
Abstract
Background
Sore throat is a common complication after general anesthesia. Oral care solutions have been used to reduce the incidence of oral complications or ventilator-associated pneumonia, but their effect on postoperative sore throat (POST) is unclear. This study aims to investigate whether oral care solution can alleviate POST in patients undergoing i-gel laryngeal mask general anesthesia.
Methods
A total of 120 patients who were scheduled for elective surgery under laryngeal mask general anesthesia were enrolled. The patients were randomly assigned to an experimental group (oral care solution) and a control group (0.9% saline) and gargled for 1 min with 10mL of oral care solution or saline 5 min before anesthesia induction. The primary outcomes were the overall incidence of sore throat within 24 h and incidence at 20 min, 1 h, 6 h, 24 h after removal of i-gel. The secondary outcomes were the severity of sore throat at the four time points and incidence of hoarseness, cough within 24 h after removal of i-gel.
Results
A total of 111 patients were included in the analysis. The overall incidence of sore throat within 24 h in the experimental group was significantly lower than that in the control group, as was the incidence at four time points (P<0.05). The VAS scores at the four time points in the experimental group were significantly lower than those in the control group (P<0.05), and the results of repeated measurement analysis of variance showed that time effect and intergroup effect were statistically significant (P<0.001). No differences were found between the groups in the incidence of hoarseness and cough.
Conclusion
Gargling with oral care solution before anesthesia induction can significantly reduce the incidence and severity of POST in patients undergoing i-gel laryngeal mask general anesthesia.
Introduction
To ensure patients’ safety, artificial airways are generally established during general anesthesia, including endotracheal intubation and laryngeal mask airways (LMA). However, it results in a series of throat complications such as sore throat, hoarseness, mucosal injury and throat edema. Among them, postoperative sore throat (POST) is more common and rated by patients as the eighth most unsatisfactory adverse effect after surgery.Citation1 POST is a type of nociceptive pain caused by throat and tracheal mucous membrane injury during intubation, with incidences ranging from 12.1% to 62%.Citation2,Citation3 POST may cause patients to have unpleasant memories of the operation and lower their satisfaction with anesthesia, resulting in compromised postoperative comfort and even prolonged hospital stay.Citation2 Laryngeal mask is a supraglottic airway device, which is an effective alternative to an endotracheal tube to maintain the airway and is widely used in short-term surgery. Since it has the advantages of easier insertion and minimal risk of tissue compression, its associated incidence of POST is less than that of endotracheal tubes.Citation4 Nonetheless, up to 49% of patients experience POST severely due to factors such as insertion technique and subsequent management according to a study.Citation5
At present, a variety of nonpharmacological and pharmacological methods have been used to prevent and treat POST. Nonpharmacological treatments include intubation with a visual laryngoscope, selection of an appropriate size of the endotracheal tube or laryngeal mask, limitation of endotracheal tube cuff pressure and so on. Pharmacological methods mainly include the use of local anesthetics, glucocorticoids, nonsteroidal anti-inflammatory drugs, N-methyl-d-aspartate receptor antagonists and so on. In addition to traditional intravenous injection, atomization inhalationCitation6 and external applicationCitation7 have been proven effective. In recent years, ketamine, dexamethasone and licorice have been made into oral gargles to prevent POST, showing varying degrees of effectiveness.Citation8–10 Oral gargle is convenient to use and is highly acceptable and safe for patients. However, the gargle needs to be prepared with certain requirements in dosage and concentration,Citation11,Citation12 which limits its widespread clinical application. In clinical practice, nurses often use oral care solutions to clean mouth for intubated or critically ill patients to reduce the incidence of oral complications or ventilator-associated pneumonia.Citation13 Chlorhexidine gargle is a common one, which is a broad-spectrum antibacterial and bactericidal drug, with a strong inhibition and killing capacity against both Gram-negative and Gram-positive bacteria. However, whether it can reduce POST has not been reported. We hypothesized that gargling with chlorhexidine oral care solution before anesthesia induction would alleviate POST in patients undergoing laryngeal mask general anesthesia.
