Abstract
Background
Patients with type 2 diabetes (T2DM) are at risk of long-term vascular complications. In trials, exenatide once weekly (ExQW), a GLP-1R agonist, improved glycemia, weight, blood pressure (BP), and lipids in patients with T2DM. We simulated potential effects of ExQW on vascular complications, survival, and medical costs over 20 years versus standard therapies.
Patients and methods
The Archimedes model was used to assess outcomes for ~25,000 virtual patients with T2DM (NHANES 1999–2006 [metformin ± sulfonylureas, age 57 years, body mass index 33 kg/m2, weight 94 kg, duration T2DM 9 years, hemoglobin A1c [A1C] 8.1%]). The effects of three treatment strategies were modeled and compared to moderate-adherence insulin therapy: advancement to high-adherence insulin at A1C ≥ 8% (treat to target A1C < 7%) and addition of pioglitazone (PIO) or ExQW from simulation start. ExQW effects on A1C, weight, BP, and lipids were modeled from clinical trial data. Costs, inflated to represent 2010 $US, were derived from Medicare data, Drugstore.com, and publications. As ExQW was investigational, we omitted ExQW, PIO, and insulin pharmacy costs.
Results
By year 1, ExQW treatment decreased A1C (~1.5%), weight (~2 kg), and systolic BP (~5 mmHg). PIO and high-adherence insulin decreased A1C by ~1%, increased weight, and did not affect systolic BP. After 20 years, A1C was ~7% with all strategies. ExQW decreased rates of cardiovascular and microvascular complications more than PIO or high-adherence insulin versus moderate-adherence insulin. Over 20 years, ExQW treatment resulted in increased quality-adjusted life-years (QALYs) of ~0.3 years/person and cost savings of $469/life-year versus moderate adherence insulin. For PIO or high-adherence insulin, QALYs were virtually unchanged, and costs/life-year versus moderate-adherence insulin increased by $69 and $87, respectively.
Conclusions
This long-term simulation demonstrated that ExQW treatment may decrease rates of cardiovascular and some microvascular complications of T2DM. Increased QALYs, and decreased costs were also projected.
Background
The incidence of diabetes and associated health problems continues to increase in the United States.Citation1,Citation2 In 2010, approximately 25.6 million adults, or 11.3% of the adult (age ≥ 20 years) population in the United States had some form of diabetes, diagnosed or otherwise; 90% to 95% of the cases were type 2 diabetes mellitus (T2DM).Citation3 These patients are at long-term risk of cardiovascular events such as coronary heart disease (CHD), myocardial infarction (MI), and stroke and of microvascular complications such as renal disease, retinal disease potentially leading to blindness, and lower extremity ulcerations that may result in amputation.Citation3
Despite clear guidelines to help correct and maintain good glycemic controlCitation4,Citation5 and a wide variety of antihyperglycemic therapies, most patients with diabetes have difficulty achieving glycemic targets.Citation6 Diabetes is commonly accompanied by several comorbidities such as obesity, dyslipidemia, and hypertension that also contribute to cardiovascular disease (CVD).Citation7,Citation8 Patients with T2DM are two to four times more likely to experience cardiovascular disease than those without T2DM.Citation3 Approximately two-thirds of patients with diabetes have elevated blood pressure (BP ≥140/90), which also contributes to CVD.Citation3 Ideally, a diabetes therapy should alleviate the symptoms of diabetes, reduce the risk of diabetes complications, and reduce associated morbidity, mortality, and costs.
Exenatide, the first antihyperglycemic agent in the glucagon- like peptide-1 (GLP-1) receptor agonist class, improves glycemic controlCitation9,Citation10 by enhancing glucose-dependent secretion of insulin, suppressing appetite, inhibiting postprandial glucagon secretion, and slowing gastric emptying. Citation10,Citation11 The twice-daily formulation (ExBID) is currently used to improve glycemic control in patients with T2DM. A once-weekly formulation (ExQW) is currently approved in the European Union and in the United States. In clinical studies, ExQW treatment resulted in reductions in hemoglobin A1c (A1C) and weight as well as in cardiovascular risk factors such as BP and lipids in patients with T2DM.Citation12–Citation15
In the absence of long-term data on the effects of ExQW, we used the Archimedes model to assess the potential effects of ExQW, pioglitazone (PIO), and high-adherence insulin compared to moderate-adherence insulin on the incidence of cardiovascular and microvascular outcomes, on life-years, and on costs over 20 years in a cohort of patients with T2DM derived from the National Health and Nutrition Examination Survey (NHANES) 1999–2006.
