. Computed tomographic (CT) scans were performed to assess details of fractures if plain radiographs cannot show it. Magnetic resonance imaging (MRI) scans were also used to determine the presence of insidious fractures and occult injuries when other imaging modalities cannot determine. Patients received either nonoperative treatment with a cast or operative treatment with a Herbert screw.Citation6
The nonoperative treatment is mainly cast immobilization in a below-the-elbow cast with the thumb held in palmar abduction, the interphalangeal joint free, and the wrist in neutral or slight extension position. Hand therapy training was initiated when indicated. The cast was removed when fractures were considered completely united, based on the clinical findings, standard radiographs, and CT scans. After that, mobilization was encouraged.
The operative treatment for acute scaphoid fractures is performed by the volar approach. In brief, patients are placed in a supine position, and the wrist placed in extension and maximal ulnar deviation during surgical procedure. The prominence of the scaphoid tubercle is marked first, and then, a Kirschner wire is drilled about 45° ulnarly and 45° dorsally in relation to the neutral plain, entering the distal scaphoid, passing through the fracture plane, and entering the proximal scaphoid under a C-arm fluoroscope. The intraosseous position was checked in all planes before a self-drilling Herbert Cannulated Bone Screw (Zimmer, Warsaw, IN, USA) was introduced into the scaphoid. At last, the Kirschner wire was removed. Postoperative cast immobilization was not necessary for these patients.
Data collection and follow-up
The following patients’ demographics were collected, including age, gender, body mass index (BMI), habit of smoking, sides of injury, and dominant hand. Besides, the exact time between injury and making a definite diagnosis was also recorded. We defined it as late diagnosis if the time from injury to making a definite diagnosis was >5 days.
From wrist radiographs, the vertical distance was measured between the line drawn parallel to the proximal surface of lunate facet of radius and another line drawn parallel to articular surface of ulnar head. A distance >2 mm was considered as the presence of ulnar variance. Multiple fractures were defined as the presence of other fractures except for scaphoid fracture. Type B1 or B2 fractures were classified according to Herbert classification ().Citation6
Table 1 Classification of type B scaphoid fractures according to the Herbert classification
Patients were followed up routinely every 2 weeks after treatment. Fracture union was defined based on radiographic findings showing more than 50% bridging trabeculae on radiographs in more than 1 view of plain radiographs. The time from treatment to fracture union was recorded. A union time more than 8 weeks was considered as late union, otherwise, it was considered as early union. Final confirmatory CT scans were obtained to confirm complete healing, and follow-up was stopped.
Statistical analysis
Descriptive analysis of the variables was performed by use of mean and SD for continuous variables and frequencies and percentages for categorical variables. The difference between groups was determined by univariate analysis, which included Fisher’s exact tests and independent-samples t-tests. After univariate analysis, variables that might be potentially associated with union time of acute scaphoid fractures (P<0.20) were entered into the multiple logistic regression analysis and P-value <0.05 was considered as statistical significance. SPSS version 18.0 for Windows (SPSS Inc., Chicago, IL, USA) was used for data analyses.
Results
A total of 132 patients with scaphoid fracture were included in our study. There were 103 males (78.0%) and 29 females (22.0%). The age of these patients was 25.0±5.1 years. Advanced imaging before treatment was performed for 61 fractures (46.2%), with 55 fractures (90.2%) having at least 1 CT scan and 6 (9.8%) having at least 1 MRI scan. Operation was performed in 67 patients (50.8%), and conservative treatment was performed in the other 65 patients (49.2%).
There were 3 complications in the conservative group. Two of them were persistent wrist pain syndrome and resolved gradually after physical therapy. The other one was diagnosed as nonunion after 4 months of follow-up, and so the patient underwent internal fixation and bone grafting surgery. There were 4 complications in the operative group, which were a partial injury of the flexor carpi radialis tendon or trapezium bone during surgery. There were no infections or nonunion in operative group.
Patients were followed up for 11.3±2.1 weeks. The union time was 7.2±0.5 weeks. According to the criteria of fracture union, there were 89 patients in early union group and 43 patients in late union group. In the univariate analysis, there were 9 patients (10.1%) with late diagnosis in early union group and 11 patients (25.6%) in late union group. There was a statistically significant difference (P=0.036) between groups. Similarly, operation was performed in 52 patients (58.4%) in early union group and in 15 (34.9%) in late union group, and the difference is highly statistically significant (P=0.015). Furthermore, the difference in Herbert classification between groups is significant (P<0.20). However, there were no significant differences in age, gender, BMI, smoking, sides of injury, dominant hand, ulnar variance, and multiple fractures between early union and late union patients. The details of the result are listed in . In the multivariate logistic regression analysis, only late diagnosis (odds ratio [OR], 1.247; 95% CI, 1.022–1.521) and conservative treatment method (OR, 1.615; 95% CI, 1.031–2.528) were identified as independent predictors of late union in scaphoid fractures patients (). Other parameters were not demonstrated to be independent predictive factors.