The manifestations of POST are typically self-limiting. Compared to treatment, prevention is the best way to improve anesthesia quality and patient satisfaction. Therefore, this study intended to observe the effect of oral care solution on POST in patients undergoing laryngeal mask general anesthesia from the perspective of anesthesia nurses without interfering with the operation methods or the anesthetic drugs usage of anesthesiologists.
Materials and Methods
Study Design
This prospective, randomized, single-blind clinical trial was approved by the Clinical Research Ethics Committee of The First Affiliated Hospital of the University of Science and Technology (No:2021-KY-129; Date:01/07/2021) and registered in the Chinese Clinical Trial Registry (http://www.chictr.org.cn; No: ChiCTR2100048725). Written informed consent was obtained from all patients. A total of 120 patients with American Society of Anesthesiologists (ASA) physical status I–II, aged 18–60 years and body mass index (BMI) of 18.5–30 kg/m2 who were scheduled for laryngeal mask general anesthesia were enrolled. Patients who are allergic to chlorhexidine or with a history of recent respiratory tract infection, sore throat or hoarseness were excluded from study.
Randomization and Blinding
According to the random number table generated by computer, patients were divided into an experimental group (oral care solution) and a control group (0.9% saline). The random grouping scheme was packed and stored in consecutively numbered opaque envelopes. An anesthesia nurse who did not participate in the subsequent study opened each envelope in turn and prepared an oral care solution or 0.9% saline in opaque cups according to the distribution plan. This study could not be performed in a double-blind manner because of the distinct smell and taste of the oral care solution. Nevertheless, postoperative follow-up anesthesia nurse did not know the distribution of patients until the follow-up ended.
Procedures
All patients routinely fasted before operation and received standard monitoring when entering the surgical room, including electrocardiography, noninvasive blood pressure, pulse oxygen saturation and bispectral index (BIS). Five minutes before anesthesia induction, the patient remained seated with his head fully tilted back and gargled with 10mL of oral care solution (Dandong Xin Shi Dai Biotech Pharmaceuticals Co. Ltd, Liaoning, China) or 0.9% saline (Fengyuan Pharmaceutical Co. Ltd, Anhui, China) under the direct observation of an anesthesia nurse. The oral care solution or saline was not swallowed and was spit 1 min later. All side effects related to oral care solution such as allergic reaction were recorded.
General anesthesia was induced with 0.2 mg/kg etomidate, 0.5 μg/kg sufentanil and 0.15 mg/kg cisatracurium. When the BIS was <60 and muscle relaxation was achieved, the patient was in a position of head extension and neck flexion, and the anesthesiologist depressed the jaw slightly, then inserted the single-use i-gel (Intersurgical Ltd, Wokingham, Berkshire, UK), which is a second generation supraglottic airway. The size of i-gel was decided according to the weight of patient. Then, a lubricated gastric tube was inserted through the gastric channel. An effective airway was confirmed by chest auscultation and end-tidal carbon dioxide (PETCO2) waveform. If the first attempt failed, the i-gel was inserted with a jaw thrust maneuver or by changing the head position. If the third attempt failed, endotracheal intubation was performed. Patient was ventilated by a face mask between attempts. The patients were then connected to a mechanical ventilator with 8–10 mL/kg tidal volume and 12–14/min respiratory rate to maintain the PETCO2 in the normal range of 35–45 mmHg. One percent sevoflurane was inhaled, and the target-controlled anesthesia system (TCI) was used to administer remifentanil (2.0–3.0 ng/mL) and propofol (2.0–3.0 μg/mL) to maintain the BIS between 40 and 60.
After the operation, the patient was transferred to the postanesthesia care unit (PACU). The anesthesiologist in PACU decided whether to reverse the neuromuscular block based on the patient’s condition. When the indicator for extubation was reached, the gastric tube was suctioned completely and the i-gel was removed by an anesthesiologist. Any airway injury such as blood on i-gel was noted. Then, patients inhaled oxygen 2–3L/min through the nose. Patients who required more than one attempt for i-gel insertion, who changed to an endotracheal tube midway through the operation, and whose duration of LMA was <1 h or >4 h was considered dropouts and excluded from the analysis.
