
Abstract
Objective
In the study reported here, single-tablet regimen (STR) versus (vs) multi-tablet regimen (MTR) strategies were evaluated through a cost analysis in a large cohort of patients starting their first highly active antiretroviral therapy (HAART). Adult human immunodeficiency virus (HIV) 1-naïve patients, followed at the San Raffaele Hospital, Milan, Italy, starting their first-line regimen from June 2008 to April 2012 were included in the analysis.
Methods
The most frequently used first-line HAART regimens (>10%) were grouped into two classes: 1) STR of tenofovir disoproxil fumarate (TDF) + emtricitabine (FTC) + efavirenz (EFV) and 2) MTR including TDF + FTC + EFV, TDF + FTC + atazanavir/ritonavir (ATV/r), TDF + FTC + darunavir/ritonavir (DRV/r), and TDF + FTC + lopinavir/ritoavir (LPV/r). Data were analyzed from the point of view of the Lombardy Regional Health Service. HAART, hospitalizations, visits, medical examinations, and other concomitant non-HAART drug costs were evaluated and price variations included. Descriptive statistics were calculated for baseline demographic, clinical, and laboratory characteristics; associations between categorical variables and type of antiretroviral strategy (STR vs MTR) were examined using chi-square or Fisher’s exact tests. At multivariate analysis, the generalized linear model was used to identify the predictive factors of the overall costs of the first-line HAART regimens.
Results
A total of 474 naïve patients (90% male, mean age 42.2 years, mean baseline HIV-RNA 4.50 log 10 copies/mL, and cluster of differentiation 4 [CD4+] count of 310 cells/μL, with a mean follow-up of 28 months) were included. Patients starting an STR treatment were less frequently antibody-hepatitis C virus positive (4% vs 11%, P=0.040), and had higher mean CD4+ values (351 vs 297 cells/μL, P=0.004) than MTR patients. The mean annual cost per patient in the STR group was €9,213.00 (range: €6,574.71–€33,570.00) and €14,277.00 (range: €5,908.89–€82,310.30) among MTR patients. At multivariate analysis, after adjustment for age, sex, antibody-hepatitis C virus status, HIV risk factors, baseline CD4+, and HIV-RNA, the cost analysis was significantly lower among patients starting an STR treatment than those starting an MTR (adjusted mean: €12,096.00 vs €16,106.00, P=0.0001).
Conclusion
STR was associated with a lower annual cost per patient than MTR, thus can be considered a cost-saving strategy in the treatment of HIV patients. This analysis is an important tool for policy makers and health care professionals to make short- and long-term cost projections and thus assess the impact of these on available budgets.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Therapeutic successes against human immunodeficiency virus (HIV) are largely due to the results obtained by scientific research work, which has identified drugs with powerful antiviral activity. Since the mid-1990s, highly active antiretroviral therapy (HAART) has modified the clinical course of HIV infection, reducing the rate of disease progression, the incidence of opportunistic infections, and mortality.Citation1,Citation2 This prolonged survival has changed HIV infection into a chronic disease.Citation3 As a consequence, combination antiretroviral therapy has resulted in longer survival and a better quality of life (QoL) for many HIV-infected patients.Citation4 The most common drug regimen (HAART therapy) administered to patients entering treatment consists of two nucleoside reverse transcriptase inhibitors combined with either a non-nucleoside reverse transcriptase inhibitor, or a “boosted” protease inhibitor.Citation5
The recent development of single-tablet regimens (STRs) has been an important development in the optimization of antiretroviral regimens. Such optimization has the potential to improve long-term adherence, virologic efficacy, clinical outcomes, and QoL.Citation5,Citation6 In the past, several studies have shown treatment simplification strategies could enhance patients’ adherence to HAART.Citation7–Citation9 Although it has been postulated that this type of intervention works by improving the patients’ QoL, some studies have specifically addressed the relationship between QoL and adherence.Citation10 For this reason, it seems important to verify how starting an STR, which determines a simultaneous improvement of the patients’ adherence and QoL, may translate into a potential economic value with a reduced number of HAART tablets in a large cohort of patients starting their first HAART. In a context of limited health care resources, pharmacoeconomic considerations are crucial to help policy makers make the most appropriate decisions on resource allocation.