Table 2 Comparison of variables between early union and late union patients with scaphoid fractures
Table 3 Multivariate logistic regression analysis of predictive factors associated with late union in acute scaphoid fractures
Discussion
In this study, we reviewed 132 patients with acute middle-third scaphoid fractures and found that both treatments can lead to satisfactory union rate. After the multivariate analysis, our main finding confirmed that late diagnosis and conservative treatment were 2 risk factors independently associated with late union. Therefore, long-term follow-up is necessary for patient with these factors.
Formerly, the first choice for nondisplaced and minimally displaced fractures was conservative treatment with long periods of cast immobilization. Despite the well-recognized problems of scaphoid nonunion after conservative treatment, it was demonstrated by previous studies that the majority of these fractures healed completely without complications.Citation2,Citation7,Citation8 In this study, we only included middle-third scaphoid fracture, which had better vascular supply than proximal-third fracture, and the results showed high rate of fracture union. However, conservative treatment with long-term immobilization is often associated with severe joint stiffness and decreased grip strength, as well as resulting in delays of patients’ return to work and resumption of normal daily activities.
An alternative surgical treatment was introduced by Filan and HerbertCitation6 with use of a new headless fixation screw. The double-threaded Herbert screw had differential pitch at the loading and trailing ends to provide rigid fixation, and thus, cast immobilization was rarely required. In their study, all acute fractures in their series had united by 12 months. Nevertheless, the true long-term benefits of internal fixation have not been adequately determined in recent randomized controlled trials or meta-analysis.Citation13–Citation15 In our current study, though we cannot determine a significant difference in the union rate, we did find relatively shorter union time in the operative group in comparison with the conservative group. This result was consistent with previous studies. For example, Bond et alCitation16 and McQueen et alCitation17 compared operative treatment with casting in mostly nondisplaced scaphoid fractures, and no significant difference in the union rate was found in either study, but both studies showed shorter union time and faster recovery in the operative group.
Meanwhile, our study found that late diagnosis might also lead to longer union time. Previous studies have demonstrated that delay in diagnosis is an important risk factor for the development of nonunion.Citation18,Citation19 There might be numerous reasons for the delayed diagnosis. Some patients might have felt that their symptoms did not warrant medical attention, but most patients encountered a missed diagnosis, because many nondisplaced scaphoid fractures presenting in the acute phase have normal initial radiographs. A previous study has revealed that 16% of scaphoid fractures may be radiographi-cally occult.Citation20 Stevenson et alCitation21 recommended early CT test to manage suspected occult scaphoid fractures for its accurate diagnosis, while Fallahi et alCitation22 considered that MRI scan should play a major role in the management of clinically suspected scaphoid fracture. For this reason, one should have a high level of suspicion when assessing young patients with radial wrist pain, and CT or MRI should be obtained to further assess for a nondisplaced scaphoid fracture.
B1 and B2 type fractures have a similar fracture line on the volar aspect of the scaphoid waist, but they show differences on the dorsal aspect of the scaphoid waist. In B1 fractures, the fracture line extends proximal to the scaphoid apex, but in B2 fractures, the fracture line extends distal to the scaphoid apex.Citation23 In comparison with B2 fractures, B1 type fractures are considered more stable, and interfragmentary motion is considerably lesser in B1 fractures.Citation24 In this series, B1 and B2 type fractures did not show significant difference in union time. However, we cannot make a definite conclusion yet because of the relatively small sample size, and further studies on basis of large population are still required to confirm this result.
The strength of this study is the absence of significant heterogenicity among patients. However, this study has several limitations. First of all, the retrospective design is the typical restriction of our study. Prospective studies are still required to confirm our results in future. Second, the results were concluded from patients with only acute middle-third scaphoid fractures, so the findings of our study need verification with different patient samples. Finally, we only analyzed a limited number of factors, and the inclusion of other factors may provide more valuable information to us.
Conclusion
In summary, though conservative treatment can lead to satisfactory union rate in patients with acute middle-third scaphoid fractures, it is associated with long union time. Besides, late diagnosis was also associated with late union. Long-term follow-up is necessary for patients with these factors.
