Abstract
Background
Diabetes represents one of the major health challenges in Switzerland, and early diagnosis and treatment is mandatory to prevent or delay diabetes-related morbidity and mortality. For the purpose of identifying affected individuals, early screening in pharmacies is a valuable option. In this survey, we aimed to determine blood glucose and metabolic control in an unselected population of individuals visiting Swiss pharmacies.
Methods
The subjects responded to a short questionnaire and underwent a single capillary blood glucose test for screening purposes. They were classified as normal, indeterminate, impaired fasting glucose, and diabetes according to predefined blood glucose levels.
Results
A total of 3135 individuals (mean age 56 years) in 18 cantons were screened in November 2010; of these, 4.2% (95% confidence interval [CI] 3.5–4.9) had previously been diagnosed with diabetes. Diabetes was newly diagnosed in 1.9% (95% CI 1.5–2.4), and 11.5% (95% CI 10.4–12.6) had impaired fasting glucose. Subjects with impaired glucose control had an increased body mass index, a frequent family history of diabetes, hypertension, hypercholesterolemia, smoking, and a low level of physical activity. Prevalence of impaired glucose control was different between the French/Italian-speaking part of Switzerland (new diabetes 4.9%; impaired fasting glucose 12.7%) and the German-speaking part (new diabetes 1.9%; impaired fasting glucose 10.3%).
Conclusion
Our study shows a 6.1% prevalence of diabetes, of which about a third (1.9%) was previously undiagnosed, and 11.5% had impaired fasting glucose. Therefore, screening initiatives in pharmacies may be suitable for detecting people with undiagnosed diabetes.
Keywords:
Introduction
There is an increasing prevalence of type 2 diabetes globally, which is attributable to a growing global population, an increase in life expectancy, increased diagnostic efforts, and a reduced diabetes risk attributable to recent advances in diabetes treatment.Citation1 Therefore, diabetes is a major driver of health care costs.Citation2
For Switzerland, a diabetes prevalence of 3.3% has been reported for 1997 and an increase to 4.8% in the year 2007.Citation3 Other data from a large population-based study conducted in the French part of Switzerland point to an even higher prevalence.Citation4 Therefore, it is not surprising that type 2 diabetes and its complications contribute to 2.2% of Switzerland’s health care expenditure.Citation5
Early diagnosis and treatment is mandatory to prevent or delay diabetes-related morbidity and mortality and reduce health care costs. Within this context, measurement of blood glucose levels during screening initiatives may help to identify persons with unknown diabetes or impaired fasting glucose and to initiate preventative measures or appropriate therapy in a timely manner. Pharmacies are particularly suitable for this purpose, because they are an easily accessible point of contact for individuals not visiting physicians.
Based on these considerations, we conducted a national survey in pharmacies of the AMAVITA chain documenting more than 3000 individuals with respect to their random blood glucose values and further cardiometabolic parameters. Our aim was to assess glucose values, classify observed values into normal, indeterminate, impaired fasting glucose, and definite diabetes, in a largely unselected population of pharmacy attendees.
Materials and methods
Individuals visiting a participating pharmacy in one of 18 cantons of Switzerland were enrolled into the present study. Participants were selected based on their willingness to undergo blood glucose testing and to provide information on their cardiometabolic risk profile, without any further predefined selection criteria. Patients not willing to participate were neither documented nor counted to determine participation rates.
Prior to enrollment, all study participants received a written information leaflet explaining the survey objectives and procedures. The study was conducted in accordance with applicable Swiss national regulations for epidemiologic studies and good epidemiologic practice, and informed verbal consent was obtained. A signed informed consent form was not required, because no personal data were registered and measurement of blood glucose is a standard procedure in Swiss pharmacies.
Documentation
On an anonymized one-page case report form, participants were asked to report the time of their last meal, as well as their gender, age, body weight, and height. The following parameters were also documented: presence or absence of diabetes, antidiabetic treatment, family history of diabetes or, in women, a weight of more than 4 kg of their newborns, a history of cardiovascular events (myocardial infarction, stroke), and cardiovascular risk factors (hypertension, hypercholesterolemia, smoking, physical exercise). Physical exercise was classified as no activity, moderate (at least 30 minutes/day for 5 days/week, eg, walking, dancing, gardening), or strenuous (at least 20 minutes/day on 3 days a week, eg, jogging, swimming, team sports).
Blood glucose classification
Capillary blood glucose was measured in all study participants using a uniform blood glucose monitoring device (Accu-Check® Aviva, Roche, Basel, Switzerland) according to the manufacturer’s instructions. Based on their blood glucose values, study participants were categorized as either fasting (last meal ≥ 8 hours), or nonfasting (last meal < 8 hours), and were further subclassified into four different groups based on their blood glucose levels as follows: normal blood glucose (<5.6 mmol/L for fasting/nonfasting), diabetes status indeterminate (5.6 to <11.1 mmol/L for nonfasting), impaired fasting glucose (5.6–6.9 mmol/L for fasting), and diabetes (≥7 mmol/L for fasting; ≥11.1 mmol/L for nonfasting).
