
Abstract
Background
Low back pain (LBP) is one of the most common spine diseases and represents the most frequent cause of absence from work in developed countries. Approximately 40% of chronic LBP is related to discogenic origin. The goal of the study is producing a review of literature to describe analytically the techniques of intradiscal injections.
Methods
PubMed database was searched for clinical studies with the different key terms: “intradiscal”, “injection”, “steroid” “procedures”, “techniques”, “CT”, “MRI”, “fluoroscopy”, “fluoroscopic”, “guidance”, “ozone”, “ultrasound”, “images”. Only studies written in English, French, or Italian in which the intradiscal injection represents the main procedure for the low back discopathy treatment on humans were considered. We excluded the articles that do not mention this procedure; those which indicated that the intradiscal injection had happened accidentally during other treatments; those reporting the patient’s pain was determined by other causes than the discopathy (facet joint syndrome, tumor, spondylodiscitis).
Results
Thirty-one articles dated from 1969 to 2018 met the criteria. The examined population was 6843 subjects, 52.3% male and 47.7% female, with a mean age of 45.9±10.1 years. The techniques are highly variable in terms of procedure: different operators, needle guidance, injection sites, drugs, tilt angle of the needle).
Conclusion
The efficacy and the safety of the intradiscal procedures are not easily comparable due to different types of studies and their limited number. Further studies are needed to standardize the intradiscal injection technique/procedure to improve safety, repeatability and effectiveness, and last but not least to reduce peri- and postoperative care and health-care costs.
Background
Low Back Pain (LBP) is one of the most common spine diseases and represents the most frequent reason of absence from work in developed countries. Around 80% of adults suffer from LBP during their lifetime, and 55% suffer from back pain associated with radicular syndrome.Citation1 Chronic LBP is often responsible for a low quality of life due to pain, for disability and loss of work productivity and, in addition, for high health-care costs for society.Citation2–Citation4 Regarding its etiology, in literature it has been reported that approximately 40% of chronic LBP has a discogenic origin.Citation5,Citation6 Currently in the advanced phases of discopathy and in high symptomatic subjects, the elective treatment still remains spinal surgery. In the other less complicated cases, the therapeutical steps could vary from a simple pharmacological therapy to a physical therapy, as the low back traction, over to spinal injection (epidural, periradicular, intradiscal and intra-articular procedures). Moreover, intervertebral disk decompression techniques are minimally invasive outpatient procedures for the treatment of disk herniation. Under imaging guidance and via a percutaneous approach, a needle is inserted in the nucleus pulposus of the herniated disk. A variety of decompressive device of thermic, chemical or mechanical nature are introduced inside the nucleus pulpous with minimal disruption of the surrounding tissues, assuring its partial removal and a significant decrease of intradiscal pressure. Thermal decompression is achieved using laser fiber, plasma, energy electrode, and radiofrequency coil/electrode. Chemical decompression is achieved by alcohol gel or ozone intradiscal injection, which causes dehydration and breakdown of the nucleus pulposus. Lately, there has been a trend for biomaterial implantation (hydrogel, platelet-rich plasma and stem cell therapy) aiming for intervertebral disk regeneration. Symptomatic intervertebral disk herniation (refractory to 4–6 weeks of a conservative therapy course), occupying less than one third of the spinal canal, as confirmed by MRI (magnetic resonance imaging), is an indication for percutaneous decompressive disk therapies. The mean success rate for all techniques is approximately 85%. The mean complication rate (infections like spondylodiscitis, allergic reaction, hemorrhage, neurologic injury) is <0.5%.Citation7 The goal of the study is producing a review of literature to describe analytically the actual techniques of intradiscal injections, the type of intervention performed, the used imaging guidance, the inoculated drug, the approach to the intervertebral disc, the patient’s position, the specialty of the operator performing the procedure, the type of anesthesia and the use of antibiotic prophylaxis.
Methods
Search Strategy
The PubMed database was searched for clinical studies with the following key terms: “intradiscal”, “injection”, “steroid” “procedures”, “techniques”, “CT” (computerized tomography), “MRI”, “fluoroscopy”, “fluoroscopic”, “guidance”, “ozone”, “ultrasound”, “images”. We made our research throw the combination of this terms, inserted between the Boolean operators “AND”/“OR”. We limited the research to studies on humans and types of articles were: case reports, clinical trials, controlled clinical trials, reviews, comparative studies, multicenter studies, and randomized controlled trials. The search was expanded through the bibliography within recruited texts ().