Patients and methods
Description of Archimedes model
The Archimedes model simulates human physiology, disease progression, and health care delivery using an integrated model to describe the interactions of diseases, disease complications, various treatments, and health care guidelines as well as measures of quality of life and cost.Citation16–Citation19 Using differential equations maintains the continuous nature of biological variables, time, and their interactions. Diseases, and their respective treatments, are modeled at the clinical level. The model includes the effects of diabetes and other diseases, and incorporates patient and provider behaviors, office visits and hospital admissions, tests and treatments, care delivery protocols, performance and compliance, utilization, and costs. The model has been validated against a number of major clinical trials, including trials of diabetes management and treatment.Citation16–Citation19
Description of simulation strategies
We designed simulation strategies to follow four hypothetical cohorts of patients with T2DM on background metformin ± sulfonylureas (SFU): (1) moderate-adherence insulin, (2) high-adherence insulin, and initiation at simulation start of (3) PIO or (4) ExQW. All strategies treated to a target A1C of 7%, but insulin was not initiated until A1C reached 8%. All strategies were identical with respect to general patient care guidelines and treatment goals, and concomitant diabetes treatments. Finally, all strategies maintained metformin therapy throughout the course of the 20-year simulation, and terminated SFU treatment when insulin was initiated. Adherence to insulin was set to 76% in the moderate-adherence insulin strategy,Citation20,Citation21 and to 100% in the high-adherence insulin strategy, to be more competitive with PIO and ExQW. Based on queries of the IMS Health database for PIO and ExBID, we assumed that 14% of patients treated with PIO and 21% of patients treated with ExQW would remain on therapy after insulin was initiated.
The simulation population was derived from NHANES 1999–2006Citation22 and was reflective of patients with T2DM who had an A1C of 7%–11%, were 18–80 years old, were currently taking metformin with or without concomitant SFU, did not use insulin, and did not have end-stage renal disease. The simulation was run for 20 years with results reported annually; results at 5, 10, and 20 years are reported here.
Outcomes
The primary outcome of the four simulation strategies was their effect on prevention or delay of long-term cardiovascular disease and other diabetic complications. We also directly examined the impact on short-term (1-year) biomarker changes (eg, A1C, BP, lipids, weight) for each treatment strategy to ensure that data from the simulated and actual clinical trial populations were not substantially different. Cardiovascular disease outcomes included major adverse cardiovascular events (MACE- a composite measure including MI, stroke, and CHD death), and individual measures of MI, stroke, CHD death, and congestive heart failure (CHF). Microvascular complications of diabetes included macroalbuminuria, end-stage renal disease (ESRD), macular edema, blindness, foot ulcer, and lower extremity amputation. All-cause death was also assessed.