Patients and methods
We evaluated STR versus (vs) multi-tablet regimen (MTR) strategies through a cost analysis in a large cohort of patients starting their first HAART. Adult HIV-1 naïve patients, followed at the San Raffaele Hospital, Milan, Italy, starting their first-line regimen from June 2008 to April 2012 were included in the analysis. The population included and evaluated in the analysis consisted of subjects having similar and superimposable sociodemographic characteristics at the time of enrollment (June 2008). The patients’ characteristics that determined their selection in the group of pooled data were divided into the following macro-groups: demographics, risk factors for HIV, baseline cluster of differentiation 4 (CD4+) count, baseline HIV-RNA, hepatitis C virus (HCV) coinfection, and disease treatment regimen. The most frequently used first-line HAART regimens (>10%) were grouped into two classes: 1) STR with tenofovir disoproxil fumarate (TDF) + emtricitabine (FTC) + efavirenz (EFV) and 2) MTR including TDF + FTC + EFV, TDF + FTC + atazanavir/ritonavir (ATV/r), TDF + FTC + darunavir/ritonavir (DRV/r), or TDF + FTC + lopinavir/ritoavir (LPV/r). Taking account of summary of product characteristics of Atripla® (STR; Gilead Sciences, Foster City, CA, USA, and Merck and Co., Inc., Whitehouse Station, NJ, USA),Citation11 patients can move from an MTR to an STR within 3 months; in this case, patients were included in the STR group. Patients were excluded in case of missing clinical data (subjects not referring to the center for more than 12 months) or cost information (patients not resident in Lombardy) and treatment regimens to less than 10% of the total first-line HAART regimens at enrollment. All data were anonymously processed and analyzed.
Resource consumption and costs
The analysis of only the comparative costs of alternative treatments is common to all forms of economic evaluation; in such situations, the studies performed may be called “cost analyses.” In this study, cost data were analyzed from the point of view of the Lombardy Regional Health Service (RHS) and HAART, hospitalizations, visits, examinations, and other concomitant non-HAART drugs costs were evaluated, price variations included. The consumption of resources for the patients considered in the analysis was linked to the administration of antiretroviral regimens and other direct health care costs, such as hospitalizations, medical examinations, visits, and laboratory tests. The RHS provides reimbursement for outpatient activities (medical examinations, laboratory and diagnostic procedures), hospital admissions, HAART, and non-HAART drugs to each regional health care structure.Citation12,Citation13 The collected data were therefore real costs incurred by the RHS – that is, bills paid to the (both public and private) providers of services delivered to each patient. Data on non-HAART drugs included all drugs prescribed to a patient and collected at any provider within the Lombardy Region, such as hospitals and pharmacies.Citation14 These data were collected for the study period and anonymously linked to the patients’ clinical and personal data through a univocal code. All collected economic data referred to the year in which they were incurred. Costs were then discounted at the 2012 level, based on the Italian inflation rate of average consumer prices.Citation15 The cost analyses considered the evolution of both total costs and of each cost category between 2008 and 2012. All clinical data were then analyzed to identify patient characteristics that may be related to the costs in each year, taking into account the CD4+ cell count (≤200, 201–350, 351–500, and >500 cells/μL).
Statistical analysis
Descriptive statistics were calculated for baseline demographic, clinical, and laboratory characteristics: means and standard deviations or range were calculated for continuous measures, and frequency (%) for categorical measures. Associations between categorical variables and type of antiretroviral strategy (STR vs MTR) were examined using chi-square or Fisher’s exact tests. The Wilcoxon rank-sum test was applied to detect differences among subjects who started an STR or MTR with respect to distributions of continuous variables. At multivariate analysis, the generalized linear model was used to identify the predictive factors of the overall cost of the first-line HAART regimens; the included covariates were: age, sex, antibody (Ab)-HCV status, HIV risk factors, baseline CD4+, and HIV-RNA. All the recorded variables were entered into the multivariate model. All tests were two-sided and P-values<0.05 were considered statistically significant. Statistical analyses were performed using SPSS Statistics (v 19.0; IBM Corp, Armonk, NY, USA) and NCSS (v 8.0; NCSS, East Kaysville, UT, USA).