Inclusion and Exclusion Criteria
For our review, we only considered studies written in English, French, or Italian in which the intradiscal injection represents the main procedure for the low back discopathy treatment, both isolated and in combination. We excluded the articles that did not mention that procedure or those which indicated that the intradiscal injection had happened accidentally during other treatments (ie during transforaminal injection). We excluded the articles where the patient’s pain was due to other causes than the discopathy (facet joint syndrome, tumor, spondylodiscitis), and also those articles that described the treatment performed on an animal species. We checked the bibliography to make sure that the articles were compatible with our research.
Results
Initially using the term “intradiscal injection” as a search key on PubMed, we found 385 articles; the results were reduced when we added other search keys or other selection criteria, as we showed in the description of our strategy of research. Depending on the abstracts or full texts we excluded the studies that did not satisfy the inclusion criteria. Moreover, in this review we included other articles shown as bibliography in previous research. The final result consisted of 31 articlesCitation4,Citation8-Citation26,Citation35–Citation44 dated from 1969 to 2018, and the examined population was 6843 subjects (). We did not consider the number of patients treated in the Giurazza et al study38,Citation40 because being a review, it considered not only intradiscal, but also paravertebral injections. We also decided to cite other authors that described the varied and numerous procedures that are available to the image-guided interventions who may provide these therapies for the spine.Citation27–Citation31
Table 1 Clinical Characteristics of Trials Employment of Intradiscal Injection
Characteristics of Included Articles ()
The review includes three observational retrospective studies,Citation12,Citation18,Citation23 12 observational prospective studies,Citation13–Citation15,Citation19,Citation22,Citation26,Citation36-Citation38,Citation41,Citation43,Citation44 two multicenter pilot studies,Citation4,Citation10 two case–control studies,Citation11,Citation16 six randomized controlled trials,Citation4,Citation8,Citation17,Citation21,Citation24,Citation35,Citation42 one multicenter studyCitation25 two pilot studies,Citation20,Citation43 one case report,Citation9 one single arm phase I clinical trialCitation44 and one review.Citation40
Population
Our population is composed of 6843 subjects, 52.3% male and 47.7% female, with a mean age of 45.9±10.1 years.
End Points
The aim of the study was to review literature for scientific evidence of intradiscal injections, to describe analytically the actual techniques, the type of intervention performed, the used imaging guidance, the inoculated drug, the approach to the intervertebral disc, the patient’s position, the operator who performed the treatment, the type of anesthesia used, antibiotic prophylaxis, if used.
Treated Disease
In all selected articles,Citation4,Citation9-Citation26,Citation35–Citation38,Citation39–Citation44 the patients suffered from lumbar discopathy.
Type of Procedure
Different types of treatments are reported in the studies: intradiscal injection,Citation4,Citation8-Citation26,Citation35–Citation44 epiduralCitation19 intraforaminalCitation11,Citation21 and facet joint injection, selective nerve block (SNRB),Citation8 intradiscal high pressure injection (IDHP),Citation15 microendoscopic discectomy (MED).Citation16
Intradiscal Injection
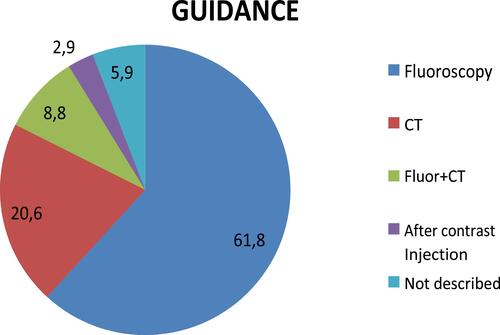
The technique of intradiscal injection is reported in 31 articles. In 24 studies,Citation4,Citation9,Citation10,Citation12,Citation14,Citation16,Citation17,Citation20,Citation22-Citation24,Citation26,Citation35–Citation44 it is the only treatment while, in the remaining seven studiesCitation11,Citation13,Citation15,Citation18,Citation19,Citation21,Citation25 it is compared to, or in association with, other minimally invasive procedures. (). In 19 articles the procedure was realized under fluoroscopy,Citation4,Citation10-Citation12,Citation14,Citation15,Citation20,Citation22,Citation24,Citation26,Citation35–Citation39,Citation41,Citation42,Citation44 in seven articles under CT guide,Citation13,Citation16–Citation18,Citation21,Citation23,Citation43 and in three studies both by fluoroscopy and CT guided, in comparisonCitation25 or in association;Citation19,Citation40 in two articles was not specifiedCitation9,Citation44 ().