Data Collection
The primary outcomes were the overall incidence of sore throat within 24 h and incidence at 20 min, 1 h, 6 h, 24 h after removal of i-gel. The incidence of POST was calculated by counting the number of patients with symptoms of sore throat. The secondary outcomes were the severity of sore throat at the four time points and incidence of hoarseness, cough within 24 h after removal of i-gel. The severity was assessed using a visual analog scale (VAS), with a score of 0 (no pain) to 10 (the most severe pain).
Parameters related to the surgery and anesthesia were also recorded, including the time for laryngeal mask insertion, which was defined as the time from inserting the laryngeal mask into the patients’ mouth to the appearance of the first square capnography wave, the anesthesia duration, the surgery duration, and the duration of LMA, which refers to the interval from the successful insertion of the laryngeal mask to the removal of it.
Statistical Analysis
The sample size was determined according to our previous pilot study, which found that the overall incidence of sore throat within 24 h after surgery was 81%. To obtain a clinically significant reduction of 30% in the incidence of POST (ie the incidence of POST is 56%) with a significance level of 0.05 and a power of 80%, each group required 51 patients. Considering the 10% of potential dropout rate, we enrolled 60 patients in each group, with a total of 120.
The data were analyzed using SPSS software (version 22.0; IBM Corp., Armonk, NY, USA). Continuous variables are presented as mean±standard deviation (SD) or median and categorical variables are presented as count and percentage. The Student’s t-test, Mann–Whitney U-test, χ2 test or repeated measurement analysis of variance were used for comparisons. P<0.05 was considered statistically significant.
Results
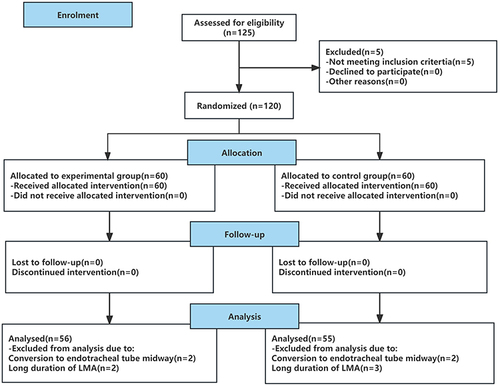
A total of 120 patients participated in the study. Nine patients were excluded from analysis (four in the experimental group and five in the control group). Four patients changed to endotracheal tube because of air leakage during operation, five patients’ LMA duration was more than 4 h. Flow diagram of the study design is shown in .
Figure 1 A flowchart that outlines patient selection, randomization, and analysis.
The types of surgery included were laparoscopic cholecystectomy, laparoscopic appendicectomy, and gynecologic laparoscopic surgery. There were no significant differences in the patient characteristics between two groups (P>0.05) (). No patient experienced side effects related to oral care solution and airway injury.
Table 1 Characteristics of the Study Population
The overall incidence of sore throat within 24 h after removal of i-gel in the experimental group was significantly lower than that in the control group (35.7% vs 69.1%, P<0.05), as was the incidence at 20 min, 1 h, 6 h and 24 h (P<0.05) ().
Table 2 Incidence of Sore Throat After Removal of Laryngeal Mask
The VAS scores of sore throat at 20 min, 1 h, 6 h and 24 h in the experimental group were significantly lower than that in the control group (P<0.05). The result of repeated measurement analysis of variance showed that interaction effect was not significant (F=0.812, P>0.05). The intergroup effect was significant (F=26.878, P<0.001), and the VAS score of the experimental group was significantly lower than that of the control group (P<0.05). The time effect was significant (F=8.832, P<0.001) and the VAS scores at 6 h and 24 h were significantly higher than those at 20 min and 1 h (P<0.05) ().
Table 3 Severity of Sore Throat After Removal of Laryngeal Mask
No difference in the incidence of hoarseness and cough within 24 h after removal of i-gel between the two groups was found (P>0.05) ().
Table 4 The Overall Incidence of Hoarseness and Cough Within 24 h After Removal of Laryngeal Mask
Discussion
Our main results show that gargling with oral care solution before anesthesia induction can significantly reduce the incidence and severity of POST in patients undergoing laryngeal mask general anesthesia. This is the first report on the efficacy of oral care solutions in reducing POST as far as we know.