Results
shows the main baseline characteristics. Included in the study was data for 474 naïve patients (90% male, mean age 42.2 years, mean baseline HIV-RNA 4.50 log10 copies/mL, CD4+ count of 310 cells/μL, with a mean follow-up of 28 months). Patients starting an STR treatment were less frequently anti-HCV Ab (antibodies anti-HCV) positive (4% vs 11%, P=0.040), and had higher mean CD4+ values (351 vs 297 cells/μL, P=0.004) than MTR patients. and show immunological and virological trends after the start of the antiretroviral therapy and independently from switch. After 12 and 24 months since the start of HAART, 93% and 94% of STR patients and 89% and 91% of MTR patients, respectively, had an HIV-RNA <50 copies/mL. Similar CD4+ recovery in both STR and MTR patients was also observed.
Figure 1 Results: immunological (A) and virological (B) trends during follow-up according to single- or multi-tablet antiretroviral regimens.
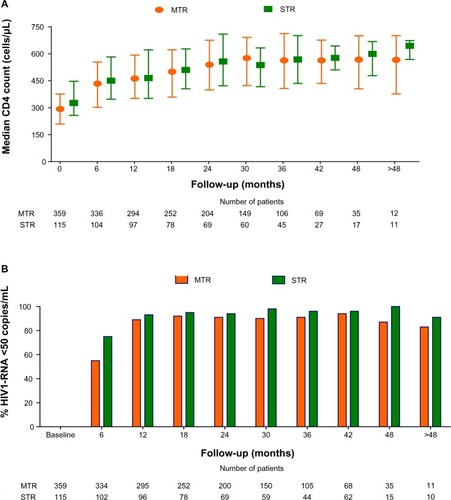
Table 1 Baseline characteristics of the 474 antiretroviral-naïve HIV-1 infected patients
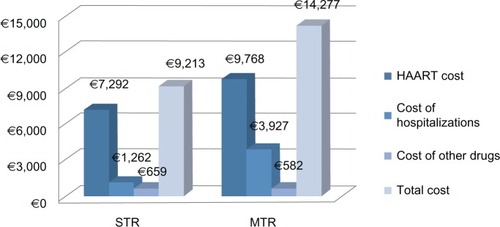
The mean annual cost per patient was €9,213.00 (range: €6,574.71–€33,570.00) among STR patients and €14,277.00 (range: €5,908.89–€82,310.30) among MTR patients. Thus, STR was found to be less costly per patient than MTR ().
Figure 2 Results: mean year cost per patient for STR versus MTR (in Euros).
Multivariate analysis () revealed the mean cost to be significantly lower among patients starting an STR treatment than among those starting an MTR regimen (adjusted mean: €12,096.00 vs €16,106.00, P=0.0001). It is interesting to notice that the year cost for patients was inversely correlated with CD4+ levels (cells/μL): decreasing immunological values, were associated with increasing mean annual cost per patient. However, the mean annual cost per patient was statistically lower for the STR group than for the MTR group (P=0.0001).
Table 2 Multivariate analysis (generalized linear model): factors associated with the overall cost (costs include antiretroviral regimens and hospitalizations and non-antiretroviral treatments)
Discussion
The availability of HAART has modified the natural progression of HIV infection, resulting in an increased survival of sero-positive subjects.Citation16 Adding new single-tablet antiretroviral regimens to conventional therapies can be useful to physicians in choosing the best possible therapy in the treatment of HIV.