Other outcomes included life-years (LYs), quality-adjusted LYs (QALYs), direct medical costs, and numbers needed-to-treat (NNT). The cost of health outcomes included the medical costs of hospital admissions, doctors’ visits, procedures, medications other than study medications, and tests. Inpatient, outpatient, ambulatory, and treatment costs were based primarily on Medicare charges. All costs were inflated to represent 2010 US dollars. Cost effectiveness was calculated using standard methods.Citation23 Since ExQW was investigational at the time of this analysis, the costs of insulin, PIO, and ExQW treatments were not included in the calculations and we conducted a cost consequence analysis. QALYs were calculated as the sum of time spent in various health states, discounted by disutility scores associated with the state’s corresponding conditions.Citation24 The model scanned each (virtual) patient’s medical record and applied disutility discounts associated with specific diagnoses. NNT was computed as in Altman et al.Citation25
ExQW model
The ExQW model was constructed using data from four phase III clinical trials of ExQW treatment. Data from DURATION-1 (104 weeks),Citation14 DURATION-2 (52 weeks),Citation15 DURATION-3 (26 weeks),Citation12 and DURATION-5 (26 weeks)Citation13 were used to quantify the effect of ExQW on A1C, weight, BP, total cholesterol (TC), and triglycerides (TG). Data points from the trials for a given variable (eg, weight) were pooled, and the locally-weighted scatterplot smoothing (LOESS) technique was used to fit contours to the resulting aggregation, modeling the change from baseline as a function of time and baseline value.Citation26 In the absence of long-term clinical trial data at the time of data analysis, no further change in effect was modeled for ExQW after 2 years, although the simulation included changes resulting from natural biomarker drift (eg, the effect of aging) and changes due to background patient care. Additionally, no direct effects on disease progression were modeled, just the effect of treatment on A1C, weight, BP, TC, and TG. For initial biomarkers values at normal levels, we assumed no effect of ExQW. Only ExQW was newly modeled for this work; models for PIO and insulin were already included in the Archimedes model.Citation18
Results
Demographics, biomarker trajectories, and medication use
The simulated population was derived from NHANES in order to create a sample representative of patients meeting the inclusion criteria (18–80 years old, T2DM, A1C 7%–11%, currently using metformin ± SFU, not yet taking insulin). Generally, patients in the simulation were similar to those in the ExQW trials, differing by <1 standard deviation ().
Table 1 Baseline characteristics of the simulation and DURATION trials populations
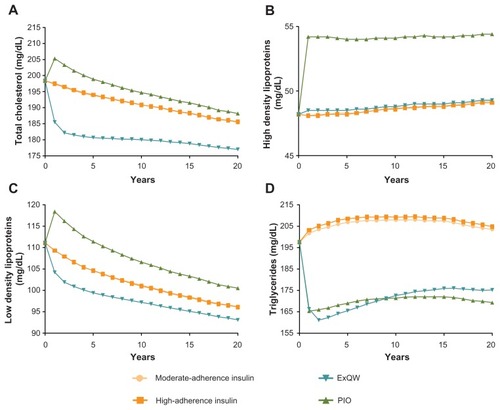
An initial assessment of biomarkers after 1 year of simulated treatment for all strategies showed results that were in line with expectations. A1C decreased by ~1% in PIO-and high-adherence insulin-treated patients and decreased by ~1.5% in ExQW-treated patients. Patients treated with both insulin strategies and PIO experienced modest initial increases in weight while ExQW-treated patients experienced a reduction in weight of ~2 kg. In the PIO and high-adherence insulin strategies there was little change in systolic BP (SBP), while the ExQW strategy decreased SBP by ~5 mmHg. Changes in lipid profiles were observed primarily in PIO- and ExQW-treated patients. In PIO-treated patients, TG decreased by 16.3% and TC, high-density lipoproteins (HDL), and low-density lipoproteins (LDL) increased by 3.4%, 12.4%, and 6.5%, respectively. In ExQW-treated patients, decreases of 6.5%, 15.8%, and 6.2% were observed in TC, TG, and LDL, respectively; HDL did not change.
At the end of the 20-year simulation, A1C was ~7% for all three treatment strategies, which was an expected outcome given the treat-to-target aspect of the simulations (). After changes in the first year, weight gradually decreased and SBP gradually increased with all treatment strategies due to the natural progression of aging (). After initial changes, LDL gradually decreased in all treatment strategies; HDL and TG remained fairly constant. Total cholesterol also gradually declined in all treatment strategies over the simulation period, with the greatest decrease after 20 years seen in EQW-treated patients ().
Figure 1 Changes in A1C (A), weight (B), and systolic blood pressure (C) over 20 years of simulated treatment with high-adherence insulin, PIO, and ExQW versus moderate-adherence insulin.
