
Abstract
Introduction
Obstructive sleep apnea (OSA) is a public health problem that affects children. Although continuous positive airway pressure (CPAP) therapy is effective, the CPAP adherence rate in children is varied. This study aimed to evaluate the CPAP adherence rate and factors associated with CPAP adherence in children with OSA using a systematic review.
Methods
The inclusion criteria were observational studies conducted in children with OSA and assessed adherence of CPAP using objective evaluation. The literature search was performed in four databases. Meta-analysis using fixed-effect model was conducted to combine results among included studies.
Results
In all, 34 studies that evaluated adherence rate and predictors of CPAP adherence in children with OSA were included, representing 21,737 patients with an average adherence rate of 46.56%. There were 11 calculations of factors predictive of CPAP adherence: age, sex, ethnicity, body mass index, obesity, income, sleep efficiency, the apnea-hypopnea index (AHI), severity of OSA, residual AHI, and lowest oxygen saturation level. Three different factors were linked to children with adherence and non-adherence to CPAP: age, body mass index, and AHI.
Conclusion
The CPAP adherence rate in children with OSA was 46.56%. Young age, low body mass index, and high AHI were associated with acceptable CPAP adherence in children with OSA.
Keywords:
Introduction
Obstructive sleep apnea (OSA) is a public health problem in children. A review reported a prevalence rate of pediatric OSA that varied among countries with a range of 0.1% (Singapore) to 13.0% (Italy).Citation1 A report from China found that the prevalence of OSA may be as high as 63.9% of 1578 children between 2 and 15 years of age with snoring.Citation2 OSA is reported to be more common in children with certain conditions such as obesity, allergic rhinitis, or Down syndrome.Citation3–6 The prevalence of OSA among children with obesity was 4.9 times higher than among non-obese children (44.6% vs 9.1%; p = 0.0002).Citation6 If left untreated, OSA in children increases their risks for neurocognitive dysfunction, abnormal behavior, and cardiovascular diseases such as hypertension or left ventricular hypertrophy.Citation7,Citation8
Continuous positive airway pressure (CPAP) is recommended for children with OSA if adenotonsillectomy is not performed or OSA is unresolved after this surgery.Citation9 A prospective study among children with OSA found that CPAP provided immediate and sustained improvement of OSA over a one-year period.Citation10 Scores on the Epworth Sleepiness Scale improved significantly at one year from baseline (14.44 to 7.86; p = 0.001).Citation10 However, information regarding the cardiovascular impact of OSA in children is lacking and evidence of CPAP benefits is quite limited.
A known problem with CPAP therapy is adherence. A previous systematic review of 46 included studies found that the average adherence rate from 20 studies (1079 participants) was 56.9% (range of 24–87%). Note that, for this systematic review, the average age of participants was 9.4 years with a range of 0.5–16 years; 34 studies had participants with developmental delays. Several factors were found to be associated with poorer CPAP adherence, including age (five studies), sex (two studies), race (one study), body mass index (BMI) (one study), and developmental delay (two studies).Citation11 However, this systematic review was reported as a scoping review without summarized calculation according to meta-analysis style.
Another meta-analysis on this topic published in 2020 with the final search in 2019 identified five factors calculated as predictors of CPAP adherence in children with OSA.Citation12 Studies conducted on non-invasive ventilator or a randomized controlled trial were included, resulting in an ability to report the CPAP adherence rate for children with OSA.Citation13,Citation14 Additionally, the adherence rate was not reported. As the previous meta-analysis did not report the CPAP adherence rate with a gap of three years and limited predictors, this study aimed to evaluate the adherence rate and add more calculations regarding predictors of CPAP adherence in children with OSA by updating the search.
Methods
This was an update to a meta-analysis study to evaluate factors predictive of adequate CPAP adherence in children with OSA. The study was registered at PROSPERO (ID: CRD42022346132).
Eligibility Criteria
Population
This study included studies conducted among children with OSA. It evaluated CPAP adherence using objective evaluation regardless of types of CPAP device, CPAP company, adherence criteria, inclusion criteria, or other factors such as age, sex, or co-morbid diseases. The CPAP devices used to treat OSA in children were standard CPAP, automatic CPAP (APAP), or bilevel positive airway pressure (BPAP). The details regarding each device have been reported elsewhere.Citation15
Intervention and Control Group
This study did not evaluate any type of intervention to assist CPAP use in children with OSA. We mainly evaluated personal and laboratory factors associated with CPAP adherence in children with OSA who experienced CPAP therapy. Those who adhered to CPAP therapy (studied group) were compared with those who did not (control group). The diagnosis of OSA is based on polysomnography with an apnea-hypopnea index (AHI) of 1/hour or higher.Citation2 During polysomnography, the lowest oxygen saturation level while asleep was reported as a percentage, and sleep efficiency percentage was reported defined as the total sleep time divided by the total time in bed during polysomnography. After treatment with CPAP, adherence data were downloaded either from the device or cloud technology.
Outcomes
The outcomes of the study were overall CPAP adherence rate and factors predictive of adequate CPAP adherence in children with OSA.