Table 2 Characteristics of Intradiscal Injection Techniques
The patients of the de Seze et al trial,Citation13 Levi et alCitation46 and Giurazza et alCitation38 works were subjected to neurosedation, in the trials by Khot et alCitation23 and Oder et alCitation18 they were subjected to conscious sedation. In the studies by Fayad et alCitation19 and Andreula et alCitation24 and another five worksCitation34,Citation37–Citation39 the patients were neither sedated nor subjected to local anesthesia. In eleven trials,Citation10,Citation11,Citation13,Citation19,Citation21,Citation36,Citation37,Citation41–Citation44 all patients were subjected to local anesthesia. The antibiotic prophylaxis was used in eight trials.Citation4,Citation10,Citation19,Citation21,Citation41–Citation44 The interventions were performed by highly experienced operators in the Lehnert’s trialCitation12 two clinicians (two authors) in the Cao et al’s study;Citation16 Fayad et al,Citation19 Benyahya et al,Citation22 Noriega et al,Citation44 Giurazza et al,Citation38 and Nguyen et alCitation34 report the experienced radiologists, Gallucci et alCitation20 and Perri et alCitation40 neuroradiologists, Tuakli-Wosornu et alCitation39 and LeviCitation40,Citation46 physiatrist and Khot et alCitation23 two senior authors.
In 17 articles the required patients position was described according to the procedure: in 11 studies a prone position was used,Citation15,Citation18,Citation19,Citation21,Citation36,Citation38,Citation40–Citation44 Nguyen et alCitation34 and Sainoh et alCitation36 propose a lateral decubitus and Zhang et alCitation10 advised use of a pillow under the waist to get the widest intervertebral spaces.
For the procedure spinal needles of 18- (n=4), 20- (n=2), 21- (n=1), 22- (n=17) and 23- (n=1) gauge were used, with variable length to 7 from 17.8 cm. For example the Muto et al’s studyCitation17 mentioned a 22-gauge spinal needle with paravertebral oblique access, Lehnert et al’s studyCitation12 mentioned an extraspinal lateral approach with a 22-gauge 17.8-cm spinal needle and Gallucci et alCitation20 a paravertebral/interlaminar approach with a 9- or 15-cm 22-gauge spinal needle Five articlesCitation13,Citation14,Citation21,Citation22,Citation25 have specified that the side of the injection was chosen on the basis of the main location of symptoms.
The percutaneous approach is always posterior for the lumbar access: in 15.Citation10,Citation11,Citation14,Citation17,Citation20,Citation23,Citation24,Citation26,Citation35,Citation36,Citation38,Citation40–Citation44 out of 31 articles it was specified as a posterolateral access, in other studies it was extralaminarCitation12 or paravertebral access,Citation20 posterior-obliqueCitation14 paravertebral-oblique,Citation17 or anterolateral access. In the Gallucci et al’s studyCitation20 the intradiscal and intraforaminal injections were administered with a paravertebral approach in 92.4% of the patients and an interlaminar approach in 7.6% of the patients. The needle was advanced through the intraforaminal space, with an angle usually between 45° and 60°. In seven articles the point of access is not described.Citation4,Citation9,Citation12,Citation16,Citation22,Citation39,Citation44 Oder et al’s studyCitation18 specified that the percutaneous approach was about 45° along the lateral margin of the inferior articular process of the vertebra and through the neuroforamen for preserving the nerve root. Muto et alCitation17 used a needle inclination in a craniocaudal direction in the case of a lower herniation.
The site of injection is the center of the disc in 22 studies,Citation7,Citation10,Citation11,Citation13,Citation16-Citation22,Citation35–Citation44 the central third of the disc in the Yin et al’s studyCitation9 and in the mid portion of the herniated disc in the Fukui et al’s study.Citation14 The position of the needle was confirmed by fluoroscopy using anteroposterior and lateral views in 20 studies;Citation4,Citation8,Citation10–Citation12,Citation14,Citation15,Citation20,Citation22,Citation24,Citation25,Citation35–Citation39,Citation41,Citation42,Citation44 in Yin et al’s trialCitation9 the procedures were performed with real time multiplanar fluoroscopy, with CT scan in seven other articles,Citation13,Citation16–Citation18,Citation21,Citation23,Citation43 in three articles with both fluoroscopy and CT,Citation19,Citation25,Citation40 in two articles the position of the needle is not described.Citation9,Citation40
Some authors recommend the time remaining in supine position after injection: respectively 10 minutes;Citation10 one hour,Citation14 one, half an hour,Citation9 two hours,Citation4,Citation21,Citation25,Citation39 three hours,Citation13,Citation16 four hours,Citation41 six hours;Citation12 12 h,Citation18 12/24 h.Citation11,Citation37
Medicaments Injected
Several drugs have been injected, and were used individually or in association with each other: an oxygen-ozone mixture (O2O3) in eight studies,Citation10,Citation12,Citation17,Citation18,Citation20,Citation24,Citation38,Citation40 a saline solution in four studies;Citation14–Citation16,Citation23 in 13 articles the steroids have been administered (methylprednisolone, acetate of prednisolone, hydrocortisone, betamethasone),Citation8,Citation10,Citation11,Citation15,Citation16,Citation18–Citation20,Citation22–Citation25,Citation34 and in six trials the local anesthetic (bupivacaine, lidocaine) were injected.Citation4,Citation14,Citation20,Citation21,Citation24 For the remaining studies hypertonic dextrose,Citation21 fibrin sealant,Citation9 blue methylene,Citation4,Citation37 discogel,Citation13 autologous bone marrow concentrate,Citation35,Citation42 allogenic mesenchymal stem cell and hyaluronic acid,Citation41 tumour necrosis factor α1 inhibitorCitation36 and songmeileCitation16 (a kind of synthetic liquid of polypeptidic biological factors extracted from Chinese herbal medical ingredient) were used.