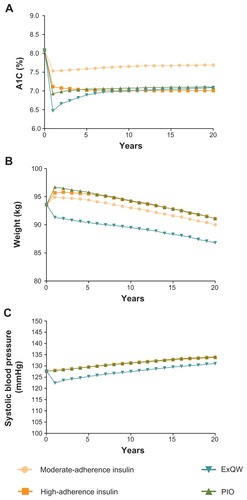
Figure 2 Changes in total cholesterol (A), high- (B) and low-density (C) lipoproteins, and triglycerides (D) over 20 years of simulated treatment with high-adherence insulin, PIO, and ExQW versus moderate-adherence insulin.
As the simulation progressed, patients’ use of insulin and other background medications changed based on the level of control for a given biomarker. In all strategies, as patients reached an A1C of 8%, insulin treatment was initiated. By the end of the 20-year simulation, 55%, 82%, 29%, and 21% of patients in the moderate-adherence insulin, high-adherence insulin, PIO, and ExQW arms, respectively, had initiated insulin use. The marked drop in the percentage of patients transitioning to insulin observed in the PIO and ExQW arms provided an indication of the effect of these agents on glycemic control. The percentage of patients using antihypertensive agents and statins increased over time for all treatment strategies (~20% to 22% antihypertensives, ~18% to 25% statins), but the increase in patients using these medications was slightly lower in ExQW-treated patients (~20% antihypertensives, ~18% statins). The decreased use of antihypertensives in ExQW-treated patients was due to the decrease in SBP. Statin use also mirrored the effect of treatments on LDL, increasing in PIO-treated patients and decreasing slightly in ExQW-treated patients relative to the insulin arms.
Effect on health outcomes
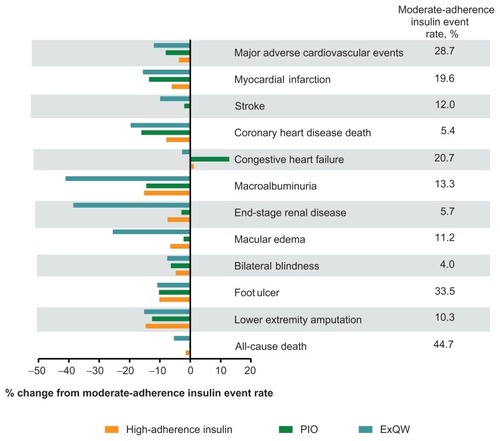
The effect of the four strategies on biomarkers translated to beneficial changes in overall long-term clinical health outcomes in the model. The event rates for MACE, components of MACE, and microvascular complications commonly associated with diabetes generally decreased for the three treatment arms relative to moderate-adherence insulin (). For most health outcomes, ExQW decreased the event rate to a greater degree than did PIO and high-adherence insulin by virtue of its greater effect on A1C, weight, BP, and lipids. All-cause death decreased for all treatments compared to moderate-adherence insulin, but was statistically significant only for patients treated with ExQW (). These decreases were pronounced at 20 years and most were seen as early as 5 and 10 years.
Figure 3 Changes relative to moderate-adherence insulin in Kaplan-Meier event rates of cardiovascular and microvascular complications of diabetes after 20 years of simulated treatment with high-adherence insulin, PIO, and ExQW.
Abbreviations: ExQW, exenatide once weekly; PIO, pioglitazone.
Effects on LYs, QALYs, and costs
At 5, 10, and 20 years, ExQW was associated with increased LYs and lower direct medical costs than moderate-adherence insulin, high-adherence insulin, and PIO strategies. Costs calculated did not include the cost of the treatments insulin, PIO, and ExQW. These differences resulted in an average cost/LY benefit of over $400 ($409–$469) relative to control ().
