
Abstract
Purpose
Left ventricular (LV) mechanics by speckle-tracking echocardiography (STE) is prognostic in patients with cardiovascular diseases, but evidence related to community-dwelling individuals is uncertain. We therefore performed a systematic review and meta-analysis of STE as a predictor of adverse outcomes in the general population.
Methods
PRISMA guidelines were followed and MEDLINE and EMBASE were searched to identify eligible studies. Primary outcome was all-cause mortality and secondary outcomes were composite cardiac and cardiovascular end-point. Random effects meta-analysis was performed, and a modified Newcastle-Ottawa Assessment Scale was used for quality assessment.
Results
Eight papers matched the predefined criteria (total number of individuals studied=11,744). All publications assessed global longitudinal strain (GLS) by two-dimensional speckle-tracking echocardiography (2D-STE), one assessed circumferential, radial and transverse strains, and one assessed GLS-derived post-systolic shortening. None assessed LV rotational measures in association with outcomes. Two studies reported associations between GLS and all-cause mortality and composite cardiovascular end-point. Six papers reported an association between GLS and composite cardiac end-point, three of which were from the same study. Four papers were suitable for meta-analysis. GLS predicted all-cause mortality (pooled minimally adjusted HR per unit strain (%)=1.07 [95% CI 1.03–1.11], p=0.001), and composite cardiovascular (pooled maximally adjusted HR=1.18 [1.09–1.28], p<0.0001) and cardiac (HR=1.08 [1.02–1.14], p=0.006) end-points. GLS also predicted coronary heart disease (HR=1.15 [1.03–1.29], p=0.017) and heart failure (HR=1.07 [1.02–1.13], p=0.012). The quality of all studies was good.
Conclusions
This study provides some evidence that STE may have utility as a measure of cardiac function and risk in the general population. 2D-STE-based GLS predicts total mortality, major adverse cardiac and cardiovascular end-points in community-dwelling individuals in a limited number of studies. Despite this, this systematic review also highlights important knowledge gaps in the current literature and further evidence is needed regarding the prognostic value of LV mechanics in unselected older populations.
Registration number: CRD42018090302.
Introduction
Left ventricular systolic dysfunction (LVSD), measured as a reduction in left ventricular (LV) ejection fraction (LVEF), is prognostic of adverse outcomes, including all-cause mortality and heart failure (HF) in the general population.Citation1 Nevertheless, LVEF has well-recognized limitations and LVSD may occur when LVEF is normal.Citation2
Speckle-tracking echocardiography (STE) is a comparatively new tool that quantifies myocardial mechanics,Citation3 and may detect LVSD when LVEF is still preserved.Citation2 Alterations in STE-derived LV strain are associated with risk factors for cardiovascular disease (CVD), including diabetes mellitus (DM),Citation4 hypertensionCitation5 and obesity,Citation6 and lower global longitudinal strain (GLS) predicts unfavorable outcomes in aortic stenosis, HF and hypertrophic cardiomyopathy.Citation7–Citation10
While systematic reviews and meta-analyses of STE-based LV strain as a predictor of adverse outcomes have previously been conducted based on studies of patients with establishedCitation11,Citation12 or established plus suspected CVD,Citation13 a systemic review has not been performed for community-dwelling individuals, who were not selected on the basis of disease or clinical status. This is important, since selecting samples based on disease status can distort associations between risk factors and outcomes – termed index event bias (collider bias).Citation14 Also, community-dwelling individuals are at lower risk of CVD compared with selected diseased populations, and the utility of STE in this setting is uncertain but potentially of value.
We therefore conducted a systematic review and meta-analysis to examine whether STE is associated with risk of total and cardiovascular mortality and morbidity independent of conventional risk factors in community-dwelling individuals (ie, in the general population).
Materials and methods
This systematic review and meta-analysis was conducted according to a previously published protocolCitation15 and conforms to the PRISMA guidance.Citation16 The protocol was registered with the PROSPERO database (CRD42018090302).