Study Types
The study types included in this study were any observational studies. Those studies with intervention, stimulation, no adherence data, non-CPAP or non-BPAP, non-objective data on adherence were excluded as were case reports/case series, commentaries, books, abstracts, and reviews.
Search Strategy
Four databases were used for systematic searching including PubMed, Central database, Scopus, and CINAHL Plus. Hand-searching for related studies was also conducted. Search terms included OSA, adherence, CPAP, and bilevel positive airway pressure (BPAP/BiPAP). The full list of search terms is shown in the Appendix. The final search was conducted on August 31, 2022.
Selection Process
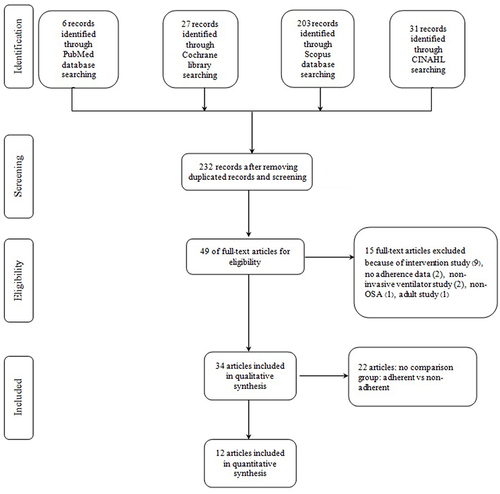
After the removal of duplicates, initial screening was conducted for non-relevant articles. Only pediatric studies were eligible and were included if factors predictive of adequate CPAP adherence were evaluated. The initial screening process was performed independently by two authors (BS, KS). Studies selected by each reviewer were compared and entered in the full-text review process. Data extraction and full-text reviews were performed independently by two authors (BS, KS) using a priori form. Any disagreements between the authors were reviewed and decided by a third reviewer (CN). A Prima flowchart of article searching and included studies is illustrated in .
Figure 1 A Prima flowchart for adherence rate and predictors adherence of a positive airway pressure machine (CPAP) in pediatric patients with obstructive sleep apnea.
Data Collection
Data collection for each included study was retrieved for the following: publication characteristics, study characteristics, outcome characteristics, and predictor characteristics. The publication characteristics comprised the first author, year of publication, and country of study origin, while study characteristics comprised the study aim and design; age, sex, comorbidities (if any), and AHI; and duration of CPAP use. The outcome characteristics included method of assessment of CPAP adherence, definition of adherence, numbers of total cases, numbers of cases in adherence group, and numbers of cases in non-adherence group. For predictor characteristics, numbers and percentages of each potential predictor in the adherence and non-adherence groups were tabulated.
Data Analysis
There were two groups in this study: an adherence and a non-adherence group. Differences between both groups were computed for CPAP adherence. Mean differences with 95% confidence interval (CI) of numerical factors between both groups were calculated, while odds ratio with 95% CI of categorical factors between both groups were executed. I2 statistic was used to measure heterogeneity among the results of included studies. Substantial heterogeneity was identified when I2 was greater than 75%. Fixed-effect model was used to perform meta-analysis when I2 was less than 75%. Random-effects model was used to combine the results of included studies when substantial heterogeneity was found. A forest plot of each factor was created to show differences between both groups. All analyses were performed by Review Manager 5.4 (RevMan).
Risk of Bias
Study quality of observational studies including retrospective, prospective, and cross-sectional studies was evaluated using the Newcastle-Ottawa Scale (NOS), which was adapted for cross-sectional studies and applied to evaluate study quality.Citation16 Details of the scale have been described elsewhere.Citation16,Citation17 Study quality is categorized as very good, good, satisfactory, and unsatisfactory. Risk of bias was performed by two authors independently (BS, CN). A disagreement between authors was reviewed and decided by a third reviewer (KS).
Results
There were 232 studies related to adherence to CPAP in patients with OSA after duplicate studies were removed (). Of these, 50 were eligible for a full-text review and 16 of them were excluded because they were intervention studies (nine), had no objective adherence assessment (two), were based on non-invasive ventilation (two), were non-OSA (one), had no objective adherence data (one), or were conducted with adults (one). Thus, 34 studies remained that evaluated adherence in children with OSA; these were published from 2011 to 2022 ().Citation18–51 Of these 34, 12 studies had compared those who were adherent with those who were not and had applied a meta-analysis calculation ( and ).Citation40–51 Most of the 34 studies were conducted in North America (23 of 34 studies) and had a retrospective study design (20 of 34 studies). The longest duration for CPAP adherence evaluation was four yearsCitation22 with an average duration of 10.04 (SD 9.82) months.