Table 2 Total life-years and costs (undiscounted) per initial person for high-adherence insulin, PIO, and ExQW vs moderate-adherence insulin after 5, 10, and 20 years of treatment
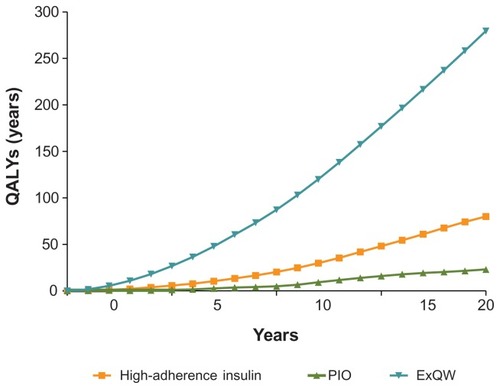
ExQW increased QALYs more than all other treatments, an effect that was observed at 5 years and continued to 20 years. After 20 years of treatment, QALYs were 13.72, 13.52, 13.46, and 13.44 per initial person for ExQW, high-adherence insulin, PIO and moderate-adherence insulin, respectively. Over 20 years, these changes translated into increases in QALYs for ExQW-treated patients of ~3 months versus moderate-adherence insulin and PIO, and of ~2.4 months versus high-adherence insulin ().
Figure 4 QALYs (undiscounted) saved versus moderate-adherence insulin per 1000 simulated patients.
Numbers needed-to-treat (NNTs)
ExQW required substantially fewer patients to be treated to avoid a single event than the high-adherence insulin and PIO strategies relative to moderate-adherence insulin ().
Table 3 Numbers needed-to-treat versus moderate-adherence insulin to avoid a single cardiovascular event
Discussion
Modeling of health and economic outcomes allows an estimation of potential effects of new treatments with insufficient long-term data. This simulation provided evidence for the effectiveness of ExQW compared with insulin or PIO for preventing the cardiovascular complications, microvascular complications, and death associated with diabetes over 20 years of treatment.
Biomarkers such as A1C, weight, blood pressure, and lipids are associated with poor long-term cardiovascular health if not kept within normal ranges. Clinical trial data have shown that ExQW decreases these biomarkers, but the data are short-term and limited to controlled clinical trial settings. Our simulation indicated that the effect of ExQW on improved glycemic control and cardiovascular biomarkers was associated with reduced cardiovascular event rates over 20 years. However, we note that the existence of a clinically-significant and positive relationship between glycemic control and cardiovascular event rates has been variable in a number of prospective trials.Citation27,Citation28 The MACE composite event rate, including MI, stroke, and CHD death, decreased with all treatments compared with moderate-adherence insulin, but patients treated with ExQW achieved the lowest rates.
All treatments in the simulation improved glycemic control but, as with cardiovascular risk factors, after 20 years, ExQW treatment reduced the risk of microvascular complications more than did high-adherence insulin or PIO. By design, all patients in the model were treated to target (A1C = 7%), and all strategies reduced the microvascular complications of diabetes. Many of these microvascular complications are also subject to the effects of weight and blood pressure. For example, macroalbuminuria, a precursor of serious renal complications, is affected by glycemic control as well as blood pressure.Citation29,Citation30 ExQW reduced macroalbuminuria by ~40%, while high-adherence insulin and PIO reduced macroalbuminuria event rates by ~16 and 15%, respectively. Development of two earlier-stage retinal complications of diabetes, proliferative diabetic retinopathy (PDR, data not shown) and macular edema, is governed to a large extent by glycemic control and blood pressure.Citation29,Citation30 The event rates of PDR and macular edema were decreased more in patients treated with ExQW than in patients treated with PIO and high-adherence insulin. However, the treatment strategies had only a small and similar effect on the very late stage complication of total blindness. Lower extremity amputation, driven by A1C, was similar across all therapies compared with moderate-adherence insulin (~15% reduction), since all therapies treated to an A1C target of 7%. Finally, treatment with ExQW had a small, but significant, improvement over treatment with PIO or high-adherence insulin in reducing all-cause death.
The improvements in health outcomes had substantial economic benefits. After 20 years of treatment, QALYs increased and total medical costs decreased for patients treated with ExQW compared to all other strategies. These improvements with ExQW treatment were observed after 5 years and increased as the simulation progressed. Cost savings were also observed with PIO treatment at 5 and 10 years, but were markedly less than for ExQW, and the savings disappeared entirely by simulation end.