However, since STR is not the only available therapeutic option, we deemed it necessary to carry out a pharmacoeconomic comparison with other antiretroviral regimens, taking into account treatments endorsed – though with different degrees of recommendation – by Italian guidelines. Various comparison models for the cost and effectiveness of different therapeutic regimens have recently been reported in the literature, with particular reference to the Italian situation.Citation17–Citation20 These research studies were developed with the use of decision models to highlight any differences in terms of cost per quality-adjusted life years (QALYs) among the different therapeutic regimens. In contrast, in our research we tried to identify the real cost of HIV patients in a hospital setting, based on the costs actually borne by the Italian National Health Service. The results obtained show that STR is the less costly treatment strategy in comparison with the other therapeutic regimens based on MTR. The mean annual cost per patient emerging from our research is basically consistent with a recent analysis of real treatment costs of HIV patients.Citation21,Citation22 These two studies, carried out on the administrative database of the Lombardy Region reimbursements for the years 2007–2009, show a mean annual cost per patient of €11,734.00 (lower 95% confidence limit [CL]: €11,057.00; upper 95% CL: €12,412.00). In our research, we estimated the mean annual cost per patient as €9,213.00 for the STR group and €14,277.00 for the MTR group. The multivariate probabilistic sensitivity analysis of the main variables confirmed the base case validity. In particular, it is important to highlight that the worsening of the patients’ condition (CD4 drop) corresponds to an increase in the mean annual cost for all patients.Citation19,Citation21,Citation22
In our study, the CD4 levels in the STR group were constantly higher than in the MTR group. It is important to remember that it is possible to correlate the expressed results in terms of CD4, as in other studies,Citation17–Citation19 to utility scores calculated on the EQ-5D™ (www.euroqol.org), as follows: for CD4 values >500 cells/μL, the utility score was 0.9460; for CD4 values 351–500 cells/μL, the utility score was 0.9330; for CD4+ values 201–350 cells/μL, the utility score was 0.9310; and for CD4+ values ≤200 cells/μL, the utility score was 0.8300.Citation23 As reported by many published papers,Citation17–Citation19 the association of CD4 levels with QoL values imply the complete superiority of the STR strategy (ie, less costly and more effective), which involves lower costs and more preference elements due to the patients’ QoL. A recent publication demonstrated that all these elements could contribute to determine a maximum potential “premium price” of 29% to be assigned to an STR for HIV-infected patients.Citation24
The results of this study need to be interpreted considering some limitations. First, the adoption of a 48-month time interval for the STR vs MTR comparison may not have been sufficient to highlight the long-term effects and complications of HAART A second limitation is that the statistical analysis did not include some additional predictive factors, such as renal function and baseline resistance; with few exceptions, all the therapies were prescribed based on resistance test, clinical history, and safety issues of the patients. Third the patient sample size was not significant with respect to the HIV-infected Italian population. Compared with similar research work,Citation19 our sample comprised data for 474 instead of 194 patients, and our time horizon was 4 years instead of 2. However, in spite of these increases in sample size and time of observation, our pharmacoeconomic analysis still confirms a cost reduction per HIV patient treated with an STR vs an MTR. Fourth, not all treatment options available for HIV patients were considered in this cost analysis. Another consideration that should be taken into account is that we found treatment costs that were high for both high and low baseline CD4 counts; the high cost may be related to the fact that we included all hospitalizations, visits, and examinations that may also occur in patients with a high CD4+ count. Our results should be evaluated in a more general context, because it is reasonable to assume that many MTR regimens were prescribed because of legitimate concerns such as central nervous system symptoms, chronic kidney disease, and resistance profile. Nevertheless, the availability of data on drug costs may help the clinician to constructively compare the cost and effectiveness of future regimens.
The favorable result of the STR in our study is probably due to the better adherence of patients to an STR – reported in the literature – determining an increase in the QoL of HIV patients.Citation10,Citation24,Citation25 It is now recognized that low antiretroviral adherence is strictly linked with treatment failureCitation26 and therefore indicators of HIV disease progression such as virologic failure,Citation27 insufficient immunological reconstitution, clinical disease progression, and death.Citation28,Citation29 We can also consider that in our study, adherence is predicative of having an undetectable viral load, but the percentage of patients reaching an undetectable viral load was almost the same in both groups. Adherence to therapy is not only necessary to obtain a therapeutic result in patients starting treatment but also to maintain an effective viral suppression in the course of time.Citation30
STRs are an effective therapeutic option that eliminate the possibility of selective nonadherence (in which only part of a regimen is taken) and, consequently, help reduce virological failure and eventual disease progression.Citation24,Citation25 Measuring and comprehending the concept of adherence to STR therapy in HIV patients are critical factors in determining the effectiveness and safety of the regimen, but they are also important to create programs aimed at improving the quality of medicine use.Citation31 The results of our study may be, for instance, applied to other hospital settings in the regional/national area to define and compare mean standard costs of illness that are consolidated by the wide denominator considered in our work. The appropriate prescription of drugs is of critical importance to reach therapeutic objectives and to optimize the use of resources in modern health systems.
