Abstract
Background
Diabetic foot complications are a leading cause of lower extremity amputation. With the increasing incidence of diabetes mellitus in the Arab world, specifically in the Kingdom of Saudi Arabia, the rate of amputation will rise significantly. A diabetic foot care program was implemented at King Abdulaziz Medical City in Riyadh, Saudi Arabia, in 2002. The program was directed at health care staff and patients to increase their awareness about diabetic foot care and prevention of complications. The purpose of this study was to perform a primary evaluation of the program’s impact on the rate of lower extremity amputation due to diabetic foot complications.
Method
This pilot study was the first analysis of the diabetic foot care program and examined two groups of participants for comparison, ie, a “before” group having had diabetic foot ulcers managed between 1983, when the hospital was first established, and 2002 when the program began and an “after group” having had foot ulcers managed between 2002 and 2004, in the program’s initial phase. A total of 41 charts were randomly chosen retrospectively. A data sheet containing age, gender, medical data, and the presentation, management, and outcome of diabetic foot cases was used for the analysis.
Results
The before group contained 20 patients (17 males) and the after group contained 21 patients (16 males). There was no difference between the two groups with regard to age and comorbidities. The rate of amputation was 70% in the before group and 61.9% in the after group. There was a decrease in the percentage of toe amputation in the after group and an increase in the percentage of below-knee amputation in the before group. However, these changes were not significant.
Conclusion
The program, although evaluated at an early stage, has increased the awareness of both patients and health care staff about the prevention and management of diabetic foot disease, and decreased the rate of lower extremity amputation. We believe that the statistical proof of its impact will be evident in the final evaluation.
Introduction
Foot complications from diabetes are one of the main causes of amputation and its subsequent physical and emotional problems. Peripheral vessels and nerve disorders may lead to foot ulcers, and superadded infection can cause foot gangrene. This problem is one of the main reasons for admission of diabetic patients to hospital, and leads to billions of dollars in medical expenses worldwide.Citation1,Citation2 In Saudi Arabia and the Arab world, the incidence is even higher.Citation3–Citation5 Diabetes-related lower extremity conditions that increase the risk for amputation among people with diabetes include peripheral neuropathy, peripheral vascular disease, and infection.Citation6 Peripheral neuropathy may cause loss of sensation in the feet, resulting in a patient’s failure to perceive foot problems, and may cause development of foot deformities that increase pressure points susceptible to ulceration. Osteomyelitis and gangrene may develop from inadequate blood supply and infection. Risk factors for amputation include being older, male, or a member of certain racial/ethnic groups, having poor glycemic control, having diabetes for a longer period, and practicing or receiving poor preventive health care.Citation7
Lower extremity amputation, a devastating consequence of diabetes, remains a very common outcome of diabetic foot complications.Citation8,Citation9 Indeed, people with diabetes are 10–15 times more likely to require lower extremity amputation than non-diabetic individuals, with a 30%–50% higher risk of undergoing a second amputation. Furthermore, the mortality rate for patients undergoing amputation is 6%. Amputation is not only a costly outcome for patients, but also expensive for the health care system. In one estimate, managing one patient with an amputation will cost around $40,000 to $75,000.Citation10–Citation12
A recent national study on the prevalence of diabetes in Saudi Arabia revealed that 25% of Saudis over 40 years of age have diabetes.Citation13 Given these statistics, the economic and social implications are apparent and significant.
The diabetic foot care program implemented at King Abdulaziz Medical City in Riyadh in 2002 is a comprehensive approach to maintaining the health of diabetic patients’ feet in order to reduce the lower limb amputation rate, thereby dramatically reducing the cost to patients, society, and the health care system. Knowledgeable and consistent care can help patients avoid the potential problems that may lead to amputation. The patients’ continued walking ability and quality of life depend on close inspection, proper footwear, a few specific “do’s and don’ts”, and the commitment of the medical care team.Citation14
The purpose of this retrospective study was to evaluate the initial impact of the program on the rate of lower extremity amputation due to diabetic foot complications.