Outcomes Measures
Pain was the most frequently tested variable. It was expressed as percentage of patients with pain relief or as mean improvement on a continuous scale. The outcome measures shown in the studies were: VAS (visual analog score), NRS (numeric rating scale), McGill Pain Questionnaire. Outcome assessment of patient satisfaction are reported by “modified MacNab scale” or using Odom criteria (“Excellent”, “Good”, “Satisfactory” and “Poor”). Back-specific disability is expressed on a back-specific index, such as the Roland Disability Questionnaire or the Oswestry Disability Index and JOA score (widely used in Japan to evaluate disabilities associated with low-back pain and includes the following items: subjective symptoms; clinical signs; restriction of activities of daily living. JOA score ranges from 29 as the most positive score to minus six for the worst a global measure of improvement). Quality of life is measured by the SF-12, SF-36, and EuroQol.
Patients Global Impression of Change (PGIC) measured by a seven-point Likert scale. The evaluations of general health status or well being, disability for work, and patient satisfaction have all so been reported.
The disc volume was evaluated by MRI and CT images.
Clinical and/or radiologic short term follow-up were mainly performed at four or six weeks; the long-term follow-up were performed from 12, 24, 48, weeks up to 4–10 years.
Efficacy
The efficacy of the treatment is the target in 30 articles,Citation4,Citation9–Citation25,Citation34–Citation44 The results are reported as clearly satisfactory in 27 out of the 30 articles,Citation4,Citation9–Citation20,Citation22,Citation24,Citation34–Citation44 In the Muto et al’s study, for example, the results on 2900 patients, treated for LBP with intradiscal injection of O2–O3, were evaluated with the modified MacNab classification, the VAS and the Oswestry Disability Index at six and 12 months. Success rates were 75–80% for soft disc herniation, 70% for multiple-disc herniations and 55% for failed back surgery syndrome. None of the patients suffered early or late neurological or infectious complications.Citation17 Benyahya et al22 made a retrospective study of medical records of 85 patients (55 women, mean age 49±9 years) to assess the effectiveness of intradiscal injection of acetate of prednisolone for the treatment of LBP. They used the global appreciation of the patient (excellent, good, mild, none, worse) concerning the result of the intradiscal injection, at one, three and six months. For effectiveness of intradiscal injection, the results showed that 71.8% of the patients considered the result good or excellent at one month, 55.3% at three months and 43.5% at six months.
Adverse Events
Six trials have reported the side effects,Citation9,Citation12,Citation22,Citation24,Citation26,Citation34 overall 32 cases for 6843 patients (0.47% of patients): three cases of discitis, two after injection of corticosteroid,Citation25 one after injection of fibrin sealant;Citation9 26 patients present impairment of sensitivity in the lower limb ipsilateral to the treatment with injection oxygen-ozone;Citation12,Citation24 two discs showed a collapse after injection of corticosteroid,Citation22 1 case of increase in sciatica pain in the 24 hafter the intervention.Citation34
Two trials were performed under CT guidance;Citation12,Citation22 two studies were performed by fluoroscopy,Citation9,Citation25 and only one case by both fluoroscopy and CT guide.Citation24 Adverse events occurred in about 0.7% of the patients with CT guided injection and in 0.2% of the patients with fluoroscopic guided injection. In Yin et al’s trials,Citation9 the patients have even been subjected to antibiotic prophylaxis, in others articles this was not described.
Yin et al, Lehnert et al, Benyahya et al, Andreula et al and Feffer et alCitation9,Citation12,Citation22,Citation24,Citation25 report a posterolateral/extraspinal-lateral approach. Giurazza et al report that
The overall procedural complications rate is estimated around 0.1%. Have been reported in the literature: paresthesia on the anterolateral portion of the left leg and foot, suggesting nerve injury; few temporary episodes of impaired bilateral sensitivity; vitreoretinal hemorrhages; thunderclap headache related to pneumoencephalus as a consequence of inadvertent intrathecal puncture; and 1 case of vertebrobasilar stroke.Citation38
Discussion
For the low back pain management, patients with a small or contained herniated disc with no response to medical treatments, can be candidates for one of the minimally invasive percutaneous techniques. Generally, the minimally invasive techniques offer good results with patient compliance and low cost, showing a very low side effects percentage.Citation20 Only 0.47% of patients have manifested adverse events after intradiscal injection. The procedure is carried out on an outpatient basis by highly experienced operators such as radiologists,Citation19,Citation22 neuroradiologists,Citation20 physiatristsCitation46,Citation39 and orthopedics.Citation23 The procedure is of interest for many medical areas, for this reason standardizing this method allows it to be extended to various practitioners.