Acknowledgments
We are grateful to Dr Bo Peng for his assistance in the statistical analysis.
Disclosure
The authors report no conflicts of interest in this work.
References
- PillaiAJainMManagement of clinical fractures of the scaphoid: results of an audit and literature reviewEur J Emerg Med2005122475115756078
- KozinSHIncidence, mechanism, and natural history of scaphoid fracturesHand Clin200117451552411775464
- HoveLMEpidemiology of scaphoid fractures in Bergen, NorwayScand J Plast Reconstr Surg Hand Surg199933442342610614752
- BrondumVLarsenCFSkovOFracture of the carpal scaphoid: frequency and distribution in a well-defined populationEur J Radiol19921521181221425745
- HaismanJMRohdeRSWeilandAJAmerican Academy of Orthopaedic SurgeonsAcute fractures of the scaphoidJ Bone Joint Surg Am200688122750275817219705
- FilanSLHerbertTJHerbert screw fixation of scaphoid fracturesJ Bone Joint Surg Br19967845195298682813
- BhatMMcCarthyMDavisTROniJADawsonSMRI and plain radiography in the assessment of displaced fractures of the waist of the carpal scaphoidJ Bone Joint Surg Br200486570571315274268
- GellmanHCaputoRJCarterVAboulafiaAMckayMComparison of short and long thumb-spica casts for non-displaced fractures of the carpal scaphoidJ Bone Joint Surg Am19897133543572925707
- JanowskiJCoadyCCatalanoLW3rdScaphoid fractures: nonunion and malunionJ Hand Surg Am201641111087109227671767
- CooneyWPLinscheidRLDobynsJHScaphoid fractures. Problems associated with nonunion and avascular necrosisOrthop Clin North Am19841523813916728452
- WongKvon SchroederHPDelays and poor management of scaphoid fractures: factors contributing to nonunionJ Hand Surg Am20113691471147421803508
- MandalesonAThamSKLewisCAcklandDCEkETScaphoid fracture fixation in a nonunion model: a biomechanical study comparing 3 types of fixationJ Hand Surg Am201843322122829132789
- ShenLTangJLuoCXieXAnZZhangCComparison of operative and non-operative treatment of acute undisplaced or minimally-displaced scaphoid fractures: a meta-analysis of randomized controlled trialsPLoS One2015105e125247
- Al-AjmiTAAl-FaryanKHAl-KanaanNFA systematic review and meta-analysis of randomized controlled trials comparing surgical versus conservative treatments for acute undisplaced or minimally-displaced scaphoid fracturesClin Orthop Surg2018101647329564049
- VinnarsBPietreanuMBodestedtAEkenstamFGerdinBNonoperative compared with operative treatment of acute scaphoid fractures. A randomized clinical trialJ Bone Joint Surg Am20089061176118518519309
- BondCDShinAYMcBrideMTDaoKDPercutaneous screw fixation or cast immobilization for nondisplaced scaphoid fracturesJ Bone Joint Surg Am200183-A448348811315775
- McQueenMMGelbkeMKWakefieldAWillEMGaeblerCPercutaneous screw fixation versus conservative treatment for fractures of the waist of the scaphoid: a prospective randomised studyJ Bone Joint Surg Br2008901667118160502
- LanghoffOAndersenJLConsequences of late immobilization of scaphoid fracturesJ Hand Surg Br198813177793361213
- KawamuraKChungKCTreatment of scaphoid fractures and non-unionsJ Hand Surg Am200833698899718656779
- HunterJCEscobedoEMWilsonAJHanelDPZink-BrodyGCMannFAMR imaging of clinically suspected scaphoid fracturesAJR Am J Roentgenol19971685128712939129428
- StevensonJDMorleyDSrivastavaSWillardCBhooraIGEarly CT for suspected occult scaphoid fracturesJ Hand Surg Eur Vol201237544745122086787
- FallahiFOliverRMandaliaSSJonkerLEarly MRI diagnostics for suspected scaphoid fractures subsequent to initial plain radiographyEur J Orthop Surg Traumatol20142471161116624292423
- MoritomoHRadiographic clues for determining carpal instability and treatment protocol for scaphoid fracturesJ Orthop Sci201419337938324535049
- LeventhalELWolfeSWMooreDCAkelmanEWeissAPCriscoJJInterfragmentary motion in patients with scaphoid nonunionJ Hand Surg Am20083371108111518762105