Abstract
Despite the remarkable advances in revascularization strategies made during the last decade, a significant proportion of patients are excluded from either percutaneous coronary intervention or coronary artery bypass grafting because of unsuitable coronary anatomy. Diffuse severe coronary artery disease, small vessel caliber, chronic total occlusions, or extremely calcified vessels are frequent reasons for deferring revascularization with either percutaneous coronary intervention or coronary artery bypass grafting. We present a case concerning a middle-aged asymptomatic patient who was treated successfully with percutaneous coronary intervention due to a chronic total occlusion lesion of the left anterior descending artery. Coronary angiography is an inadequate method for the estimation of the burden of atherosclerotic disease in an artery fed by collaterals. Assessment of any residual antegrade flow, and ipsilateral and contralateral collateral filling of the segments distal to the occlusion with invasive or noninvasive techniques, could affect the appropriate decision-making by physicians.
Introduction
Diffuse severe coronary artery disease, small vessel caliber, chronic total occlusions, or extremely calcified vessels are frequent reasons for deferring revascularization with either percutaneous coronary intervention or coronary artery bypass grafting.Citation1 Presumably, estimation of such angiographic characteristics in a culprit vessel with a proximal total occlusion is feasible only through a well developed collateral network. There is general agreement that optimal medical treatment is the cornerstone of coronary artery disease management. Meanwhile, there is no doubt that timely revascularization offers a benefit in controlling patients with severe symptoms and may also offer a survival benefit in patients with diffuse disease and diabetes.Citation2 Known techniques and innovations are crucial if old, calcified, and long chronic total occlusions are to be recanalized, proceeding with percutaneous coronary intervention. On the other hand, coronary artery bypass grafting is the basic alternative for treatment of diffusely diseased vessels not amendable to percutaneous coronary intervention. We present a case concerning a middle-aged asymptomatic patient who was treated successfully with percutaneous coronary intervention due to a chronic total occlusion lesion of the left anterior descending artery, despite initial misleading angiographic images.
Case report
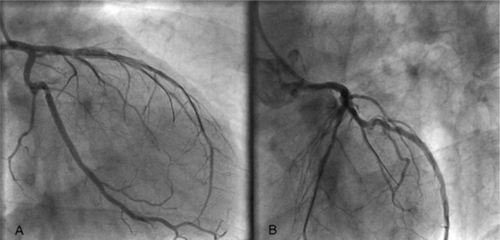
An asymptomatic 47-year-old male patient with a strong family history of coronary artery disease was admitted for coronary angiography due to a positive exercise stress test followed by a thallium scan which showed extensive ischemia of the anterior left ventricular wall. An echocardiogram revealed mild apical left ventricular hypokinesia with preserved global left ventricular ejection fraction. Coronary angiography showed a chronic total occlusion of the proximal part of the left anterior descending artery, along with a 40% stenosis of the left circumflex artery, and a normal right coronary artery. Beyond the proximal left anterior descending artery occlusion, the vessel was opacified through ipsilateral () and mostly contralateral collaterals (Rentrop Grade 2),Citation3 and appeared to have diffuse atheroma with at least three severe angiographic stenoses extending to its distal part (). This angiographic anatomy suggested that if percutaneous coronary intervention was selected as the initial therapeutic strategy, following a presumably successful treatment of the chronic total occlusion, multiple stents would be needed to restore full vessel patency. On the other hand, revascularization with coronary artery bypass grafting would require an extensive endarterectomy distal to the implantation of an arterial graft. Therefore, an attempt at percutaneous coronary intervention with a plan for referral for coronary artery bypass grafting if the former was unsuccessful was decided. Surprisingly, following successful stenting of the proximal left anterior descending artery occlusion with a paclitaxel-eluting stent, it became evident that, distal to the latter, the vessel had diffuse atherosclerosis, but without any other significant angiographic stenosis as the initial angiography had suggested (). The patient had an uneventful recovery and was discharged after three days. Follow-up at six months with an exercise treadmill test showed no electrocardiographic signs of ischemia and an excellent exercise tolerance.
Figure 1 A) Right anterior oblique caudal view of left anterior descending artery. Total proximal occlusion of left anterior descending artery (white arrow). Arrowheads indicate mild ipsilateral collaterals from the obtuse marginal to the left anterior descending artery. B) Straight right anterior oblique view of right coronary artery. Contralateral collaterals from the right coronary artery are feeding the distal part of the left anterior descending artery (white arrow), giving the impression of a narrow and multi-atheromatous vessel. Arrowheads show severe and diffuse atheroma in the left anterior descending artery. (Image courtesy of the Catheterization Laboratory at Patras University Hospital).
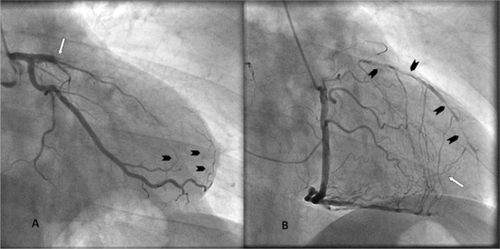
Figure 2 Right anterior oblique caudal (Panel A) and left anterior oblique; cranial (Panel B) projection of left anterior descending artery. After stent apposition, left anterior descending artery appears as a diffusely atheromatous vessel without critical stenosis. One more guide wire was used in order to protect the diagonal branch. (Image courtesy of the Catheterization Laboratory at Patras University Hospital).