Eligibility criteria
All longitudinal studies (including placebo arms of population-based clinical trials) that assessed the prospective association of any STE-derived parameter with at least one of the pre-specified outcomes in community-dwelling individuals (>18 years), who were not selected on the basis of disease or clinical status were eligible. Studies were included if they were reported in English, published in peer-reviewed journals and adhered to appropriate ethical standards. Abstracts, reviews, conference proceedings or letters to the editor were excluded.
Outcomes
The primary outcome was all-cause mortality. Secondary outcomes were 1) a composite cardiac end-point, including any combination of cardiovascular mortality, coronary heart disease (CHD) events (myocardial infarction, unstable angina, angina/ischemia requiring emergent hospitalization or revascularization), HF hospitalization, new-onset atrial fibrillation (AF), life-threatening arrhythmia, recorded automatic implantable cardioverter defibrillator shocks, or 2) composite cardiovascular end-points, including a composite cardiac end-point and stroke, transient-ischemic attacks or peripheral arterial disease with arterial revascularization procedure. Any individual secondary end-points included in composite cardiac or cardiovascular end-points were considered as tertiary outcomes.
Search strategy
Literature was searched in MEDLINE and EMBASE via OvidSP interface. Search strategies are shown in the Supplementary materials and data to be extracted were predefined.Citation15 The last search was carried out on February 28, 2018. Additional papers could be identified by searching the reference lists of relevant articles and their citation metrics using Web of Science Core Collection.
Study selection and data extraction
Search results from each database were combined and duplicates were removed before screening. Initial title and abstract screening were performed and full texts of selected articles were retrieved and double screened for eligibility using a predefined eligibility form,Citation15 and data extracted using a predefined form.Citation15 Screening and extraction was performed by two researchers working independently (L.A. and C.P.). Discrepancies were reviewed and resolved through consensus.
Quality assessment
A modified version of the Newcastle-Ottawa Quality Assessment Scale of cohort studiesCitation17 was used to assess the quality of included papers.Citation15 The total quality score was reported as the average of the two researchers’ scores ranging from 0 (lowest quality score) to 7 (highest quality score). Papers were included irrespective of the quality assessment score.
Statistical methods
All analyses were performed using Stata 15.1 (StataCorp LLC, USA). We used random effects meta-analysis to pool effect estimates and calculated the 95% CIs of the relevant HRs based on the expectation of heterogeneity between different studies. All HRs were rescaled to per unit strain (%). Results were presented graphically as forest plots and heterogeneity was assessed using Higgins Thompson I2 test and Cochran’s Q test.Citation15
We planned to carry out a meta-analysis on a minimally adjusted model (ie, age, sex and ethnicity [if relevant]) and a maximally adjusted model, including cardiovascular risk factors and conventional echocardiographic measures. Meta-analyses were only possible for GLS. Endocardial strain was used for primary analyses, but we performed sensitivity analysis by repeating analyses replacing endocardial with midwall or epicardial strains when available.
We planned to assess potential sources of heterogeneity,Citation15 but were unable to perform any subgroup analysis or meta-regression due to the limited number of identified studies per analysis. Similarly, it proved impossible to compare different software for STE analysis due to lack of relevant data.
Results
Search results and study selection
A PRISMA diagram is shown in . A total of 7040 records were identified. After removing duplicates, 6222 records of 6235 were excluded by title and abstract. Thirteen full text articles were assessed for eligibility. Five did not meet the inclusion criteria (n=1: ineligible outcome;Citation18 n=4: same cohort, deemed not population representative due to selection criteriaCitation19–Citation22), the other eight papers from five studies were eligible (n=2 from Cardiovascular Abnormalities and Brain Lesion study,Citation23,Citation24 n=3 from Copenhagen City Heart StudyCitation25–Citation27, and n=1 from Framingham Offspring Study and Framingham Omni Study,Citation28 Flemish Study on Environment, Genes and Health Outcomes [FLEMENGHO],Citation29 and Atherosclerosis Risk in Communities Citation30).