The occurrence of POST is affected by many factors, such as sex, number of intubation attempts, use of a nasogastric tubeCitation14 and the selection of the supraglottic airway device and its placement technique.Citation15 The incidence of sore throat after laryngeal mask general anesthesia in previous studies ranged from 24% to 49%.Citation5,Citation16–18 However, our study showed an overall POST incidence of 52.3% and up to 69.1% in the control group. The high incidence of POST may be related to the following factors: 91% of patients were female, whose incidence of POST is higher than men.Citation2,Citation19 In addition, 69% of the patients were in the lithotomy position during surgery, which is more likely to lead to POST after laryngeal mask general anesthesia, as reported in previous studies.Citation2 Meanwhile, the establishment of a pneumoperitoneum during operation increased airway pressure and the incidence of POST.Citation20 Our study also found that POST increased with time. The follow-up time in this study was 20 min after removal of i-gel. The residual effect of general anesthesia might mask the early POST. As time went on, patients became more conscious and were allowed to drink and eat, so their feelings for POST were more obvious. These may be reasons for the increase in POST over time. This finding is consistent with another study, which reported a higher incidence of sore throat at 24 h (83.7%) when LMA was used.Citation21
POST is mainly caused by inflammatory reactions of the mucosa of the trachea and pharynx or stimulation due to foreign body insertion.Citation22 Currently, the drugs used in clinics mainly reversibly block the occurrence and transmission of sensory nerve impulses, inhibit the transmission of nociceptive stimuli or suppress inflammatory responses to prevent and treat POST. Drugs are mostly administered through local routes, such as atomization, buccal tablets, external application, and gargles, with high safety and fewer adverse effects but comparable efficacy to intravenous injection.Citation23
Oral mucosa has a thin stratum corneum and many blood vessels, allowing more drugs to enter the blood vessels and exert a pharmacological effect through direct contact with the mucosa. Therefore, various gargles have attracted the attention of researchers. Rudra et alCitation8 studied the effect of ketamine gargle on POST and found that the incidence of POST decreased from 60% to 25%. Lee et alCitation9 found that the incidence of POST decreased from 63% to 33% when dexamethasone gargle was used. Agarwal et alCitation10 used licorice liquid as a gargle and found a significant decrease in the incidence of POST both at rest and during swallowing. However, these gargles all need to be configured and there are no special commercial gargles containing these drugs on the market, limiting their clinical application.
Oral care solution is of great significance to reduce the aggregation of oral pathogenic bacteria and the incidence of oral infection or ventilator-associated pneumonia. The oral care solution used in this study was chlorhexidine gargle, its active ingredient is chlorhexidine gluconate, which is a potent topical antimicrobial cationic compound that interacts with anionic receptor sites on the bacterial cell wall and increases the permeability of bacteria. This nonspecific mechanism of action is highly effective against aerobic and anaerobic Gram-positive and Gram-negative bacteria.Citation24 In the field of oral care practice, chlorhexidine is a potent topical antimicrobial and is used in many countries.Citation25,Citation26 Randomized controlled trials conducted by scholars have shown that topical use of chlorhexidine can reduce the incidence of ventilator-associated pneumonia and nosocomial respiratory infection.Citation27,Citation28 In this study, we found that the overall incidence of POST decreased from 69.1% to 35.7% and the incidence and severity of POST at 20 min, 1 h, 6 h and 24 h were also significantly lower when patients gargled with chlorhexidine oral care solution 5 min before anesthesia induction. In this case, the oral care solution was thought to have a direct effect on the throat mucosa by inhibiting the growth of bacteria and inflammatory reactions, and thus reduced the sore throat after general anesthesia.
Since the endotracheal tube or laryngeal mask comes into contact with vocal organs, they may be damaged during surgery and result in hoarseness after surgery. For patients, hoarseness affects normal life, social interaction and professional performance. Vocal cord injury is the main cause of hoarseness. The insertion of laryngeal masks does not pass through the glottis, which results in slight stimulation to the vocal cords than that of an endotracheal tube, leading to a relatively low incidence of hoarseness. In this study, the incidence of hoarseness in the experimental group was lower than that in the control group; however, the difference was not statistically significant.