Table 1 Characteristics of Pediatric Studies with Obstructive Sleep Apnea (OSA) on Compliance of a Continuous Positive Airway Pressure Machine (CPAP): Included Studies but Not in a Meta-Analysis
Table 2 Characteristics and Outcomes of Pediatric Studies with Obstructive Sleep Apnea (OSA) on Compliance of a Continuous Positive Airway Pressure Machine (CPAP): Included Studies but Not in a Meta-Analysis
Table 3 Characteristics of Pediatric Studies with Obstructive Sleep Apnea (OSA) on Compliance of a Continuous Positive Airway Pressure Machine (CPAP): Included Studies for a Meta-Analysis
Table 4 Characteristics and Outcomes of Pediatric Studies with Obstructive Sleep Apnea (OSA) on Compliance of a Continuous Positive Airway Pressure Machine (CPAP): Included Studies for a Meta-Analysis
The adherence rate was assessed using data downloaded from CPAP devices either online or from the device in most studies, while CPAP adherence was defined by case notes, clinical data, parent report, or durable medical equipment (DME) providers as shown in and .Citation24,Citation42,Citation43,Citation46 The adherence criteria differed slightly among studies but was mostly defined as usage of four hours or more per night for 50–70% of nights. For the included studies without meta-analysis calculation ( and ), the adherence rate was 46.53% (9,883/21,240) from 13 studies based on usage of four hours or more per night (). The adherence rate for included studies for meta-analysis was 47.69% (237/497). In total, the adherence rate in children with OSA was 46.56% (10,120/21,737). The average CPAP usage in four studies () ranged from 2.8 to 7.0 hours/night. Note that three studies compared clinical factors per specific group: developmental disabilities,Citation25 family members with CPAP therapy,Citation32 and age group.Citation18 Additionally, one study compared those with CPAP adherence to intermittent users, who were categorized as non-adherent.Citation47
There were 11 calculations of factors predictive of CPAP adherence: age, sex, ethnicity, BMI, obesity, income, sleep efficiency, AHI, severity of OSA, residual AHI, and lowest oxygen saturation level (). Three factors in regard to children who were adherent and those who were non-adherent with CPAP use were identified as age (), BMI (), and AHI (). Children with OSA with effective adherence to CPAP use were younger and had lower BMIs than those with non-adherence. The mean differences (95% CI) of these two factors were −1.42 years (−2.07, −0.77) and −6.55 kg/m2 (−11.80, −1.30), respectively, as shown in and . Children with OSA with satisfactory adherence to CPAP had significantly higher AHIs than those who were non-adherent, with a mean difference of 4.75 events/hour (95% CI of 1.07, 8.43 events/hour) as shown in . Regarding the quality of the included studies (), most had a score of satisfactory (8/10; 80%). Two studies were not evaluated due to non-cross-sectional study design.
Table 5 Study Quality Evaluation by the Newcastle-Ottawa Scale Adapted for Cross-Sectional Studies of the Included Studies of Pediatric Studies with Obstructive Sleep Apnea on Compliance of a Continuous Positive Airway Pressure Machine: Included Studies for a Meta-Analysis
Figure 2 Calculation of age (years) of pediatric patients with obstructive sleep apnea on adherence of a continuous positive airway pressure machine.Citation40–43,Citation45,Citation48,Citation49,Citation51
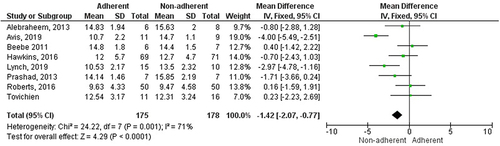
Figure 3 Calculation of sex of pediatric patients with obstructive sleep apnea on adherence of a continuous positive airway pressure machine.Citation40–49,Citation51
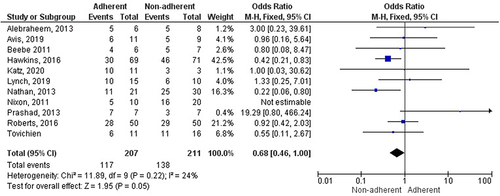
Figure 4 Calculation of ethnicity (Caucasian) of pediatric patients with obstructive sleep apnea on adherence of a continuous positive airway pressure machine.Citation41–43,Citation45
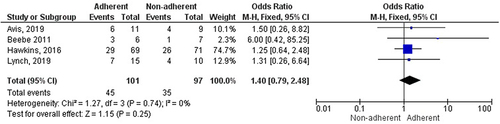
Figure 5 Calculation of body mass index (kg/m2) of pediatric patients with obstructive sleep apnea on adherence of a continuous positive airway pressure machine.Citation40–42,Citation45,Citation49
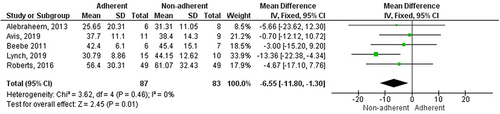
Figure 6 Calculation of obesity of pediatric patients with obstructive sleep apnea on adherence of a continuous positive airway pressure machine.Citation40,Citation46,Citation48,Citation51
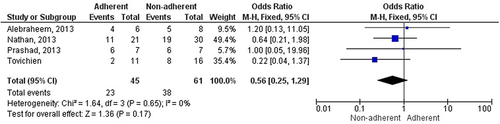
Figure 7 Calculation of income of family less than 20,000 USD of pediatric patients with obstructive sleep apnea on adherence of a continuous positive airway pressure machine.Citation41,Citation45
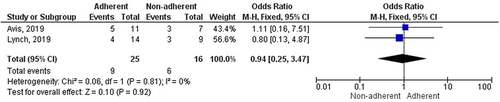
Figure 8 Calculation of sleep efficiency (%) during polysomnography of pediatric patients with obstructive sleep apnea on adherence of a continuous positive airway pressure machine.Citation41,Citation49

Figure 9 Calculation of apnea-hypopnea index (events/hour) of pediatric patients with obstructive sleep apnea on adherence of a continuous positive airway pressure machine.Citation40,Citation42,Citation43,Citation45,Citation48–50