Methods
In 2002, a diabetic foot care team was formed to revise and establish a proposed diabetic foot care program. The members were specialists involved in diabetic foot management and professionals who had an interest in the program. The team consisted of a vascular surgeon, a diabetologist, an infectious disease internist, a diabetic educator, surgical and medical nurses, and a general surgeon. The aim of the program was to determine the impact of a diabetic foot education program on the prevention and outcomes of diabetic foot complications in our main hospital and satellite primary care clinics. The objectives were to increase the knowledge of patients and health care staff about diabetic foot care, to increase the skills of patients and staff regarding methods for diabetic foot care in order to prevent and manage diabetic foot lesions, and to encourage health care staff to undertake regular foot examination and foot care education in their practice.
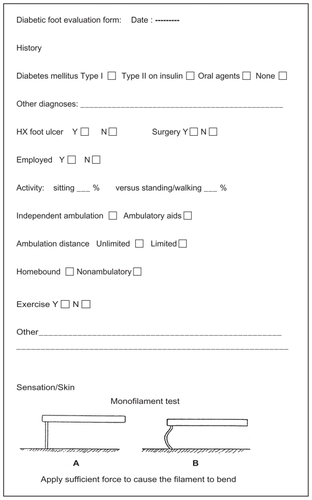
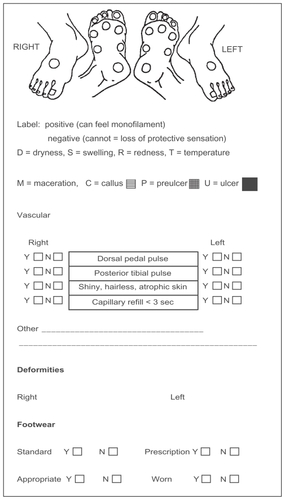
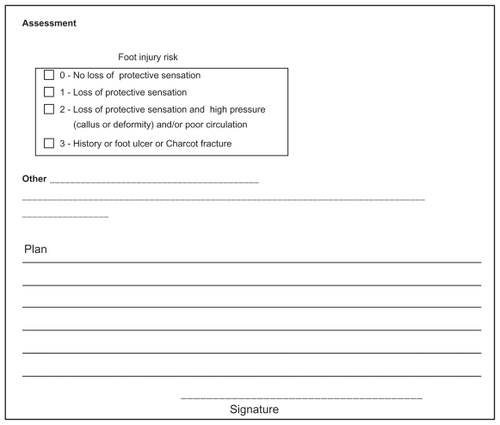
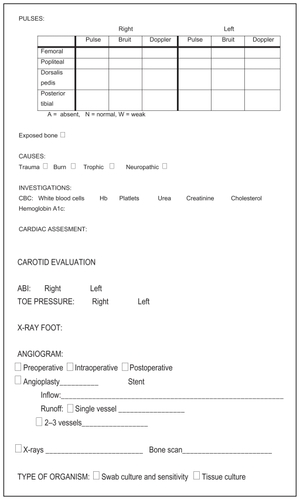
The program included foot care education for health care staff, which included the following elements: how to stratify and manage patients in low- and high-risk categories, for which a screening data sheet was provided (); how to apply standard wound care practice protocols; and how to follow the guidelines set out in the institution’s referral system for patients with either low- or high-risk diabetic foot problems, including early referral of high-risk patients to a specialist. The education methods for health care staff consisted of lectures on diabetic foot care given at regular intervals and in regular diabetic foot workshops. These workshops were one-day activities conducted by the diabetic foot team. All health care providers in our hospital and satellite clinics caring for diabetes patients were permitted to attend. The morning program consisted of didactic lectures with photographic illustrations, as well as interactive discussions. In the afternoon program, the participants divided into groups and rotated among stations. The first station involved hands-on practice on how to assess foot vascularity and was taught by a vascular surgeon. In the second station, a physician instructed participants on how to assess for the presence of neuropathy. The third station was taught by a diabetic foot educator who gave participants general knowledge about the importance of footwear, examples of major amputation caused by improper footwear, and various examples of foot deformities and minor amputations. By the end of 2004, four workshops had been conducted, with a total of 98 participants. Patient education was mainly provided by a diabetic educator, who conducted educational series and distributed educational pamphlets.
Appendix 1 King Abdulaziz Medical City Diabetic Foot Program screening sheet.
The diabetic foot team monitored the program through feedback from health care staff and patients. Questionnaires were conducted at the end of every activity (workshops and lectures) and short questionnaires were given at random time points to evaluate patient and staff knowledge about the program. These were used to evaluate the program and determine how it could be improved. Program information and results were entered in the hospital’s data system.