Conclusion
In our study, STR was associated with a lower annual cost per patient than MTR, thus can be considered a cost-saving strategy in the treatment of HIV patients. This analysis is an important tool for policy makers and health care professionals to make short- and long-term cost projections and thus assess the impact of these on available budgets.
Disclosure
This research was supported by Gilead Sciences Srl, Milan, Italy. The authors are employees of independent research organizations and maintained independent scientific control over the study, including data analysis and interpretation of final results.
References
- MocroftALedergerberBKatlamaCEuroSIDA study groupDecline in the AIDS and death rates in the EuroSIDA study: an observational studyLancet20033629377222912853195
- Antiretroviral Therapy Cohort CollaborationLife expectancy of individuals on combination antiretroviral therapy in high-income countries: a collaborative analysis of 14 cohort studiesLancet7262008372963529329918657708
- VolberdingPADeeksSGAntiretroviral therapy and management of HIV infectionLancet20103769734496220609987
- FreedbergKALosinaEWeinsteinMCThe cost effectiveness of combination antiretroviral therapy for HIV diseaseN Engl J Med20013441182483111248160
- National Committee on AIDS, Ministry of Health National Commission for the Fight Against AIDSLinee Guida Italiane sull’utilizzo dei farmaci antiretrovirali e sulla gestione diagnostico-clinica delle persone con infezione da HIV-1 [Italian guidelines on antiretroviral drugs and the diagnostic-clinical management of HIV patients]2012 Italian. Available at: http://www.salute.gov.it/imgs/C_17_pubblicazioni_1793_allegato.pdfAccessed September 15, 2013
- NachegaJBRosenkranzBPhamPATwice-daily versus once-daily antiretroviral therapy and coformulation strategies in HIV-infected adults: benefits, risks, or burden?Patient Prefer Adherence2011564565122259241
- MaggioloFRipamontiDAriciCSimpler regimens may enhance adherence to antiretrovirals in HIV-infected patientsHIV Clin Trials20023537137812407486
- StoneVEJordanJTolsonJMillerRPilonTPerspectives on adherence and simplicity for HIV-infected patients on antiretroviral therapy: self-report of the relative importance of multiple attributes of highly active antiretroviral therapy (HAART) regimens in predicting adherenceJ Acquir Immune Defic Syndr200436380881615213564
- BoyleBAJayaweeraDWittMDGrimmKMaaJFSeekinsDWRandomization to once-daily stavudine extended release/lamivudine/efavirenz |versus a more frequent regimen improves adherence while maintaining viral suppressionHIV Clin Trials20089316417618547903
- AiroldiMZaccarelliMBisiLOne-pill once-a-day HAART: a simplification strategy that improves adherence and quality of life of HIV-infected subjectsPatient Prefer Adherence2010411512520517472
- European Medicines Agency (EMA)Atripla [summary of European public assessment report]LondonEMA2009 [updated October 3, 2012]. Available at: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/000797/human_med_000657.jsp&murl=menus/medicines/medicines.jsp&mid=WC0b01ac058001d125Accessed June 10, 2013
- Lombardy RegionSocial and Health Care Plan. No. 937/2010MilanLombardy Region2010 Italian. Available at: http://www.sanita.regione.lombardia.it/shared/ccurl/956/366/DGRregole_e_allegati.zipAccessed June 10, 2012
- Lombardy RegionApprovazione del documento avente peroggetto Percorso Diagnostico Terapeutico (PDT) per il paziente affetto da malattia HIV/AIDS [Therapeutic and diagnostic path (PDT) for the patient with HIV/AIDS disease] Decree no 7485852011MilanLombardy Region2012 Italian. Available at: http://www.sanita.regione.lombardia.it/cs/Satellite?c=Page&childpagename=DG_Sanita/Page/NormativaDetail&pagename=DG_SANWrapper&cid=1213275902673&keyid=3520Accessed June 10, 2012