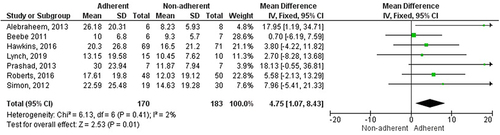
Figure 10 Calculation of severe obstructive sleep apnea (OSA) of pediatric patients with OSA on adherence of a continuous positive airway pressure machine.Citation43,Citation45,Citation46
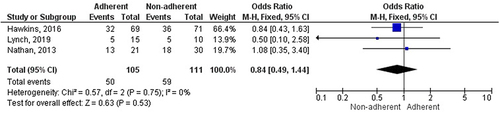
Figure 11 Calculation of residual apnea-hypopnea index (events/hour) of pediatric patients with obstructive sleep apnea on adherence of a continuous positive airway pressure machine.Citation40,Citation43

Figure 12 Calculation of lowest oxygen level (%) during polysomnography of pediatric patients with obstructive sleep apnea on adherence of a continuous positive airway pressure machine.Citation43,Citation48,Citation49

Discussion
This meta-analysis showed that the adherence rate in children with OSA was 46.56% with CPAP usage of four hours or more based on 21,737 children with OSA. Age, BMI, and AHI were related to adequate CPAP adherence.
Compared with the previous meta-analysis, we summarized the adherence rate based on a large study population. Meta-analysis calculations were added for 11 factors, and we added 11 articles published after 2019 that were not included in the previous systematic review.Citation12 After including more studies in the present meta-analysis, we found significant results in regard to age, BMI, and AHI on CPAP adherence in children with OSA (, and ) and nearly significant results regarding sex with a 95% CI of 0.46, 1.00 (). The previous meta-analysis was unable to declare significance in regard to age (not performed), BMI (difference −0.14; 95% CI: −0.47, 0.19), or AHI (difference 4.32; 95% CI: −0.61, 9.26).Citation12 As previously noted, these three factors were significant predictors of CPAP adherence in this study. These differences between the two meta-analysis studies may be due to more studies included in the present analysis. However, we did not perform an analysis on CPAP vs BPAP, as in the previous meta-analysis, as we were unable to find appropriate data for calculation in the two studies.Citation26,Citation35 In our study, one study reported significant adherence between CPAP vs BPAP with an unadjusted odds ratio of 3.60 (2.39–5.10).Citation46 However, this was not significant after being adjusted for other factors. Additionally, we were unable to analyze the developmental delay factor as data were not sufficient for the calculation. Only the study by Kang et al reported findings in regard to developmental delay, while the Hawkins study had incomplete data on this factor, resulting in the inability to calculate as a meta-analysis.Citation25,Citation43 Finally, this present study included only published articles, unlike the previous report, which included abstract articles.Citation12
As previously reported, children with OSA who were younger were adherent with CPAP. The adherent group was −1.85 years younger than the non-adherent group. The younger patients may have had caregivers, usually their mother, who facilitated their CPAP treatment. By contrast, older children may have more barriers to wearing the CPAP device during sleep. A study conducted with adolescent patients with an average age of 13.2 years found that older children may have several barriers to CPAP use because they are away from home more often (47%); they may simply want to forget about having OSA (43.1%); they may not feel well (42.0%); or they may forget to use the device (39.2%).Citation50 In addition, a lack of help from a parent or other caregiver to use CPAP at night represented another barrier in 31.4%.Citation50
Similar to age, BMI was negatively correlated with CPAP adherence (). In other words, those with lower BMI had better CPAP adherence than those with higher BMI. As shown in , the significance of BMI was driven by the study by Lynch et al.Citation45 A previous report found that high BMI was related to mask leakage (r = 0.579; p < 0.001) resulting in poor CPAP adherence.Citation52 Obese children may have a higher risk for mask leakage, leading to poor adherence as high mask leakage was correlated with poor adherence (r = −0.376; p = 0.008).Citation52
Regarding polysomnographic factors, only AHI was related to CPAP adherence in children with OSA. Previous studies in adult patients with OSA found that lowest oxygen saturation differed significantly between the adherence group and the non-adherence group (80.33% vs 85.18%; p value = 0.017) as well as duration of oxygen saturation lower than 90% (10.0% vs 5.0%; p = 0.013).Citation53,Citation54 Four studies showed that AHI was related to CPAP adherence in adult patients.Citation53–56 Adult patients with oxygen desaturation index (ODI), an index comparable to AHI, of over 60 times/hour had a CPAP adherence rate of 90.8% at 10 years. The ODI or AHI also had an adjusted hazard ratio for CPAP adherence of 0.97 (p < 0.001). As previously reported,Citation57 severity of OSA may be associated with more sleepiness, leading to better adherence to CPAP but not other polysomnographic factors such as oxygen level or sleep efficiency ( and ).