Figure 1 PRISMA flow diagram illustrates different stages of this systematic review.
Characteristics of included papers
Characteristics of included papers are shown in (additional information regarding the studies is included in Table S1). Most (4/8) were based on US samples (two papers from the same study).Citation23,Citation24,Citation28,Citation30 The remainder included one paper from BelgiumCitation29 and three papers (from the same study) from Denmark.Citation25–Citation27 The total number of participants was 11,744, participants in the five studies reported in the eight identified papers ranged between 675 and 6118. Follow-up ranged between 608 days (469–761) (median; IQR)Citation30 and 12.5 years (9.4–12.8).Citation27 One study recruited participants free of CVD at baseline,Citation28 while others included participants with known CVD.
Table 1 Brief characteristics of included studies
Exposures and outcomes of included papers
Exposures and outcomes from included papers are shown in . All used two-dimensional speckle-tracking echocardiography (2D-STE). Two used Philips QLAB 8.1, two used TomTec CPA and four used EchoPac. All studies (n=8) assessed GLS. One study also assessed circumferential, radial and transverse strainsCitation28 and another assessed GLS-derived post-systolic shortening measures.Citation26 None assessed LV rotational measures in association with the chosen outcomes. All papers except oneCitation27 provided data on exposure reliability (intra-observer,Citation29,Citation30 inter-observerCitation24 reproducibility or bothCitation23,Citation25,Citation26,Citation28).
Table 2 Exposure and outcome characteristics of the included papers
GLS and all-cause mortality
Two studies found associations between 2D-STE-derived measures and all-cause mortality .Citation26,Citation28 GLS was reported in both studies; however, only oneCitation28 provided both minimally and maximally adjusted estimates. Consequently, meta-analysis was only performed on the two minimally adjusted estimates; pooled HR=1.07 (1.03–1.11), p=0.001 ().
Figure 2 GLS as a predictor of all-cause mortality (A), composite cardiac end-point (B) and cardiovascular end-point (C). All-cause mortality HR estimates are from minimally adjusted (Cheng et al) and unadjusted (Brainin et al) models. Composite cardiovascular and cardiac end-points are based on maximally adjusted models (listed in the Supplementary materials). For Kuznetsova et al, endocardial-wall strain is shown. Hazard ratios are per unit change in strain value. The heterogeneity assessment including the I2 statistics and p-value of Q test is shown.

Table 3 Results of studies assessed the association between two-dimensional speckle-tracking echocardiographic-derived measures and all-cause mortality, composite cardiovascular and cardiac end-points
GLS and composite cardiovascular end-point
Two studies reported associations between GLS and a composite cardiovascular end-point, but neither provided a minimally adjusted estimate ().Citation23,Citation29 Random effect meta-analysis indicated that lower 2D-STE-based GLS was associated with higher risk of a composite cardiovascular end-point; pooled maximally adjusted HR=1.18 (1.09–1.28), p<0.0001 (). Substituting mid-wall or epicardial-wall strains for endocardial strain did not alter this finding (Figure S1).
GLS and composite cardiac end-point
Among six papers which assessed different 2D-STE-derived measures,Citation25–Citation30 only GLS or a GLS-derived measure (post-systolic index) was associated with a composite cardiac end-point (). Three of these papers were from the same study population;Citation25–Citation27 one study was not suitable for quantitative synthesis because the estimates provided combined GLS and LVEF, and were available only for a selected high-risk subset of the population (stage A and B HF);Citation30 therefore, data from three papersCitation25,Citation28,Citation29 were used for meta-analysis. Low GLS predicted higher HR of a composite cardiac end-point; pooled maximally adjusted HR=1.08 (1.02–1.14), p=0.006 (). A sensitivity analysis showed that replacing the endocardial with mid- or epicardial-wall strainsCitation29 had minimal effect (Figure S3). Analysis of minimally adjusted estimates is shown in Figure S2.