Limitations and assumptions
These findings were based on a mathematical model and as such were subject to the assumptions used to create it. The ExQW model was derived from four clinical trials, each with limited data, and assumed that the effects of ExQW treatment would remain constant after year 2, that ExQW treatment would continue indefinitely unless advancement to insulin occurred, and that there were no adverse effects associated with ExQW treatment. The adverse effects that were modeled included hypoglycemia for insulin and SFU treatment and CHF for PIO treatment, both well-documented for the respective treatments. Patients were assumed to be 100% compliant to insulin, PIO, and ExQW in the high-adherence insulin, PIO, and ExQW treatment strategies, respectively, a less than realistic scenario. However, effects for more realistic compliance levels can be estimated by interpolating results between the moderate-adherence insulin and the other treatment arms. The simulation model did include the cost of treatment for diseases/ conditions such as high blood pressure and high cholesterol; it did not include any treatment costs for insulin, PIO, and ExQW. Finally, the impact of known or suspected biomarkers for cardiovascular and microvascular complications such as measures of inflammation, oxidation, or fat-derived cytokines and the effects of each of the glucose-lowering agents on these markers were not included in the model.
Conclusion
The simulation of ExQW treatment in patients with T2DM for 20 years indicates that the treatment may decrease the complications associated with the morbidity and mortality of T2DM, including MACE and many microvascular complications. ExQW treatment was also associated with a decrease in the cost of management of diabetes and its complications and an increase in QALYs. Simulations using ExQW data gathered beyond 2 years and incorporating adverse event data will further refine these observations. Validation through long-term trials such as the Exenatide Study of Cardiovascular Event Lowering (EXSCEL) trial (NCT01144338) is also needed.
Acknowledgment
We wish to acknowledge Susan Strobel, PhD of SciComm LLC for assistance with manuscript preparation (funded by Amylin Pharmaceuticals, Inc).
Disclosure
Julia A. Gaebler, Amy Blickensderfer, Matthew Wintle, David Maggs, Jenny Han, and Richard Pencek were employees and shareholders of Amylin Pharmaceuticals, Inc. at the time this study was conducted. Gerardo Soto-Campos, Peter Alperin, Marc Cohen, and Barbara Peskin received research support from Amylin Pharmaceuticals, Inc.; at the time this study was conducted, all were employees of Archimedes Inc. Byron Hoogwerf is an employee of Eli Lilly and Company.
References
- Center for Disease Control and PreventionDiabetes data and trends: national surveillance data – number (in millions) of civilian, non-institutionalized adults with diagnosed diabetes, United States, 1980–2009c2011 [updated March 30, 2011]. Available from: http://www.cdc.gov/diabetes/statistics/prev/national/figadults.htmAccessed November 13, 2011
- Center for Disease Control and PreventionDiabetes data and trends: national surveillance data – diabetes complicationsc2011 [updated June 16, 2011]. Available from: http://www.cdc.gov/diabetes/statistics/complications_national.htmAccessed November 13, 2011
- Centers for Disease Control and PreventionNational diabetes fact sheet: national estimates and general information on diabetes and prediabetes in the United States, 2011c2011 [Updated November 8, 2011]. Available from: http://www.cdc.gov/diabetes/pubs/factsheet11.htmAccessed November 13, 2011
- NathanDMBuseJBDavidsonMBMedical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of DiabetesDiabetes Care20093219320318945920
- RodbardHWJellingerPSDavidsonJAStatement by an American Association of Clinical Endocrinologists/American College of Endocrinology consensus panel on type 2 diabetes mellitus: an algorithm for glycemic controlEndocr Pract20091554055919858063
- KoroCEBowlinSJBourgeoisNFedderDOGlycemic control from 1988 to 2000 among U.S. adults diagnosed with type 2 diabetes: a preliminary reportDiabetes Care200427172014693960