For preoperative management there is no consensus regarding sedation, local anesthesia, or antibiotic prophylaxis. Only seven authors mention antibiotic use,Citation4,Citation9,Citation20,Citation46–Citation41 only two articles describe conscious sedationCitation18,Citation23 and three describe a deep sedation.Citation13,Citation38,Citation46 Some unreviewed medical articlesCitation28,Citation29 do not recommend local or general anesthesia because they could mask the nerve root puncture symptoms; the needle passes very close to the nerve root and may often touch it, causing a strong electric shock sensation which is quite harmless; if the patient is conscious they will feel the pain. About 0.19% of the patients subjected to antibiotic prophylaxis have had adverse events; while without antibiotics about 0.09% of the population have had side effects; current data do not allow a statistical analysis; for this reason prospective clinical trials are needed. Some authors advise setting up an aseptic room for anesthesiology care, ensuring peripheral access to the patient.Citation29
A concordance has emerged about the patient position, the injection site and the needle type. The most included articlesCitation14,Citation17,Citation20,Citation26,Citation28–Citation30,Citation35,Citation37-Citation44 report a prone position as the best to increase the intervertebral space, also using a support under the abdomen to reduce lumbar lordosis. The lateral decubitus was reported in two worksCitation34,Citation36 and in an unreviewed journal on chemiodiscolysis with ozone.Citation28 According to five of the articles,Citation12,Citation13,Citation20,Citation21,Citation24 de Santis et alCitation29 recommend an access side at the same side as the symptoms.
The chosen injection site is the center of the disc, and the injection point was checked by fluoroscopic projections,Citation4,Citation9–Citation11,Citation13,Citation14,Citation19,Citation21,Citation23,Citation25,Citation34–Citation39,Citation41,Citation43 CT scans;Citation12,Citation15–Citation18,Citation20,Citation23,Citation24,Citation38,Citation40 we highlight the need for trials to evaluate the more effective, safe, and less expensive methods, especially if using a toxic or very expensive drugs. For the safety, the data do not clarify which is the least injurious method, even though we have recorded a greater percentage of adverse events with the CT guided injection (). Clinical trials with same medication comparing the fluoroscopy and CT guided injections are needed.
During the procedure, the needle can be readily shifted a few millimeters to pass through without damaging the nerve. The approach and the needle inclination are essential criteria for a successful and safe procedure. In some articles it appears that the lumbar approach has a lateral inclination of 45° to 60° with respect to the axial lineCitation18,Citation20 and that for the lower discs an additional cranial-caudal inclination is needed.Citation20 We did not find accurate descriptions on the needle insertion procedure because the needle course was always evaluated radiographically and the access site was chosen accordingly. The authors recommend and/or use a fluoroscopy performed with the C-arm, that allows identification the trajectory of optimal access for needle placement into each disc.Citation10,Citation29,Citation30 An image-guided procedure handbookCitation30 describes a window of anatomical access to the intradiscal injection delineated by the superior articular process medially, the superior endplate below, and the traversing nerve root laterally and above. Staying close to the superior articular process could keep the needle as far as possible from the traversing nerve root.
The postintervention management was different between treatments, the authors have advised several rest times depending on the procedure ().
The efficacy and the safety of the intradiscal procedures are not easily comparable because the techniques are highly variable in terms of procedure (different operators, needle guidance, injection sites, drugs, tilt angle of the needle) ().
Conclusions
The efficacy and the safety of the intradiscal procedures are not easily comparable because of differences in the design of studies and their limited number.
The intradiscal injection is a technique widely used in the LBP management of patients with no response to rehabilitative and medical treatments. Differences of agreement between researchers are present on the technical aspects of the procedure in terms of imaging guidance, of injected substances, and efficacy of evaluation tools.
Further studies are needed in order to standardize the intradiscal injection technique/procedure as well as to improve efficacy, safety, repeatability, and to assess cost-effectiveness.
Figure 1 Flow diagram illustrating published literature on intradiscal injection.