GLS and tertiary outcomes
Four papers provided data on GLS in association with tertiary outcomes,Citation24,Citation25,Citation28,Citation29 one of which assessed circumferential, radial and transverse strainsCitation28 (). Three papers reported CHD,Citation25,Citation28,Citation29 two HF,Citation25,Citation28 one AFCitation24 and one cardiovascular death.Citation25 GLS was associated with CHD, AF and HF, whereas circumferential strain was only associated with HF although this was assessed in only one study (). Meta-analysis showed that GLS was a predictor of CHD and HF (CHD maximally adjusted HR=1.15 [1.03–1.29], p=0.017; HF HR=1.07 [1.01–1.13], p=0.012; ). Meta-analysis based on minimally adjusted estimates is shown in Figure S4, and further sensitivity analysis was performed for CHD replacing the endocardial with mid- or epicardial-wall strains and results were hardly altered (Figure S5). Additional information from studies that reported Kaplan–Meier data related to various outcomes is shown in Table S1.
Figure 3 GLS as a predictor of coronary heart disease (A) and heart failure (B) on maximally adjusted models (listed in the Supplementary materials). For Kuznetsova et al, endocardial-strain is shown. Hazard ratios are per unit change in strain value. The heterogeneity assessment including the I2 statistics and p-value of Q test is shown.
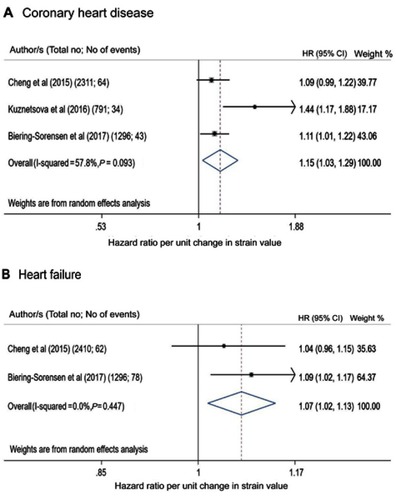
Table 4 Results of studies assessed the association between two-dimensional speckle-tracking echocardiographic-derived measures and tertiary outcomes
Publication bias and study quality
Assessment of publication bias was not possible due to the small number of identified studies. The quality of the studies was good. Seven scored a maximum 7Citation23–Citation26,Citation28–Citation30 and one scored 6Citation27 (Table S2). The degree of heterogeneity indicated by I-square was small in most of the meta-analyses and was only large in two analyses.
Discussion
This systematic review and meta-analysis summarizes current evidence about the prognostic value of STE-derived measures in the general population. 2D-STE-derived GLS was the most studied measure and it predicted total mortality, major adverse cardiac and cardiovascular end-points in community-dwelling individuals in a limited number of studies that included a total of 11,744 participants. Although information on potential confounders was limited and inconsistent, there was some evidence that this was independent of conventional cardiovascular risk factors and other echocardiographic measures. There was insufficient evidence in relation to other myocardial deformation indices or 3D-STE-derived indices to draw conclusions with respect to outcomes. Therefore, this systematic review also highlights important knowledge gaps in the current literature regarding the possible utility of myocardial deformation indices in unselected older populations, and further evidence is still required, particularly regarding 3D-STE.