The limitation of this study is that it only observed the effect of chlorhexidine oral care solution on POST. The effect of other types of oral care solution remains to be explored. Secondly, we administered the intervening measure only once before induction of anesthesia, and the results showed a short duration of effect, further research is needed. Also, it is a single-center study, and multi-center, large-sample clinical observation is still needed to evaluate the effect of oral care solution on POST.
Conclusions
In summary, gargling with oral care solution before anesthesia induction can significantly reduce the incidence and severity of POST in patients undergoing laryngeal mask general anesthesia. The method is easy to perform and its effect is good, all of which suggest that the treatment is promising for clinical application.
Data Sharing Statement
Data are available from the corresponding author (Xia Chen) on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Clinical Research Ethics Committee of The First Affiliated Hospital of the University of Science and Technology (No:2021-KY-129) and registered in the Chinese Clinical Trial Registry (http://www.chictr.org.cn; No: ChiCTR2100048725). Written informed consent was obtained from all patients. The study was performed in accordance with the ethical standards of the Declaration of Helsinki.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Macario A, Weinger M, Carney S, Kim A. Which clinical anesthesia outcomes are important to avoid? The perspective of patients. Anesth Analg. 1999;89(3):652–658. doi:10.1097/00000539-199909000-00022
- Higgins PP, Chung F, Mezei G. Postoperative sore throat after ambulatory surgery. Br J Anaesth. 2002;88(4):582–584. doi:10.1093/bja/88.4.582
- Xu YJ, Wang SL, Ren Y, Zhu Y, Tan ZM. A smaller endotracheal tube combined with intravenous lidocaine decreases post-operative sore throat - a randomized controlled trial. Acta Anaesthesiol Scand. 2012;56(10):1314–1320. doi:10.1111/j.1399-6576.2012.02768.x
- Gong Y, Xu X, Wang J, Che L, Wang W, Yi J. Laryngeal mask airway reduces incidence of post-operative sore throat after thyroid surgery compared with endotracheal tube: a single-blinded randomized controlled trial. BMC Anesthesiol. 2020;20(1):16. doi:10.1186/s12871-020-0932-2
- Wong DT, Tam AD, Mehta V, Raveendran R, Riad W, Chung FF. New supraglottic airway with built-in pressure indicator decreases postoperative pharyngolaryngeal symptoms: a randomized controlled trial. Can J Anaesth. 2013;60(12):1197–1203. doi:10.1007/s12630-013-0044-2
- Rajan S, Tosh P, Paul J, Kumar L. Effect of inhaled budesonide suspension, administered using a metered dose inhaler, on post-operative sore throat, hoarseness of voice and cough. Indian J Anaesth. 2018;62(1):66–71. doi:10.4103/ija.IJA_382_17
- Tabari M, Soltani G, Zirak N, Alipour M, Khazaeni K. Comparison of effectiveness of betamethasone gel applied to the tracheal tube and IV dexamethasone on postoperative sore throat: a randomized controlled trial. Iran J Otorhinolaryngol. 2013;25(73):215–220.
- Rudra A, Ray S, Chatterjee S, Ahmed A, Ghosh S. Gargling with ketamine attenuates the postoperative sore throat. Indian J Anaesth. 2009;53(1):40–43.