- Agenzia Italiana del Faramco [AIFA; Italian Drug Agency]Negoziazione e rimborsabilitá [Negotiation and reimbursement; web page on the Internet]RomeAIFA2013 Italian. Available at: http://www.agenziafarmaco.gov.it/it/content/negoziazione-e-rimborsabilit%C3%A0Accessed November 13, 2011
- IstatIndice dei prezzi al consumo per le rivalutazioni monetarie [Consumer Price Index for inflation adjustments]RomaIstituto nazionale di statistica Available from: http://www.istat.it/it/archivio/30440Accessed November 7, 2013
- LiottaGCaleoGMMancinelliSAnalysis of survival in HIV-infected subjects according to socio-economic resources in the HAART eraAnn Ig20082029510418590041
- MoeremansKAnnemansLLöthgrenMCost effectiveness of darunavir/ritonavir 600/100 mg bid in protease inhibitor-experienced, HIV-1-infected adults in Belgium, Italy, Sweden and the UKPharmacoeconomics201028Suppl 110712821182347
- ColomboGLColangeliVDi BiagioADi MatteoSViscoliCVialePCost-effectiveness analysis of initial HIV treatment under Italian guidelinesClinicoecon Outcomes Res2011319720522163167
- RizzardiniGBonfantiPCarenziLCost-effectiveness analysis of HIV treatment in the clinical practice of a public hospital in northern ItalyTher Clin Risk Manag2012837738423028230
- FogliaEBonfantiPRizzardiniGCost-utility analysis of lopinavir/ritonavir versus atazanavir + ritonavir administered as first-line therapy for the treatment of HIV infection in Italy: from randomised trial to real worldPLoS One201382e5777723460905
- RizzardiniGRestelliUBonfantiPThe cost of HIV disease in Northern Italy: the payer’s perspectiveJ Acquir Immune Defic Syndr201157321121721546850
- RizzardiniGRestelliUBonfantiPCost of human immunodeficiency virus infection in Italy, 2007–2009: effective and expensive, are the new drugs worthwhile?Clinicoecon Outcomes Res2012424525222973114
- SimpsonKNLuoMPChumneyESunEBrunSAshrafTCost-effectiveness of lopinavir/ritonavir versus nelfinavir as the first-line highly active antiretroviral therapy regimen for HIV infectionHIV Clin Trials20045529430415562370
- ColomboGLDi MatteoSMaggioloFAntiretroviral therapy in HIV-infected patients: a proposal to assess the economic value of the single-tablet regimenClinicoecon Outcomes Res20135596823430273
- AntinoriAMarcotullioSAmmassariAItalian HIV Guidelines Working GroupItalian guidelines for the use of antiretroviral agents and the diagnostic-clinical management of HIV-1 infected persons. Update 2011New Microbiol201235211315922707127
- d’Arminio MonforteALepriACRezzaGInsights into the reasons for discontinuation of the first highly active antiretroviral therapy (HAART) regimen in a cohort of antiretroviral naïve patients. I.CO.N.A. Study Group. Italian Cohort of Antiretroviral-PatientsAIDS200014549950710780712
- PatersonDLSwindellsSMohrJAdherence to protease inhibitor therapy and outcomes in patients with HIV infectionAnn Intern Med20001331213010877736
- BangsbergDRPerrySCharleboisEDNon-adherence to highly active antiretroviral therapy predicts progression to AIDSAIDS20011591181118311416722
- LimaVDHarriganRBangsbergDRThe combined effect of modern highly active antiretroviral therapy regimens and adherence on mortality over timeJ Acquir Immune Defic Syndr200950552953619223785
- AntinoriACozzi-LepriAAmmassariAAdICoNA Study GroupRelative prognostic value of self-reported adherence and plasma NNRTI/PI concentrations to predict virological rebound in patients initially responding to HAARTAntivir Ther20049229129615134192
- BorghiCCiceroAFGAderenza e persistenza in terapia. [Adherence and persistence in therapy]Giornale Italiano di Farmacoeconomia e Farmaco Utilizzazione200812513 Italian