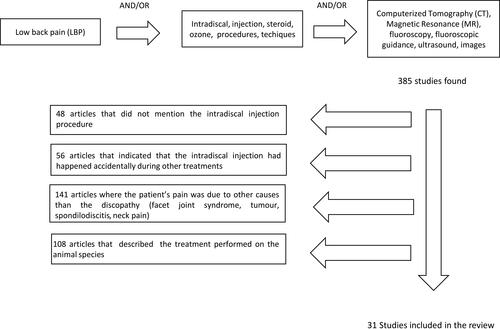
Figure 2 Different type of image guidance for intradiscal injection.
Abbreviations
ADC, apparent diffusion coefficient; AL-MSC, allogenic mesenchymal stem cells; AT-BMC, autologous bone marrow concentrate; AT-MSC, adipose tissue mesenchymal stem cells; BM, blue methilene; C, control group; Cs, corticosteroid; CT, computerized tomography; EG, experimental group; EL, extraspinal lateral; Ep, epidural; EQ-5D, EuroQol; Fluor, fluoscopy; AL, anterolateral; FRI, Functional Rating Index; FS, fibrin sealant; HA, hyaluronic acid; HyD, hypertonic dextrose; ID, intradiscal injection; LA, local anesthetic; LBP, low back pain; MGPQ, McGill Pain Questionnaire; MIDPD, measurement of the intervertebral disc posterior dimension; MRI, magnetic resonance imaging; MSC, mesecnchymal stem cells; NASS, the modified North American Spine Society; NRS, Numeric Rating Scale; ODI, Oswestry Disability Index; P, periganglionic injection; PL, posterolateral; PO, posterior-oblique; Post, posterior; PR, periradicular injection; PRP, platelet-rich plasma; Pv/IL, paravertebral/interlaminar; PvO, paravertebral-Oblique; RCT, randomized controlled trial; RMDQ, Roland–Morris Disability Questionnaire; SANE, modified single assessment numeric evaluation; SF-36, short form-36; SNRB, selective nerve block; TF, transforaminal; TNF-α I, tumor nerosis factor α inhibitor; Treatm, treatment; VAS, visual analog scale.
Data Sharing Statement
All data analyzed during this study are included in this article.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
Additional information
Funding
References
- Guarnieri G, Vassallo P, Pezzullo MG, et al. A comparison of minimally invasive techniques in percutaneous treatment of lumbar herniated discs. Neuroradiol J. 2009;22(1):108–121. doi:10.1177/197140090902200116
- Becker A, Held H, Redaelli M, et al. Implementation of a guideline for lowback pain management in primary care: a cost effectiveness analysis. Spine. 2012;37:701–710. doi:10.1097/BRS.0b013e31822b01bd
- Leadley RM, Armstrong N, Lee YC, Allen A, Kleijnen J. Chronic diseases in the European Union: the prevalence and health cost implications of chronic pain. J Pain Palliat Care Pharmacother. 2012;26:310–325. doi:10.3109/15360288.2012.736933
- Kallewaard JW, Geurts JW, Kessels A, Willems P, van Santbrink H, van Kleef M. Efficacy, safety, and predictors of intradiscal methylene blue injection for discogenic low back pain: results of a multicenter prospective clinical series. Pain Pract. 2015. doi:10.1111/papr.12283
- Kuslich SD, Ulstrom CL, Michael CJ. The tissue origin of low back pain and sciatica: a report of pain response to tissue stimulation during operations on the lumbar spine using local anesthesia. Orthop Clin North Am. 1991;22:181–187.
- Schwarzer AC, Aprill CN, Derby R, Fortin J, Kine G, Bogduk N. The relative contributions of the disc and zygapophyseal joint in chronic lowback pain. Spine. 1994;19:801–806. doi:10.1097/00007632-199404000-00013
- Santiago FR, Kelekis A, Alvarez LG, Filippiadis DK. Interventional procedures of the spine. Semin Musculoskelet Radiol. 2014;18(3):309–317. doi:10.1055/s-0034-1375572
- Mineta K, Higashino K, Sakai T, Fukui Y, Sairyo K. Recurrence of type I modic inflammatory changes in the lumbar spine: effectiveness of intradiscal therapy. Skeletal Radiol. 2014;43(11):1645–1649. doi:10.1007/s00256-014-1947-x
- Yin W, Pauza K, Olan WJ, Doerzbacher JF, Thorne KJ. Intradiscal injection of fibrin sealant for the treatment of symptomatic lumbar internal disc disruption: results of a prospective multicenter pilot study with 24-month follow-up. Pain Med. 2014;15:16–31. Wiley Periodicals, Inc.