Above, we have discussed why AHI was associated with CPAP adherence in adults. In children, our analysis found that six of seven studies in the meta-analysis calculation had non-significant higher AHI in the adherent group than the non-adherent group; the study by Alebraheem et al was the exception (). Additionally, another study identified non-significant higher AHI in the adherent group as well (20.5 vs 17.5 events/h; p 0.651).Citation51 Note that the study by Tovichien et al was not included as they reported median AHI. After totaling up, the adherent group had greater significant value than the non-adherent group. Unlike in adults, further studies may be required to explain why AHI is significantly related to CPAP adherence. One study found that less severe OSA was related to low adherence to CPAP with a relative risk of 0.97.Citation19
This study also added data about the adherence rate in children with OSA in a large sample (n = 22,075), which was not reported in the previous meta-analysis. The adherence rate was almost 50% but may be higher in specific populations, eg, 90% in children with developmental delays,Citation25,Citation43 87% in children with obesity or craniofacial anomalies,Citation28 or in those using BPAP (91–100%).Citation27,Citation46 This adherence rate was slightly lower than that previously reported at 56.9%.Citation11 These differences may be due to sample size numbers and included studies. The previous study had 1,079 participants from 20 studies, while this study had 22,075 participants from 34 studies.Citation11 Several studies conducted with adults found that CPAP adherence rate ranged from 34% to 83%.Citation58–62 Similar to children with OSA, there are several predictors of good adherence, such as age, sex, education level, and AHI.Citation61–65
This study has several limitations. First, there are no standard criteria for CPAP adherence in children with OSA, resulting in different adherence criteria (). Second, some factors are not analyzed as they do not meet the calculation criteria for meta-analysis and data are not available for some populations, for example, Black children or children with asthma.Citation18 Finally, interventions to facilitate CPAP adherence or OSA consequences or related conditions such as quality of life or cardiovascular diseases were not studied.Citation66–72
Conclusions
Young age, low BMI, and high AHI are associated with satisfactory CPAP adherence in children with OSA. Although these factors were significant, the overall quality of evidence was fair, and the duration of study was generally about six months with no interventions. Further studies with longer durations or interventions should be considered. However, these factors may be helpful for clinicians in order to initiate CPAP therapy in potential patients for satisfactory adherence. Additionally, further interventions may be important for these groups of patients to facilitate CPAP adherence. Based on the large sample size, the CPAP adherence rate for children with OSA was 46.56%.
Patient and Public Involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Additional information
Funding
References
- Lumeng JC, Chervin RD. Epidemiology of pediatric obstructive sleep apnea. Proc Am Thorac Soc. 2008;5:242–252. doi:10.1513/pats.200708-135MG
- Xu Z, Wu Y, Tai J, et al. Risk factors of obstructive sleep apnea syndrome in children. J Otolaryngol Head Neck Surg. 2020;49:11. doi:10.1186/s40463-020-0404-1
- Simpson R, Oyekan AA, Ehsan Z, et al. Obstructive sleep apnea in patients with Down syndrome: current perspectives. Nat Sci Sleep. 2018;10:287–293. doi:10.2147/NSS.S154723
- Trivedi M, ElMallah M, Bailey E, et al. Pediatric Obstructive Sleep Apnea and Asthma: clinical Implications. Pediatr Ann. 2017;46(9):e332–e335. doi:10.3928/19382359-20170815-03
- Cao Y, Wu S, Zhang L, et al. Association of allergic rhinitis with obstructive sleep apnea: a meta-analysis. Medicine. 2018;97(51):e13783. doi:10.1097/MD.0000000000013783
- Andersen IG, Homøe P. Obstructive sleep apnea in children and adolescents with and without obesity. Eur Arch Otorhinolaryngol. 2019;276:871–878. doi:10.1007/s00405-019-05290-2
- Krysta K, Bratek A, Zawada K, et al. Cognitive deficits in adults with obstructive sleep apnea compared to children and adolescents. J Neural Transm. 2017;124:187–201. doi:10.1007/s00702-015-1501-6
- Cuspidi C, Tadic M, Gherbesi E, et al. Targeting subclinical organ damage in obstructive sleep apnea: a narrative review. J Hum Hypertens. 2021;35(1):26–36. doi:10.1038/s41371-020-00397-0