Discussion
More than 30% of patients with significant coronary artery disease present with chronic total occlusions.Citation4 In such patients, the existence of a collateral circulation supplying the myocardium distal to a severe stenosis or total occlusion may improve ventricular function, minimize the infarcted area, reduce the incidence of left ventricular aneurysm formation, and lead to improved survival compared with patients lacking a well developed collateral network.Citation5 Additionally, the existence of the latter allows angiographic assessment of the involved vessel beyond the level of the chronic total occlusion. The extent of collateral flow is not always adequately estimated by coronary angiography, because there is a capacity for further dilatation in response to neurohumoral mediators.Citation6 There are controversial opinions and results in the literature concerning the proper treatment of severe but asymptomatic coronary artery disease.Citation7 Conversely, recanalization of chronic total occlusions, especially when the left anterior descending artery is involved, with percutaneous coronary intervention can reduce mortality and the need for bypass surgery,Citation8 and even improve symptoms and prognosis.Citation9 If coronary artery bypass grafting is selected as the initial therapeutic strategy, optimal visualization of the target vessel in its entire length through feeding collaterals is mandatory for deciding the feasibility of the former, but the surgeon should also construct a plan for the site of graft implantation, and the potential need for downstream endarterectomy. Obviously, close collaboration between cardiologists and surgeons is needed to balance the feasibility and risks of surgery versus percutaneous coronary intervention for cases in which the angiographic anatomy of the target vessel constitutes the critical point upon which the joint therapeutic decision is based.
Coronary blood flow depends on the balance between coronary artery perfusion pressure and flow resistance in the coronary tree. The main limitation of coronary angiography is that collateral flow detection provides only an estimate of the absolute collateral flow. A momentarily altered balance between vasodilatation and vasoconstriction in the infarct-related artery could affect and could be affected by the flow through collaterals, potentially leading to a false angiographic estimation of lumen characteristics. Antegrade flow and flow through collaterals are constantly under an active balance. There are at least two possible explanations for the observed discrepancy between the angiographic assessment of coronary collateral vessels and rest or stress myocardial perfusion. First, coronary angiography depicts only those epicardial collateral channels with a lumen diameter >100 μm,Citation10 but the most numerous and probably most important subendocardial and intramural intercoronary channels,Citation11 about 20 μm in diameter,Citation12 are not visualized. Second, the development and visualization of collateral vessels depend, at least in part, on the transanastomotic pressure, and could have an additional effect on angiographic visualization of the main vessel, which remains frequently a major channel supporting myocardium perfusion distally to the blockage of the artery.Citation13
Because angiography in this situation may be proved unreliable, noninvasive imaging techniques that may assist better image guidance during chronic total occlusion revascularization, such as computed tomography angiography and invasive high fidelity intracoronary imaging with optical coherence tomography, might be useful for studying the lumen of the target vessel and guiding therapy.Citation14
Conclusion
In conclusion, the degree of distal vessel filling, not only via collateral circulation, and the resulting angiographic estimation of lumen characteristics, may affect medical and surgical decisions potentially impacting on the outcome for the patient, especially when the left anterior descending artery is involved. Hence, our case exemplifies that even reasonable opacification of the target vessel through collaterals, may be misleading for the construction of a surgical plan, and most importantly, for final decision-making.
Disclosure
The authors report no conflicts of interest in this work.
References
- IvanhoeRJWeintraubWSDouglasJSJrPercutaneous transluminal coronary angioplasty of chronic total occlusions. Primary success, restenosis, and long-term clinical follow-upCirculation1992851061151728439
- MagroMGargSSerruysPWRevascularization treatment of stable coronary artery diseaseExpert Opin Pharmacother20111219521221226632
- RentropKPCohenMBlankeHPhillipsRAChanges in collateral channel filling immediately after controlled coronary artery occlusion by an angioplasty balloon in human subjectsJ Am Coll Cardiol198555875923156171
- DelacretazEMeierBTherapeutic strategy with total coronary artery occlusionsAm J Cardiol1997791851879193021
- HabibGBHeibigJFormanSAInfluence of coronary collateral vessels on myocardial infarct size in humans. Results of phase I thrombolysis in myocardial infarction (TIMI) trial. The TIMI InvestigatorsCirculation1991837397461900223
- KomaruTKanatsukaHShiratoKCoronary microcirculation: Physiology and pharmacologyPharmacol Ther20008621726110882810
- GershlickTThomasMPCI or CABG: Which patients and at what costHeart2007931188119017890695
- JoyalDAfilaloJRinfretSEffectiveness of recanalization of chronic total occlusions: A systematic review and meta-analysisAm Heart J201016017918720598990
- LeungWHLauCPEffects of severity of the residual stenosis of the infarct-related coronary artery on left ventricular dilation and function after acute myocardial infarctionJ Am Coll Cardiol1992203073131634665
- GensiniGGBruto da CostaBCThe coronary collateral circulation in living manAm J Cardiol1969243934005805200
- GreggDEPattersonREFunctional importance of the coronary collateralsN Engl J Med1980303140414067432386
- Di CarliMShermanTKhannaSMyocardial viability in asynergic regions subtended by occluded coronary arteries: Relation to the status of collateral flow in patients with chronic coronary artery diseaseJ Am Coll Cardiol1994238608688106690
- TraupeTGloeklerSde MarchiSWernerGSeilerCAssessment of the human coronary collateral circulationCirculation20101221210122020855668
- CourtneyBMunceNAndersonKInnovations in imaging for chronic total occlusions: A glimpse into the future of angiography’s blind-spotEur Heart J20082958359318238930