- Zhang Y, Ma Y, Jiang J, Ding T, Wang J. Treatment of the lumbar disc herniation with intradiscal and intraforaminal injection of oxygen-ozone. J Back Musculoskelet Rehabil. 2013;26(3):317–322. doi:10.3233/BMR-130386
- Beaudreuil J, Dieude P, Poiraudeau S, Revel M. Disabling chronic low back pain with modic type 1 MRI signal: acutereduction in pain with intradiscal corticotherapy. Ann Phys Rehabil Med. 2012;55:139–147. doi:10.1016/j.rehab.2012.01.004
- Lehnert T, Naguib NN, Wutzler S, et al. Analysis of disk volume before and after CT-guided intradiscal and periganglionic ozone-oxygen injection for the treatment of lumbar disk herniation. J Vasc Interv Radiol. 2012;23(11):1430–1436. doi:10.1016/j.jvir.2012.07.029
- De Seze M, Saliba L, Mazaux J-M. Percutaneous treatment of sciatica caused by a herniated disc: an exploratory study on the use of gaseous discography and discogel1 in 79 patients. Ann Phys Rehabil Med. 2013;56:143–154. doi:10.1016/j.rehab.2013.01.006
- Fukui SMD PhD, Iwashita NMD, Nitta K MD, Tomie HMD, Nosaka SMD PhD. The results of percutaneous intradiscal high-pressure injection of saline in patients with extruded lumbar herniated disc: comparison with microendoscopic discectomy. Pain Med.2012;13:762–768. doi:10.1111/j.1526-4637.2012.01400.x
- Yu Y, Liu W, Song D, Guo Q, Jia L. Diagnosis of discogenic low back pain in patients with probable symptoms but negative discography. Arch Orthop Trauma Surg. 2012;132(5):627–632. doi:10.1007/s00402-011-1448-5
- Cao P, Jiang L, Zhuang C, et al. Intradiscal injection therapy for degenerative chronic discogenic low back pain with endplate modic changes. Spine J. 2011;11(2):100–106. doi:10.1016/j.spinee.2010.07.001
- Muto M, Ambrosanio G, Guarnieri G, et al. Low back pain and sciatica: treatment with intradiscal-intraforaminal O(2)-O(3) injection. Our experience. Radiol Med. 2008;113(5):695–706. doi:10.1007/s11547-008-0302-5
- Oder B, Loewe M, Reisegger M, Lang W, Ilias W, Thurnher SA. CT-guided/steroid therapy for the treatment of degenerative spinal disease–effect of age, gender, disc pathology and multi-segmental changes. Neuroradiology. 2008;50(9):777–785. doi:10.1007/s00234-008-0398-2
- Fayad F, Lefevre-Colau MM, Rannou F, et al. Relation of inflammatory modic changes to intradiscal steroid injection outcome in chronic low back pain. Eur Spine J. 2007;16(7):925–931. doi:10.1007/s00586-006-0301-y
- Gallucci M, Limbucci N, Zugaro L, et al. Sciatica: treatment with intradiscal and intraforaminal injections of steroid and oxygen-ozone versus steroid only. Radiology. 2007;242(3):907–913. doi:10.1148/radiol.2423051934
- Miller Matthew RDSc, PA-C, Mathews RSMD, PhD, Dean RKMD. Treatment of painful advanced internal lumbar disc derangement with intradiscal injection of hypertonic dextrose. Pain Physician. 2006;9:115–121.
- Benyahya R, Lefevre-Colau MM, Fayad F, et al. Intradiscal injection of acetate of prednisolone in severe low back pain: complications and patients assessment of effectiveness. Ann Readapt Med Phys. 2004;47:621–626. doi:10.1016/S0168-6054(04)00193-X
- Khot A, Bowditch M, Powell J, Sharp D. The use of intradiscal steroid therapy for lumbar spinal discogenic pain: a randomized controlled trial. Spine. 2004;29:833–836. doi:10.1097/00007632-200404150-00002
- Andreula CF, Simonetti L, De Santis F, et al. Minimally invasive oxygenozone therapy for lumbar disk herniation. AJNR Am J Neuroradiol. 2003;24:996–1000.
- Feffer HL. Therapeutic intradiscal hydrocortisone. A long-term study. Clin Orthop Relat Res. 1969;67:100–104. doi:10.1097/00003086-196911000-00015
- Andreula C, Muto M, Leonardi M. Interventional spinal procedures. Eur J Radiol. 2004;50:112–119. doi:10.1016/j.ejrad.2003.10.013
- Muto M, Andreula C, Leonardi M. Treatment of herniated lumbar disc by intradiscal and intraforaminal oxygen-ozone (O2-O3) injection. J Neuroradiol. 2004;31(3):183–189. doi:10.1016/S0150-9861(04)96989-1
- Leonardi M. La puntura discale sotto fluoroscopia. Riv Ital Ossigeno Ozonoterapia. 2002;1:73–78.