Our aim is to re-evaluate the program’s impact at the end of 2012, ie, 10 years after its inception. However, in this primary evaluation, the program’s initial results (from 2002 to the end of 2004) were analyzed.
The sample size for this study was 41 patients at King Abdulaziz Medical City in Riyadh. The hospital uses the International Classification of Diseases, Eighth Revision, Clinical Modification (ICD-8-CM). The ICD-8-CM system provides codes to classify a wide variety of signs, symptoms, abnormal findings, complaints, social circumstances, and external causes of injury or disease. After approval from the research committee at the hospital and the university, we chose diabetic foot ulcers and cellulitis as codes with which to collect the sample populations.
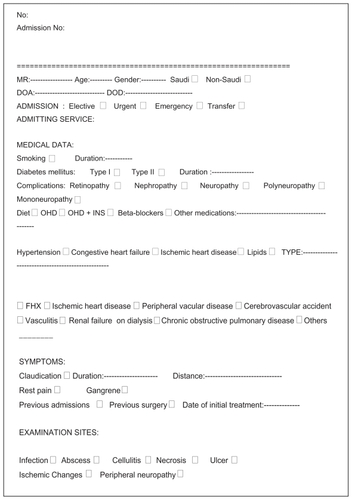
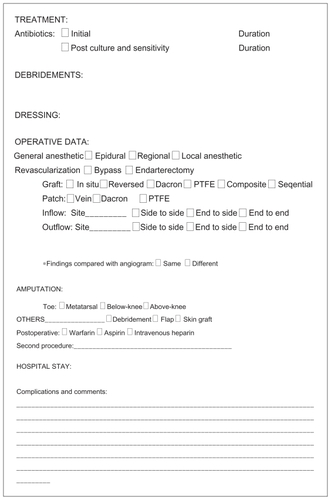
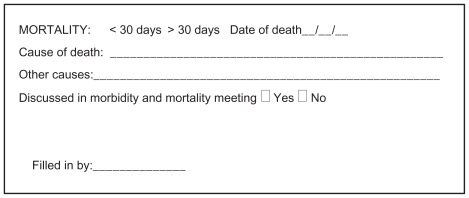
For this first analysis, a total of 41 charts were randomly chosen and retrospectively reviewed. Twenty belonged to patients who presented with diabetic foot complications between 1983 and 2002 (the “before group”), and 21 to patients who presented with such complications in the program’s first two years, from 2002 to 2004 (the “after” group). Patients were evaluated by searching each patient’s hospital record for previous admissions and outpatient visits related to diabetic foot complications. A data sheet () designed to include multiple parameters related to diabetic foot management, was completed by a medical student, and supervised and revised by the author. Demographic data included gender, age, type, complications, duration of diabetes, comorbidities, presentation, investigations, and operative data. Only data pertaining to the objectives of our study were analyzed. The outcome of each group’s diabetic foot ulcers, ie, either healing or amputation, was compared. The data were analyzed using the SPSS program (SPSS Inc., Chicago, IL). Chi-square tests were used to compare categoric data and t-tests were used for both categoric and continuous measures. Statistical significance was declared for one-tailed P values of 0.05.
Appendix 2 King Abdulaziz Medical City, Diabetic Foot Care Program data sheet.
Results
For the purpose of this evaluation, data pertaining to the objectives of our study were analyzed. Theses were demographic data, diabetes duration, risk factors for development of diabetic foot complications, clinical presentation, and the outcome of the diabetic foot complication. Males comprised 76.2% of the after group and 85% of the before group. The mean age was 61.1 years for the after group and 58.6 years for the before group. The mean duration of diabetes in both groups was not significant. In the after group, the mean duration was 16.83 years, with a standard deviation of 8.34 years, with nine patients missing documentation of diabetes duration. In the before group, the mean duration was 13.29 years with a standard deviation of 10 years, with four undocumented patients (). There were no neuropathies in the before group, while 23.8% of the after group had neuropathies. There were also no vascular problems in the before group, while 4.8% of the after group had vascular problems. All patients in the after group presented with an ulcer, compared with 85% of the before group. Patients in the after group also had a higher chance of presenting with gangrene and osteomyelitis (63.3% and 42.9%, respectively), (). The overall amputation rate was higher in the before group at 70% than in the after group (70% versus 61.9%, respectively). Toe amputation was lower in the after group at 28.6%, while below-knee amputation was higher in the before group at 33.3% ().