- BuseJBGinsbergHNBakrisGLPrimary prevention of cardiovascular diseases in people with diabetes mellitus: a scientific statement from the American Heart Association and the American Diabetes AssociationCirculation200711511412617192512
- American Diabetes AssociationStandards of medical care in diabetes – 2011Diabetes Care201134Suppl 1S11S6121193625
- EngJKleinmanWASinghLSinghGRaufmanJPIsolation and characterization of exendin-4, an exendin-3 analogue from Heloderma suspectum venomJ Biol Chem1992267740274051313797
- BYETTA® (exenatide) injection. Full prescribing informationc2010 [Revised September 2010; Amylin Pharmaceuticals Inc, San Diego, CA] Available from: http://pi.lilly.com/us/byetta-pi.pdfAccessed August 20, 2011
- KimWEganJMThe role of incretins in glucose homeostasis and diabetes treatmentPharmacol Rev20086047051219074620
- DiamantMVan GaalLStranksSOnce weekly exenatide compared with insulin glargine titrated to target in patients with type 2 diabetes (DURATION-3): an open-label randomised trialLancet20103752234224320609969
- BlevinsTPullmanJMalloyJDURATION-5: Exenatide once weekly resulted in greater improvements in glycemic control compared to exenatide twice daily in patients with type 2 diabetesJ Clin Endocrinol Metab2011961301131021307137
- TaylorKGurneyKHanJPencekRWalshBTrautmannMExenatide once weekly treatment maintained improvements in glycemic control and weight loss over 2 yearsBMC Endocr Disord201111921529363
- WyshamCBergenstalRMalloyJDURATION-2: efficacy and safety of switching from maximum daily sitagliptin or pioglitazone to once-weekly exenatideDiabet Med20112870571421434995
- EddyDSchlessingerLValidation of the Archimedes diabetes modelDiabetes Care2003263102311014578246
- EddyDMSchlessingerLKahnRClinical outcomes and cost-effectiveness of strategies for managing people at high risk for diabetesAnn Intern Med200514325126416103469
- AlperinPSoto-CamposGPeskinBUnderstanding the effect of glycemic control on macrovascular outcomes in patients with diabetes using the Archimedes Model [abstract]Diabetes201059 Abstract 879-P
- KahnRAlperinPEddyDAge at initiation and frequency of screening to detect type 2 diabetes: a cost-effectiveness analysisLancet20103751365137420356621
- BrownJBNicholsGAGlauberHSBakstATen-year follow-up of antidiabetic drug use, nonadherence, and mortality in a defined population with type 2 diabetes mellitusClin Ther1999211045105710440626
- CramerJAPughMJThe influence of insulin use on glycemic controlDiabetes Care200528788315616237
- Centers for Disease Control and PreventionNational Health and Nutrition Examination Survey (NHANES)c2011 Available from: http://www.cdc.gov/nchs/nhanes.htmAccessed June 23, 2011
- GoldMRSiegelJERussellLBWeinsteinMCCost- Effectiveness in Health and MedicineNew York, NYOxford University Press1996
- SullivanPWGhushchyanVPreference-based EQ-5D index scores for chronic conditions in the United StatesMed Decis Making20062641042016855129
- AltmanDGAndersenPKCalculating the number needed to treat for trials where the outcome is time to an eventBMJ19993191492149510582940
- ClevelandWSGrosseEShyuMJLocal regression modelsChambersJMHastieTStatistical Models in SNew York, NYChapman and Hall1992309376
- HolmanRRPaulSKBethelMAMatthewsDRNeilHA10-year follow-up of intensive glucose control in type 2 diabetesN Engl J Med20083591577158918784090
- SkylerJSBergenstalRBonowROfor American Diabetes Association, American College of Cardiology Foundation, and American Heart AssociationIntensive glycemic control and the prevention of cardiovascular events: implications of the ACCORD, ADVANCE, and VA diabetes trials: a position statement of the American Diabetes Association and a scientific statement of the American College of Cardiology Foundation and the American Heart AssociationDiabetes Care20093218719219092168
- UK Prospective Diabetes Study (UKPDS) GroupIntensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33)Lancet19983528378539742976
- UK Prospective Diabetes Study GroupTight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38BMJ19983177037139732337