- Marcus CL, Brooks LJ, Draper KA, et al. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2012;130:576–584. doi:10.1542/peds.2012-1671
- Sudarsan SS, Paramasivan VK, Arumugam SV, et al. Comparison of treatment modalities in syndromic children with obstructive sleep apnea--A randomized cohort study. Int J Pediatr Otorhinolaryngol. 2014;78(9):1526–1533. doi:10.1016/j.ijporl.2014.06.027
- Watach AJ, Xanthopoulos MS, Afolabi-Brown O, et al. Positive airway pressure adherence in pediatric obstructive sleep apnea: a systematic scoping review. Sleep Med Rev. 2020;51:101273. doi:10.1016/j.smrv.2020.101273
- Blinder H, Momoli F, Bokhaut J, et al. Predictors of adherence to positive airway pressure therapy in children: a systematic review and meta-analysis. Sleep Med. 2020;69:19–33. doi:10.1016/j.sleep.2019.12.015
- Ennis J, Rohde K, Chaput J-P, et al. Facilitators and Barriers to Noninvasive Ventilation Adherence in Youth with Nocturnal Hypoventilation Secondary to Obesity or Neuromuscular Disease. J Clin Sleep Med. 2015;11(12):1409–1416. doi:10.5664/jcsm.5276
- Marcus CL, Rosen G, Ward SLD, et al. Adherence to and effectiveness of positive airway pressure therapy in children with obstructive sleep apnea. Pediatrics. 2006;117:e442–451. doi:10.1542/peds.2005-1634
- Killick R, Marshall NS. The impact of device modifications and pressure delivery on adherence. Sleep Med Clin. 2021;16:75–84. doi:10.1016/j.jsmc.2020.10.008
- Sisay M, Mengistu G, Edessa D. Epidemiology of self-medication in Ethiopia: a systematic review and meta-analysis of observational studies. BMC Pharmacol Toxicol. 2018;19:56. doi:10.1186/s40360-018-0248-8
- Namwaing P, Ngamjarus C, Sakaew W, et al. Chest physical therapy and outcomes in primary spontaneous pneumothorax: a systematic review. J Med Assoc Thailand. 2021;104:S165–S168.
- Bhattacharjee R, Benjafield AV, Armitstead J, et al. Adherence in children using positive airway pressure therapy: a big-data analysis. Lancet Digit Health. 2020;2:e94–e101. doi:10.1016/S2589-7500(19)30214-6
- Blinder H, Momoli F, Holland SH, et al. Clinical predictors of nonadherence to positive airway pressure therapy in children: a retrospective cohort study. J Clin Sleep Med. 2021;17(6):1183–1192. doi:10.5664/jcsm.9162
- Cielo CM, Hernandez P, Ciampaglia AM, et al. Positive airway pressure for the treatment of OSA in infants. Chest. 2021;159(2):810–817. doi:10.1016/j.chest.2020.08.020
- Castorena-Maldonado A, Torre-Bouscoulet L, Meza-Vargas S, et al. Preoperative continuous positive airway pressure compliance in children with obstructive sleep apnea syndrome: assessed by a simplified approach. Int J Pediatr Otorhinolaryngol. 2008;72(12):1795–1800. doi:10.1016/j.ijporl.2008.08.016
- Com G, Carroll JL, Tang X, et al. Characteristics and surgical and clinical outcomes of severely obese children with obstructive sleep apnea. J Clin Sleep Med. 2015;11(04):467–474. doi:10.5664/jcsm.4608
- DiFeo N, Meltzer LJ, Beck SE, et al. Predictors of positive airway pressure therapy adherence in children: a prospective study. J Clin Sleep Med. 2012;8(03):279–286. doi:10.5664/jcsm.1914
- Elder D, Gandhi S, Campbell A. CPAP for paediatric patients in Aotearoa New Zealand: audit of a developing service at Capital and Coast DHB 2005-2020. N Z Med J. 2022;135:62–71.
- Kang EK, Xanthopoulos MS, Kim JY, et al. Adherence to positive airway pressure for the treatment of obstructive sleep apnea in children with developmental disabilities. J Clin Sleep Med. 2019;15:915–921. doi:10.5664/jcsm.7850
- Katz SL, MacLean JE, Hoey L, et al. Insulin resistance and hypertension in obese youth with sleep-disordered breathing treated with positive airway pressure: a prospective multicenter study. J Clin Sleep Med. 2017;13:1039–1047. doi:10.5664/jcsm.6718
- Machaalani R, Evans CA, Waters KA. Objective adherence to positive airway pressure therapy in an Australian paediatric cohort. Sleep Breath. 2016;20:1327–1336. doi:10.1007/s11325-016-1400-6
- Marcus CL, Ward SL, Mallory GB, et al. Use of nasal continuous positive airway pressure as treatment of childhood obstructive sleep apnea. J Pediatr. 1995;127:88–94. doi:10.1016/S0022-3476(95)70262-8
- Mulholland A, Mihai R, Ellis K, et al. Paediatric CPAP in the digital age. Sleep Med. 2021;84:352–355. doi:10.1016/j.sleep.2021.06.006
- O’Donnell AR, Bjornson CL, Bohn SG, et al. Compliance rates in children using noninvasive continuous positive airway pressure. Sleep. 2006;29:651–658.