Risk assessment and management of patients with CVD are guided by the measurement of LV global systolic function.Citation2 LVEF is considered the cornerstone in assessing LV systolic function,Citation1 but LV strain imaging is attracting interest as an additional tool to improve risk assessment and guide management in diseased populations.Citation2,Citation12 Nevertheless, the evidence on the utility of STE as a measure of cardiac function and risk in community-dwelling individuals has been limited. We provide a synthesis of current evidence that provides some support for GLS as a useful risk measure but also highlights the need for more information regarding the utility of STE for risk assessment and diagnosis. Based on limited numbers of identified studies, GLS was a prognostic marker of cardiovascular mortality and morbidity independent of conventional risk factors. This is important because risk factors which potentially lead to CVDs such as aging, hypertension and DM are common characteristics of longitudinal population-based samples of elderlyCitation23–Citation30 and are known to be associated with alterations in GLS even when LVEF is still normal.Citation4,Citation5,Citation31,Citation32
According to the disease progression, the layers of the myocardium as well as the various other contributors to cardiac mechanics can be affected differently.Citation33 Disease affecting the subendocardial layer such as ischemia, hypertension or DM tends to impair longitudinal mechanics, while circumferential and twist mechanics remain preserved or even enhanced to preserve the overall LV systolic performance and LVEF.Citation33,Citation34 With more involvement of the mid-myocardial and subepicardial layers, both circumferential and twist mechanics will deteriorate leading to a reduction in LVEF.Citation3,Citation33 In unselected population without overt cardiac diseases, Russo et al characterized the relationship between multidirectional myocardial mechanics with radial thickening and LVEF.Citation35 Radial strain was more influenced by circumferential strain than longitudinal strain explaining why radial thickening, and hence LVEF, is less sensitive than longitudinal function in detecting subclinical LVSD.Citation35 This may contribute to the added prognostic value of GLS over LVEF especially when LVEF is still normal or mildly impaired.Citation12
STE-based LV strain imaging allows comprehensive quantification of complex myocardial mechanics. While STE is increasingly used in clinical practice, it suffers from inherent technical limitations.Citation31 High-quality images and adequate frame rates are crucial for accurate tracking. For 2D-STE, multiple views are required which is time-consuming to apply in large population-based studies. Indeed, among identified studies,Citation23–Citation30 only one study measured circumferential, radial and transverse strains,Citation28 while none measured LV rotation.Citation26 This could be due to analysis time required or the limited feasibility and reproducibility of these measurements. Nevertheless, circumferential strain, both MRI-basedCitation36 and 2D-STE based,Citation28 was an independent prognostic marker for incident HF over and beyond traditional risk factors and conventional measures in subjects free of CVDs of community-dwelling individuals. Further, Cheng et al have suggested that distinct components of LV mechanics (ie, GLS, circumferential strain, etc.) are differently associated with individual CVD outcomes,Citation28 but it was not possible to answer this question due to the limited number of studies. In the future, 3D imaging methods may overcome some of the limitations of 2D-STE and provide additional insight to the different relationship between individual components of LV mechanics and CVD outcomes.
Study limitations
A number of limitations of this study ought to be acknowledged. This systematic review was limited to English language publications, which may have introduced a selection bias. We identified only eight papers based on five different studies; all identified studies used 2D-STE and no study examined additive the prognostic value of 3D-STE-derived LV deformation indices in a general population. Once multiple publications from the same study were accounted for, meta-analyses were based on either two or three studies limiting the precision of estimates of between-study variance which could result in an underestimate of the width of the confidence intervals. Further, meta-analysis should be performed when results of at least ten relevant studies are available. The small number of studies also precluded sub-group analysis and meta-regression to explore sources of heterogeneity between studies. We assumed a priori that there would be heterogeneity between the various observational studies and consequently used random effects modeling, although there was not strong evidence of heterogeneity in the identified studies. Since estimates from random effects models behave like the fixed effect estimate as heterogeneity decreases, it is not likely that this will have introduced substantial error. The small number of studies also prevented us from employing formal assessment of publication bias (e.g. funnel plots), but this bias cannot be excluded. Analyses employed different vendor-specific software and possibly different software versions; both are factors which may introduce systematic differences between studies. For this reason, GLS analysis including LV segmentation is different between studies included in this meta-analysis (e.g. endocardial analysis of GLS from 12 LV-segments,Citation28 transmural analysis of GLS from 18 LV-segmentsCitation25 or GLS from only 6 LV-segmentsCitation29). However, since we examined associations with outcomes in relation to a continuous exposure (GLS) the impact of this source of heterogeneity is likely to be small, consistent with our sensitivity analysis.