Table 1 Patient demographic data, comorbidities, and complications
Table 2 Presentations and investigations
Table 3 Amputation level
Discussion
The study shows that there was an 8.1% reduction in amputation rate after implementation of the program, but this was not statistically significant. The percentage of the cases that required amputation at the level of the toes was actually lower in the before group, while the percentage of patients who required amputation at below-knee level was higher in the after group. In addition, one case required above-knee amputation, which represents 5% of the before group. We observed that there were no neuropathies in the before group, while 23.8% of the after group had neuropathies. There were also no vascular problems in the before group, while 4.8% of the after group had vascular problems.
The literature is replete with studies demonstrating the major impact of increasing patients’ and health care providers’ awareness about foot care and changing their behaviors and practices regarding the prevention of ulcers and amputation. For instance, Lavery et al found that implementing a lower extremity disease management program consisting of screening and treatment protocols for diabetic members in a managed care organization decreased the incidence of amputations by 47.4%.Citation15–Citation19 Studies from several countries have shown that increasing awareness of diabetic foot care, as well as its prevention and proper management, resulted in a 50% reduction in major amputation rates.Citation20–Citation22 However, those studies are reported from developed countries. Few to none of the developing countries have implemented such a program, although they have a higher incidence of diabetes and diabetic foot complications. To our knowledge, our program is the first attempt to implement such a program in our part of the world.
We believe that the following factors might have affected our results. The differences in neuropathy, vasculopathy, and other risk factors for diabetic foot complications were mainly due to highly deficient chart documentation in the before group, which demonstrates the low awareness of the diabetic foot problem in general. Despite this, the encouraging finding was that all patients in the after group presented with a foot ulcer. This could be due to the increased awareness of the general practitioners or other front-line physicians who participated in the program and became more aware of the importance of referring patients with early ulcers to a specialist. In addition, patients educated in the program learned to seek immediate medical advice when they found any lesions on their feet. This could explain the lower percentage of toe amputation in the after group, which may have decreased due to early management of foot ulcers. On the other hand, the after group had a higher percentage of below-knee amputation. This could be explained by the random selection of charts or by the presentation of patients from other cities or hospitals with no foot care program (because our hospital is a tertiary centre, difficult or poorly managed cases are often referred). Our initial results did not replicate other international experience, which has established the effectiveness of establishing a diabetic foot care program in reducing the amputation rate. Nevertheless, this was also the experience of some other programs in their initial stages.Citation23,Citation24
Given that this was a pilot study, limitations include a small sample size, a short duration of follow-up, and missing data in the charts of both groups. In addition, the after group was chosen too early, so the protocols of the program had not yet been well implemented or disseminated to all health care providers. The poor compliance of patients with follow-up and prevention education is also an important factor. Other factors that are unique to our part of the world no doubt represent an important contribution to the delay in obtaining the required results of the program. These include education (because there is a high percentage of illiterate people in the community), the media (which pays less attention to medical problems here than in other countries), and the common belief that traditional management (herbal medicine, cautery, bloodletting) is more effective than modern medicine.Citation3,Citation5 The latter is, in the author’s view, the main determining factor.
Based on the results we have seen since 2004, we believe that our program will have a significant impact on reducing the rate of amputation due to diabetic foot complications, and this will be demonstrated in our next evaluation. Patients, health care staff, and even hospital admission censuses are showing a decrease in the rate of advanced diabetic foot complications. Operating room statistics are also showing a decline in amputation procedures. Moreover, general practitioners and endocrinologists are reporting changes in patients’ behavior regarding foot care, and patients frequently ask that their feet be checked at all visits. The pattern of referral to our vascular clinic has changed from advanced diabetic foot lesions to early ulcers.
Educating health care staff and patients about diabetic foot complications and increasing their awareness will no doubt have a significant impact on reducing the rate of amputation; however, it will require commitment and patience to achieve the required results, especially in communities where education is still growing, as in developing countries. Achieving these results will encourage hospital administrators and policy makers to support and disseminate the program to other institutions.
Developing countries differ in their amount of resources and level of government support. Our program does not require financial support or advanced resources, so we recommend its use in all developing countries with diabetic foot crises, because it is easily conducted without financial burden. It only requires a caring enthusiastic group of health care staff who can adapt the program and tailor it to their capabilities in order for good long-term results to be achieved.