- Perriol M-P, Jullian-Desayes I, Joyeux-Faure M, et al. Long-term adherence to ambulatory initiated continuous positive airway pressure in non-syndromic OSA children. Sleep Breath. 2019;23:575–578. doi:10.1007/s11325-018-01775-2
- Puri P, Ross KR, Mehra R, et al. Pediatric positive airway pressure adherence in obstructive sleep apnea enhanced by family member positive airway pressure usage. J Clin Sleep Med. 2016;12:959–963. doi:10.5664/jcsm.5924
- Ramirez A, Khirani S, Aloui S, et al. Continuous positive airway pressure and noninvasive ventilation adherence in children. Sleep Med. 2013;14:1290–1294. doi:10.1016/j.sleep.2013.06.020
- Trucco F, Chatwin M, Semple T, et al. Sleep disordered breathing and ventilatory support in children with Down syndrome. Pediatr Pulmonol. 2018;53(10):1414–1421. doi:10.1002/ppul.24122
- Uong EC, Epperson M, Bathon SA, et al. Adherence to nasal positive airway pressure therapy among school-aged children and adolescents with obstructive sleep apnea syndrome. Pediatrics. 2007;120:e1203–1211. doi:10.1542/peds.2006-2731
- van den Broek N, Broer L, Vandenbussche N, et al. Obstructive sleep apnea in people with intellectual disabilities: adherence to and effect of CPAP. Sleep Breath. 2021;25:1257–1265. doi:10.1007/s11325-020-02221-y
- Weiss MR, Allen ML, Landeo-Gutierrez JS, et al. Defining the patterns of PAP adherence in pediatric obstructive sleep apnea: a clustering analysis using real-world data. J Clin Sleep Med. 2021;17:1005–1013. doi:10.5664/jcsm.9100
- Willis LD, Spray BJ, Scribner A, et al. Outcomes of pediatric titration sleep studies following empirical use of positive airway pressure and the effect on adherence to therapy. Respir Care. 2022;67(4):464–470. doi:10.4187/respcare.09521
- Xanthopoulos MS, Kim JY, Blechner M, et al. Self-efficacy and short-term adherence to continuous positive airway pressure treatment in children. Sleep. 2017. doi:10.1093/sleep/zsx096
- Alebraheem Z, Toulany A, Baker A, et al. Facilitators and barriers to positive airway pressure adherence for adolescents. A qualitative study. Ann Am Thorac Soc. 2018;15(1):83–88. doi:10.1513/AnnalsATS.201706-472OC
- Avis KT, Gamble KL, Schwebel DC. Effect of positive airway pressure therapy in children with obstructive sleep apnea syndrome: does positive airway pressure use reduce pedestrian injury risk? Sleep Health. 2019;5:161–165. doi:10.1016/j.sleh.2018.12.006
- Beebe DW, Byars KC. Adolescents with obstructive sleep apnea adhere poorly to positive airway pressure (PAP), but PAP users show improved attention and school performance. PLoS One. 2011;6:e16924. doi:10.1371/journal.pone.0016924
- Hawkins SMM, Jensen EL, Simon SL, et al. Correlates of pediatric CPAP adherence. J Clin Sleep Med. 2016;12:879–884. doi:10.5664/jcsm.5892
- Katz SL, Kirk VG, MacLean JE, et al. Factors related to positive airway pressure therapy adherence in children with obesity and sleep-disordered breathing. J Clin Sleep Med. 2020;16:733–741. doi:10.5664/jcsm.8336
- Lynch MK, Elliott LC, Avis KT, et al. Quality of life in youth with Obstructive Sleep Apnea Syndrome (OSAS) treated with Continuous Positive Airway Pressure (CPAP) Therapy. Behav Sleep Med. 2019;17:238–245. doi:10.1080/15402002.2017.1326918
- Nathan AM, Tang JPL, Goh A, et al. Compliance with noninvasive home ventilation in children with obstructive sleep apnoea. Singapore Med J. 2013;54(12):678–682. doi:10.11622/smedj.2013241
- Nixon GM, Mihai R, Verginis N, et al. Patterns of continuous positive airway pressure adherence during the first 3 months of treatment in children. J Pediatr. 2011;159(5):802–807. doi:10.1016/j.jpeds.2011.04.013
- Prashad PS, Marcus CL, Maggs J, et al. Investigating reasons for CPAP adherence in adolescents: a qualitative approach. J Clin Sleep Med. 2013;9:1303–1313. doi:10.5664/jcsm.3276
- Roberts SD, Kapadia H, Greenlee G, et al. Midfacial and dental changes associated with nasal positive airway pressure in children with obstructive sleep apnea and craniofacial conditions. J Clin Sleep Med. 2016;12(04):469–475. doi:10.5664/jcsm.5668
- Simon SL, Duncan CL, Janicke DM, et al. Barriers to treatment of paediatric obstructive sleep apnoea: development of the adherence barriers to continuous positive airway pressure (CPAP) questionnaire. Sleep Med. 2012;13(2):172–177. doi:10.1016/j.sleep.2011.10.026