Conclusion
This study synthesized current evidence regarding STE-derived measures as prognostic indicators of mortality and cardiovascular events in community-dwelling individuals. Despite limited number of studies in this meta-analysis, LV GLS by 2D-STE showed prognostic value in this population and may add to conventional cardiovascular risk factors and other echocardiographic measures. However, our findings also highlight the limitations of the existing evidence base and identify important knowledge gaps in the current literature regarding the possible utility of myocardial deformation indices and 3D-STE in unselected older populations – these are issues where further evidence is needed.
Abbreviation list
AF, atrial fibrillation; CHD, coronary heart disease; CVD, cardiovascular disease; DM, diabetes mellitus; GLS, global longitudinal strain; HF, heart failure; LV, left ventricular; LVEF, left ventricular ejection fraction; LVSD, left ventricular systolic dysfunction; MI, myocardial infarction; STE, speckle-tracking echocardiography.
Acknowledgments
LA is supported by a scholarship grant from Imam Abdulrahman Bin Faisal University for her postgraduate studies (PhD) at UCL. AH works in a unit that receives support from the UK Medical Research Council (Programme Code MC_UU_12019/1), he also receives support from the British Heart Foundation (PG/15/75/31748, CS/15/6/31468, CS/13/1/30327), and the National Institute for Health Research University College London Hospitals Biomedical Research Centre. CP receives support from the British Heart Foundation (CS/15/6/31468). RH is supported by the UK Medical Research Council (MC_UU_12019/2).
Disclosure
This work was presented at the British Society of Echocardiography 2018 as a presentation with interim findings. Professor Alun Hughes reports grants from British Heart Foundation, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
- Wang TJ, Evans JC, Benjamin EJ, Levy D, LeRoy EC, Vasan RS. Natural history of asymptomatic left ventricular systolic dysfunction in the community. Circulation. 2003;108(8):977–982. doi:10.1161/01.CIR.0000085166.44904.7912912813
- Potter E, Marwick TH. Assessment of left ventricular function by echocardiography: the case for routinely adding global longitudinal strain to ejection fraction. JACC Cardiovasc Imaging. 2018;11(2 Pt 1):260–274.29413646
- Mor-Avi V, Lang RM, Badano LP, et al. Current and evolving echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/EAE consensus statement on methodology and indications endorsed by the Japanese society of echocardiography. J Am Soc Echocardiogr. 2011;24(3):277–313. doi:10.1016/j.echo.2011.01.01521338865
- Jensen MT, Sogaard P, Andersen HU, et al. Global longitudinal strain is not impaired in type 1 diabetes patients without albuminuria: the Thousand & 1 study. JACC Cardiovasc Imaging. 2015;8(4):400–410. doi:10.1016/j.jcmg.2014.12.02025746329
- Narayanan A, Aurigemma GP, Chinali M, Hill JC, Meyer TE, Tighe DA. Cardiac mechanics in mild hypertensive heart disease: a speckle-strain imaging study. Circ Cardiovasc Imaging. 2009;2(5):382–390. doi:10.1161/CIRCIMAGING.108.81162019808626
- Wong CY, O’Moore-Sullivan T, Leano R, Byrne N, Beller E, Marwick TH. Alterations of left ventricular myocardial characteristics associated with obesity. Circulation. 2004;110(19):3081–3087. doi:10.1161/01.CIR.0000147184.13872.0F15520317
- Cho GY, Marwick TH, Kim HS, Kim MK, Hong KS, Oh DJ. Global 2-dimensional strain as a new prognosticator in patients with heart failure. J Am Coll Cardiol. 2009;54(7):618–624. doi:10.1016/j.jacc.2009.04.06119660692