Conclusion
Although our initial results did not replicate those of other international studies which have shown the effectiveness of diabetic foot care programs in reducing the amputation rate, we have found that this was the experience of some other programs in their initial stages. Therefore, we believe that the second stage of evaluation will demonstrate a significant improvement in the lower limb amputation rate of diabetic patients in our hospital.
Disclosure
The author reports no conflict of interest in this work, which was presented at the 11th Annual Congress of Asian Society for Vascular Surgery and the Fourth Annual Meeting of the World Federation of Vascular Surgery Societies in 2010.
References
- GoodridgeDTrepmanEEmbilJMHealth-related quality of life in diabetic patients with foot ulcers: Literature reviewJ Wound Ostomy Continence Nurs20053236837716301902
- Ragnarson-TennvallGApelqvistJPrevention of diabetes related foot ulcers and amputations: A cost-utility analysis based on Markov model simulationsDiabetologia2001442077208711719840
- Al-WahbiAMThe diabetic foot in the Arab worldSaudi Med J20062714715316501666
- WrobelJSMayfieldJAReiberGEGeographic variation of lower-extremity major amputation in individuals with and without diabetes in the Medicare populationDiabetes Care20012486086411347744
- Al-WahbiAMGillGThe diabetic foot in the Arab worldDiabetes in the Arab WorldCambridgeFSG Communications2005
- BoultonAJThe pathogenesis of diabetic foot problems: An overviewDiabetes Med1996131216
- DargisVPantelejevaOJonushaiteAVileikyteLBoultonAJBenefits of a multidisciplinary approach in the management of recurrent diabetic foot ulceration in Lithuania: A prospective studyDiabetes Care2009221428143110480504
- JohannessonAIncidence of lower limb amputation in the diabetic and non-diabetic general population: A 10-year population-based cohort study of initial unilateral, contralateral and re amputationsDiabetes Care20093227528019001192
- Calle-PascualALRedondoMJBallesterosMNontraumatic lower extremity amputations in diabetic and non-diabetic subjects in Madrid SpainDiabetes Metab1997235195239496558
- ReiberGELipskyBAGibbonsGWThe burden of diabetic foot ulcersAm J Surg1998176510
- PelqvistJLarssonJWhat is the most effective way to reduce incidence of amputation in the diabetic footDiabetes Metab Res Rev200016S758311054894
- KingLBImpact of a preventive program on amputation rates in the diabetic populationJ Wound Ostomy Continence Nurs20083547948218794698
- Al-NozhaMMAl-MaatouqMAAl-MazrouYYDiabetes mellitus in Saudi ArabiaSaudi Med J2004251603161015573186
- HolsteinPESorensenSLimb salvage experience in a multidisciplinary diabetic foot unitDiabetes Care200922B9710310097908
- LarssonJApelqvistJTowards less amputations in diabetic patients. Incidence, causes, cost, treatment, and prevention: A reviewActa Orthop Scand2005661811927740955
- LaveryLAWunderlichRPTredwellJLDisease management for diabetic foot: Effectiveness of a diabetic foot prevention program to reduce amputations and hospitalizationsDiabetes Res Clin Pract200570313716126121
- Calle-PascualALDuranAA preventive foot care program for people with diabetes with different stages of neuropathyDiabetes Res Clin Pract20025711111712062856
- MaloneJMSnyderMPrevention of amputation by diabetic educationAm J Surg19891585205232589581
- McCabeCJStevensonRCDolanAMEvaluation of diabetic foot screening and prevention programDiabetes Med1998158084
- MorelandMEKilbourneAMEngelhardtJBDiabetes preventive care and non-traumatic lower extremity amputation ratesJ Health Qual2004261217
- AssalJPMehnertHTritschlerHJOn your feet! Workshop on the diabetic footJ Diabetes Complications20021618319412039404
- van GilsCCWheelerLAMellstromMAmputation prevention by vascular surgery and podiatry collaboration in high-risk diabetic and non diabetic patients. The Operation Desert Foot experienceDiabetes Care19992267868310332665
- ArgisVPantelejevaOJonushaiteAVileikyteLBoultonAJBenefits of a multidisciplinary approach in the management of recurrent diabetic foot ulceration in Lithuania: A prospective studyDiabetes Care20092214281431
- SinghNArmstrongDGLipskyBAPreventing foot ulcers in patients with diabetesJAMA200529321722815644549