- Tovichien P, Kulbun A, Udomittipong K. Comparing adherence of Continuous and Automatic Positive Airway Pressure (CPAP and APAP) in Obstructive Sleep Apnea (OSA) children. Front Pediatr. 2022;10:841705. doi:10.3389/fped.2022.841705
- Sopkova Z, Dorkova Z, Tkacova R. Predictors of compliance with continuous positive airway pressure treatment in patients with obstructive sleep apnea and metabolic syndrome. Wien Klin Wochenschr. 2009;121:398–404. doi:10.1007/s00508-009-1181-z
- Riachy M, Najem S, Iskandar M, et al. Factors predicting CPAP adherence in obstructive sleep apnea syndrome. Sleep Breath. 2017;21(2):295–302. doi:10.1007/s11325-016-1408-y
- Campos-Rodriguez F, Martinez-Alonso M, Sanchez-de-la-Torre M, et al. Long-term adherence to continuous positive airway pressure therapy in non-sleepy sleep apnea patients. Sleep Med. 2016;17:1–6. doi:10.1016/j.sleep.2015.07.038
- Kohler M, Smith D, Tippett V, et al. Predictors of long-term compliance with continuous positive airway pressure. Thorax. 2010;65:829–832. doi:10.1136/thx.2010.135848
- Baratta F, Pastori D, Bucci T, et al. Long-term prediction of adherence to continuous positive air pressure therapy for the treatment of moderate/severe obstructive sleep apnea syndrome. Sleep Med. 2018;43:66–70. doi:10.1016/j.sleep.2017.09.032
- McArdle N, Devereux G, Heidarnejad H, et al. Long-term use of CPAP therapy for sleep apnea/hypopnea syndrome. Am J Respir Crit Care Med. 1999;159:1108–1114. doi:10.1164/ajrccm.159.4.9807111
- Weaver TE, Grunstein RR. Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc. 2008;5:173–178. doi:10.1513/pats.200708-119MG
- Sarrell EM, Chomsky O, Shechter D. Treatment compliance with continuous positive airway pressure device among adults with obstructive sleep apnea (OSA): how many adhere to treatment?. Harefuah. 2013;152:140–144, 184, 183.
- Campos-Rodriguez F, Martinez-Alonso M, Sanchez-de-la-Torre M, et al. Long-term adherence to continuous positive airway pressure therapy in non-sleepy sleep apnea patients. Sleep Med. 2016;17:1–6.
- Kaewkes C, Sawanyawisuth K, Sawunyavisuth B. Are symptoms of obstructive sleep apnoea related to good continuous positive airway pressure compliance? ERJ Open Res. 2020;6:1–4. doi:10.1183/23120541.00169-2019
- Sawunyavisuth B. What personal experiences of CPAP use affect CPAP adherence and duration of CPAP use in OSA patients? J Med Assoc Thailand. 2018;101:S245–S249.
- Campos-Rodriguez F, Martinez-Garcia MA, Reyes-Nuñez N, et al. Long-term continuous positive airway pressure compliance in females with obstructive sleep apnoea. Eur Respir J. 2013;42:1255–1262. doi:10.1183/09031936.00165812
- Russo-Magno P, O’Brien A, Panciera T, et al. Compliance with CPAP therapy in older men with obstructive sleep apnea. J Am Geriatr Soc. 2001;49(9):1205–1211. doi:10.1046/j.1532-5415.2001.49238.x
- Şahin E, Cengiz C, Dağıstan H, et al. Factors affecting CPAP compliance in patients with obstructive sleep apnea. J Surg Med. 2021;5:340–343. doi:10.28982/josam.897532
- Sawunyavisuth B. What are predictors for a continuous positive airway pressure machine purchasing in obstructive sleep apnea patients? Asia Pacific J Sci Technol. 2018;23:5.
- Boonwang T, Namwaing P, Srisaphonphusitti L, et al. Esports may improve cognitive skills in soccer players: a systematic review. Asia Pacific J Sci Technol. 2022;27:64.
- Sawunyavisuth B, Ngamjarus C, Sawanyawisuth K. Any effective intervention to improve CPAP adherence in children with obstructive sleep apnea: a systematic review. Glob Pediatr Health. 2021;8:2333794X211019884. doi:10.1177/2333794X211019884
- Sanlung T, Sawanyawisuth K, Silaruks S, et al. Clinical characteristics and complications of obstructive sleep apnea in srinagarind hospital. J Med Assoc Thailand. 2020;103:36–39.
- Sawunyavisuth B, Ngamjarus C, Sawanyawisuth K. A meta-analysis to identify factors associated with CPAP machine purchasing in patients with obstructive sleep apnea. Biomed Rep. 2022;16:45. doi:10.3892/br.2022.1528
- Manasirisuk P, Chainirun N, Tiamkao S, et al. Efficacy of generic atorvastatin in a real-world setting. Clin Pharmacol. 2021;13:45–51. doi:10.2147/CPAA.S285750
- Soontornrungsun B, Khamsai S, Sawunyavisuth B, et al. Obstructive sleep apnea in patients with diabetes less than 40 years of age. Diabetes Metab Syndrome. 2020;14:1859–1863. doi:10.1016/j.dsx.2020.09.008