- Hung CL, Verma A, Uno H, et al. Longitudinal and circumferential strain rate, left ventricular remodeling, and prognosis after myocardial infarction. J Am Coll Cardiol. 2010;56(22):1812–1822. doi:10.1016/j.jacc.2010.06.04421087709
- Yingchoncharoen T, Gibby C, Rodriguez LL, Grimm RA, Marwick TH. Association of myocardial deformation with outcome in asymptomatic aortic stenosis with normal ejection fraction. Circ Cardiovasc Imaging. 2012;5(6):719–725. doi:10.1161/CIRCIMAGING.112.97734823008423
- Liu H, Pozios I, Haileselassie B, et al. Role of global longitudinal strain in predicting outcomes in hypertrophic cardiomyopathy. Am J Cardiol. 2017;120(4):670–675. doi:10.1016/j.amjcard.2017.05.03928687124
- Shetye A, Nazir SA, Squire IB, McCann GP. Global myocardial strain assessment by different imaging modalities to predict outcomes after ST-elevation myocardial infarction: A systematic review. World J Cardiol. 2015;7(12):948–960. doi:10.4330/wjc.v7.i12.94826730301
- Kalam K, Otahal P, Marwick TH. Prognostic implications of global LV dysfunction: a systematic review and meta-analysis of global longitudinal strain and ejection fraction. Heart. 2014;100(21):1673–1680. doi:10.1136/heartjnl-2013-30447424860005
- Stanton T, Leano R, Marwick TH. Prediction of all-cause mortality from global longitudinal speckle strain: comparison with ejection fraction and wall motion scoring. Circ Cardiovasc Imaging. 2009;2(5):356–364. doi:10.1161/CIRCIMAGING.109.86233419808623
- Dahabreh IJ, Kent DM. Index event bias as an explanation for the paradoxes of recurrence risk research. JAMA. 2011;305(8):822–823. doi:10.1001/jama.2011.16321343582
- Al Saikhan L, Park C, Hardy R, Hughes A. Prognostic implications of left ventricular strain by speckle-tracking echocardiography in population-based studies: a systematic review protocol of the published literature. BMJ Open. 2018;8. doi:10.1136/bmjopen-2018-023346
- Shamseer L, Moher D, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015;350:g7647. doi:10.1136/bmj.g764725555855
- Wells G, Shea B, O’Connell D, et al. The Newcastle-Ottawa scale (NOS) for assessing the quailty of nonrandomised studies in meta-analyses Available from: http://www.ohri_ca/programs/clinical_epidemiology/oxford.asp. Accessed July 8, 2019.
- Russo C, Jin Z, Homma S, et al. Subclinical left ventricular dysfunction and silent cerebrovascular disease: the Cardiovascular Abnormalities and Brain Lesions (CABL) study. Circulation. 2013;128(10):1105–1111. doi:10.1161/CIRCULATIONAHA.113.00198423902759
- Yang H, Negishi K, Wang Y, Nolan M, Saito M, Marwick TH. Echocardiographic screening for non-ischaemic stage B heart failure in the community. Eur J Heart Fail. 2016;18(11):1331–1339. doi:10.1002/ejhf.2016.18.issue-1127813300
- Yang H, Marwick TH, Wang Y, et al. Association between electrocardiographic and echocardiographic markers of stage B heart failure and cardiovascular outcome. ESC Heart Fail. 2017;4(4):417–431. doi:10.1002/ehf2.1215129154431
- Yang H, Negishi K, Wang Y, Nolan M, Marwick TH. Imaging-guided cardioprotective treatment in a community elderly population of stage B heart failure. JACC Cardiovasc Imaging. 2017;10(3):217–226. doi:10.1016/j.jcmg.2016.11.01528279368
- Wang Y, Yang H, Nolan M, Pathan F, Negishi K, Marwick TH. Variations in subclinical left ventricular dysfunction, functional capacity, and clinical outcomes in different heart failure aetiologies. ESC Heart Fail. 2018;05:05.