- De Santis F, Leonardi M, Simonetti L, Dall’Olio M, Princiotta C, Menetti F. Ossigeno-Ozonoterapia: la tecnica intradiscale. Int J Ozone Ther. 2009;8:138–146.
- Mathis. Image-Guided spine Interventions. New York: Springer; 2004.
- Migliore T, Laganà P, Granata B, et al. Safety of intra-articular hip injection of hyaluronic acid products by ultrasound guidance: an open study from ANTIAGE register. Eur Rev Med Pharmacol Sci. 2013;17(13):1752–1759.
- Migliore A, Bizzi E, Massafra U, et al. A new technical contribution for ultrasound-guided injections of sacro-iliac joints. Eur Rev Med Pharmacol Sci. 2010;14(5):465–469.
- Jee H, Lee JH, Park K 3, Ahn J, Park Y. Ultrasound-guided versus fluoroscopy-guided sacroiliac joint intra-articular injections in the noninflammatory sacroiliac joint dysfunction: a prospective, randomized, single-blinded study. Arch Phys Med Rehabil. 2014;95(2):330–337. doi:10.1016/j.apmr.2013.09.021
- Nguyen C, Boutron I, Baron G, et al. Intradiscal glucocorticoid injection for patients with chronic low back pain associated with active dicopathy. Ann Intern Med. 2017. doi:10.7326/M16.1700
- Pettine A, Suzuki RK, Sand TT, Murphy MB. Autologous bone marrow concentrate intradiscal injection for the treatment of degenerative disc disease with three-year follow up. Int Orthop. 2017;41:2097. doi:10.1007/s00264-017-3560-9
- Sainoh T, Orita S, Miyagi M, et al. Single intradiscal administration of the tumor necrosis factor-alpha inhibitor, etanercept, for patients with discogenic low back pain. Pain Med. 2016;17:40–45. doi:10.1111/pme.12892
- Zhang XJ, Hao J, Hu ZM, Yang HT. Clinical evaluation and magnetic resonance imaging assessment of intradiscal methylene blue injection for the treatment of discogenic low back pain. Pain Physician. 2016;19:E1189–E1195.
- Giurazza F, Guarnieri G, Murphy KJ, Muto M. Intradiscal O2O3: rationale, injection technique, short- and long-term outcomes for the treatment of low back pain due to disc herniation. Can Assoc Radiol J. 2017;68:171–177. doi:10.1016/j.carj.2016.12.007
- Tuakli-Wosornu YA, Terry A, Boachie-Adjei K, et al. Lumbar intradiskal Platelet-Rich Plasma (PRP) injections: a prospective, double-blind, Randomized Controlled Study. Pmrjournal. 2016;8:1–10.
- Perri M, Marsecano C, Varrassi M, et al. Indications and efficacy of O2–O3 intradiscal versus steroid intraforaminal injection in different types of disco vertebral pathologies: a prospective randomized double‑blind trial with 517 patients. Radiol Med. 2016;121:463–471. doi:10.1007/s11547-015-0598-x
- Kumar H, Ha DH, Lee EJ, et al. Safety and tolerability of intradiscal implantation of combined autologous adipose-derived mesenchymal stem cells and hyaluronic acid in patients with chronic discogenic low back pain: 1-year follow-up of a phase I study. Stem Cell Res Ther. 2017;8:262. doi:10.1186/s13287-017-0710-3
- Pettine K, Suzuki R, Sand T, Murphy M. Treatment of discogenic back pain with autologous bone marrow concentrate injection with minimum two year follow-up. Int Orthop. 2015. doi:10.1007/s00264-015-2886-4
- Centeno C, Markle J, Dodson E, et al. Treatment of lumbar degenerative disc disease‑associated radicular pain with culture‑expanded autologous mesenchymal stem cells: a pilot study on safety and efficacy. J Transl Med. 2017;15:197. doi:10.1186/s12967-017-1300-y
- Noriega DC, Ardura F, Hernández-Ramajo R, et al. Intervertebral disc repair by allogeneic mesenchymal bone marrow cells: a randomized controlled trial. Transplantation. 2017;101(8):1945–1951. doi:10.1097/TP.0000000000001484
- Hartung W, Ross CJ, Straub R, et al. Ultrasound-guided sacroiliac joint injection in patients with established sacroiliitis: precise IA injection verified by MRI scanning does not predict clinical outcome. Rheumatology (Oxford). 2010;49(8):1479–1482. doi:10.1093/rheumatology/kep424
- Levi D, Horn S, Tyszko S, Levin J, Hecht-Leavitt C, Walko E. Intradiscal platelet-rich plasma injection for chronic discogenic low back pain: preliminary results from a prospective trial. Pain Med. 2016;17:1010–1022. doi:10.1093/pm/pnv053