- Lee JH, Kim SB, Lee W, et al. Effects of topical dexamethasone in postoperative sore throat. Korean J Anesthesiol. 2017;70(1):58–63. doi:10.4097/kjae.2017.70.1.58
- Agarwal A, Gupta D, Yadav G, Goyal P, Singh PK, Singh U. An evaluation of the efficacy of licorice gargle for attenuating postoperative sore throat: a prospective, randomized, single-blind study. Anesth Analg. 2009;109(1):77–81. doi:10.1213/ane.0b013e3181a6ad47
- Kuriyama A, Maeda H. Topical application of licorice for prevention of postoperative sore throat in adults: a systematic review and meta-analysis. J Clin Anesth. 2019;54:25–32. doi:10.1016/j.jclinane.2018.10.025
- Kheirabadi D, Ardekani MS, Honarmand A, Safavi MR, Salmasi E. Comparison prophylactic effects of gargling different doses of ketamine on attenuating postoperative sore throat: a single-blind randomized controlled trial. Int J Prev Med. 2021;12:62. doi:10.4103/ijpvm.IJPVM_147_19
- Saddki N, Mohamad Sani FE, Tin-Oo MM. Oral care for intubated patients: a survey of intensive care unit nurses. Nurs Crit Care. 2017;22(2):89–98. doi:10.1111/nicc.12119
- Gemechu BM, Gebremedhn EG, Melkie TB. Risk factors for postoperative throat pain after general anaesthesia with endotracheal intubation at the university of Gondar teaching hospital, Northwest Ethiopia, 2014. Pan Afr Med J. 2017;27:127. doi:10.11604/pamj.2017.27.127.10566
- El-Boghdadly K, Bailey CR, Wiles MD. Postoperative sore throat: a systematic review. Anaesthesia. 2016;71(6):706–717. doi:10.1111/anae.13438
- L’Hermite J, Dubout E, Bouvet S, et al. Sore throat following three adult supraglottic airway devices: a randomised controlled trial. Eur J Anaesthesiol. 2017;34(7):417–424. doi:10.1097/EJA.0000000000000539
- Li X, Wang X, Zhao Y, et al. Incidence of postoperative sore throat after using a new technique of insertion of a second generation Laryngeal Mask Airway: a randomised controlled trial. Eur J Anaesthesiol. 2021;38(3):285–293. doi:10.1097/EJA.0000000000001378
- Oh SK, Lim BG, Kim H, Lim SH. Comparison of the clinical effectiveness between the streamlined liner of pharyngeal airway (SLIPA) and the laryngeal mask airway by novice personnel. Korean J Anesthesiol. 2012;63(2):136–141. doi:10.4097/kjae.2012.63.2.136
- Jaensson M, Gupta A, Nilsson U. Gender differences in sore throat and hoarseness following endotracheal tube or laryngeal mask airway: a prospective study. BMC Anesthesiol. 2014;14:56. doi:10.1186/1471-2253-14-56
- Hu J, Geng G, Li H, Huang S. The changes of cuff pressure in the endotracheal tube during laparoscopic surgery and influence on postoperative sore throat. Chin J Nurs. 2013;48(3):222–223. doi:10.3761/j.issn.0254-1769.2013.03.011
- Ning M, Zhong W, Li J, Wang T, Lu Y. Comparison between I-gel® and endotracheal intubation in terms of the incidence of postoperative sore throat following thyroid surgery: a randomized observational trial. Am J Transl Res. 2022;14(1):373–380.
- Scuderi PE. Postoperative sore throat: more answers than questions. Anesth Analg. 2010;111(4):831–832. doi:10.1213/ANE.0b013e3181ee85c7
- Ki S, Myoung I, Cheong S, et al. Effect of dexamethasone gargle, intravenous dexamethasone, and their combination on postoperative sore throat: a randomized controlled trial. Anesth Pain Med. 2020;15(4):441–450. doi:10.17085/apm.20057
- Genuit T, Bochicchio G, Napolitano LM, McCarter RJ, Roghman MC. Prophylactic chlorhexidine oral rinse decreases ventilator-associated pneumonia in surgical ICU patients. Surg Infect (Larchmt). 2001;2(1):5–18. doi:10.1089/109629601750185316
- Zhang Q, Xie H, He Y, et al. A survey of oral care practice in intensive care units of grade 3A hospitals in China. Chin J Evid Based Med. 2010;10(6):665–669. doi:10.3969/j.issn.1672-2531.2010.06.011
- Rello J, Koulenti D, Blot S, et al. Oral care practices in intensive care units: a survey of 59 European ICUs. Intensive Care Med. 2007;33(6):1066–1070. doi:10.1007/s00134-007-0605-3
- Koeman M, van der Ven AJ, Hak E, et al. Oral decontamination with chlorhexidine reduces the incidence of ventilator-associated pneumonia. Am J Respir Crit Care Med. 2006;173(12):1348–1355. doi:10.1164/rccm.200505-820OC
- DeRiso AJ, Ladowski JS, Dillon TA, Justice JW, Peterson AC. Chlorhexidine gluconate 0.12% oral rinse reduces the incidence of total nosocomial respiratory infection and nonprophylactic systemic antibiotic use in patients undergoing heart surgery. Chest. 1996;109(6):1556–1561. doi:10.1378/chest.109.6.1556