- Russo C, Jin Z, Elkind MS, et al. Prevalence and prognostic value of subclinical left ventricular systolic dysfunction by global longitudinal strain in a community-based cohort. Eur J Heart Fail. 2014;16(12):1301–1309. doi:10.1002/ejhf.4625211239
- Russo C, Jin Z, Sera F, et al. Left ventricular systolic dysfunction by longitudinal strain is an independent predictor of incident atrial fibrillation: a community-based cohort study. Circ Cardiovasc Imaging. 2015;8(8):e003520. doi:10.1161/CIRCIMAGING.115.00352026253626
- Biering-Sorensen T, Biering-Sorensen SR, Olsen FJ, et al. Global longitudinal strain by echocardiography predicts long-term risk of cardiovascular morbidity and mortality in a low-risk general population: the copenhagen city heart study. Circ Cardiovasc Imaging. 2017;10(3). doi:10.1161/CIRCIMAGING.116.005521
- Brainin P, Biering-Sorensen SR, Mogelvang R, Sogaard P, Jensen JS, Biering-Sorensen T. Postsystolic shortening by speckle tracking echocardiography is an independent predictor of cardiovascular events and mortality in the general population. J Am Heart Assoc. 2018;7(6). doi:10.1161/JAHA.118.008528
- Modin D, Biering-Sorensen SR, Mogelvang R, Landler N, Jensen JS, Biering-Sorensen T. Prognostic value of echocardiography in hypertensive versus nonhypertensive participants from the general population. Hypertension. 2018;71(4):742–751. doi:10.1161/HYPERTENSIONAHA.117.1067429483222
- Cheng S, McCabe EL, Larson MG, et al. Distinct aspects of left ventricular mechanical function are differentially associated with cardiovascular outcomes and all-cause mortality in the community. J Am Heart Assoc. 2015;4(10):e002071. doi:10.1161/JAHA.115.00207126508740
- Kuznetsova T, Cauwenberghs N, Knez J, et al. Additive prognostic value of left ventricular systolic dysfunction in a population-based cohort. Circ Cardiovasc Imaging. 2016;9(7). doi:10.1161/CIRCIMAGING.116.004661
- Shah AM, Claggett B, Loehr LR, et al. Heart failure stages among older adults in the community: the atherosclerosis risk in communities study. Circulation. 2017;135(3):224–240. doi:10.1161/CIRCULATIONAHA.117.02730527881564
- Collier P, Phelan D, Klein AA. Test in context: myocardial strain measured by speckle-tracking echocardiography. J Am Coll Cardiol. 2017;69(8):1043–1056. doi:10.1016/j.jacc.2016.11.02628231932
- Kuznetsova T, Herbots L, Richart T, et al. Left ventricular strain and strain rate in a general population. Eur Heart J. 2008;29(16):2014–2023. doi:10.1093/eurheartj/ehn28018583396
- Sengupta PP, Tajik AJ, Chandrasekaran K, Khandheria BK. Twist mechanics of the left ventricle. JACC Cardiovasc Imaging. 2008;1(3):366–376.19356451
- Seo Y, Ishizu T, Atsumi A, Kawamura R, Aonuma K. Three-dimensional speckle tracking echocardiography. Circ J. 2014;78(6):1290–1301. doi:10.1253/circj.CJ-14-036024770358
- Russo C, Jin Z, Homma S, et al. Relationship of multidirectional myocardial strain with radial thickening and ejection fraction and impact of left ventricular hypertrophy: a study in a community-based cohort. Echocardiography. 2013;30(7):794–802. doi:10.1111/echo.1213423360509
- Choi EY, Rosen BD, Fernandes VR, et al. Prognostic value of myocardial circumferential strain for incident heart failure and cardiovascular events in asymptomatic individuals: the multi-ethnic study of atherosclerosis. Eur Heart J. 2013;34(30):2354–2361. doi:10.1093/eurheartj/eht13323644181