Regional analyses
For the regional analyses, cantons were subdivided into the German-speaking population (SUI-GER) which comprised the cantons Aargau, Bern, Basel-Land, Basel-Stadt, Graubünden, Luzern, St Gallen, Solothurn, Zug, and Zurich, and the French/Italian speaking population (SUI-FR/IT) comprising Fribourg, Geneva, Jura, Neuchâtel, Tessin, Waadtland, and Wallis.
Statistical analysis
We performed a descriptive analysis of the data. For this purpose, only participants with complete data regarding the individual parameters were considered. Continuous variables are shown as the mean ± standard deviation, and categorical variables as percentages. P values for comparison between groups of patients were calculated using the two-sided t-test for quantitative variables and the χ2 test for qualitative variables.
Results
A total of 3135 participants were enrolled by 102 pharmacies in November 2010. The study population comprised 27% males, had a mean age of 56 years and a mean body mass index of 25 kg/m2. Mean random blood glucose was 6.0 ± 1.5 mmol/L, and about one quarter (23.0%) of participants were in a fasting state (). The presence of diabetes was self-reported by 131/3135 participants (4.2%; 95% confidence interval [CI] 3.5–4.9), and the majority of these known diabetic participants (67.2%) were treated with oral antidiabetic drugs alone. A total of 6.1% received an insulin-containing regimen (insulin alone or basal insulin-assisted oral antidiabetic treatment) and 24.4% received diet and exercise alone.
Table 1 Participant characteristics (total n = 3135)
Prevalence of unknown impaired glucose control
Of 3004 participants with previously unknown diabetes, 86.7% had a normal (43.2%) or indeterminate (43.5%) blood glucose status, 11.5% were diagnosed with impaired fasting glucose, and 2.0% had new diabetes. Impaired glucose control was particularly prevalent in older age (P < 0.001), male patients (P = 0.011), and those with a body mass index > 25 kg/m2 (P < 0.001). The prevalence was also higher in participants with risk factors, such as hypertension, hypercholesterolemia, and smoking (P < 0.001, ).
Table 2 Metabolic profile in participants
SUI-GER versus SUI-FR/IT
In the total cohort, the diabetes prevalence was 6.1% (CI 5.3–7.0, ). A total of 1681 participants were from the SUI-GER region, and 1454 participants from the SUI-FR/IT region (). Mean blood glucose levels were similar in both regions of Switzerland. In the SUI-FR/IT region, the participants were younger (P < 0.001) and were more often fasting (P < 0.001), while the prevalence of diabetes was only nominally higher and many participants were treated with oral antidiabetic drugs compared with SUI-GER. Furthermore, participants in SUI-FR/IT had lower blood pressure values (P = 0.046), were more likely to be smokers (P = 0.002), and had a low level of physical activity (P < 0.001, ).
Figure 1 Prevalence of diabetes.
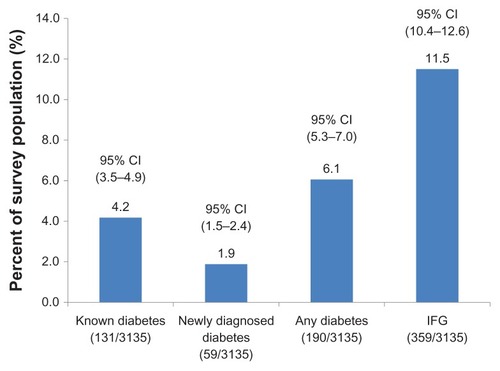
Table 3 Distribution of glucose control by region and canton based on a total survey population of 3135
The regional comparison () showed a lower number of participants with known diabetes in the SUI-FR/IT region (5.0% versus 3.6% in SUI-GER; P = 0.063), whereas no regional difference was seen with regard to newly diagnosed diabetes (1.9% for both).
The frequency of a normal glucose profile varied between 30.7% (Basel-Stadt) and 52.8% (Tessin), whereas impaired fasting glucose was most frequently diagnosed in Geneva (17.2%), but in only 5% of participants in the canton of Jura. The presence of diabetes was most frequently reported in Geneva (8.0%) and least frequently in the canton of Jura (1%). Most cases of new diabetes were detected in the canton of Zug (6.0%), whereas the lowest number of new diabetes cases was seen in the canton of Graubünden (0.5%) and Wallis (1%). Due to low numbers of study participants, the cantons of Schaffhausen, Solothurn, and Waadtland were not considered for this comparison.
Discussion
Our analysis shows a 6.1% prevalence of diabetes in an unselected Swiss population visiting a pharmacy and agreeing to participate in our survey, of which 4.2% had known diabetes and 1.9% were newly detected by capillary blood glucose determination. These data not only confirm a recently published prevalence of 4.8% in a population aged 18 to >65 years (nationwide, population-based telephone survey), but indicate stable prevalence of diabetes from 2007 to 2010 using a similar methodologic approach.Citation3 However, based on the number of newly diagnosed diabetic participants in our survey, it can be assumed that the real diabetes burden in Switzerland is higher than previously reported.
Diabetes prevalence in perspective
According to the International Diabetes Federation, an estimated 629,000 participants (aged 20–79 years) in Switzerland suffer from diabetes, corresponding to a prevalence of 8.9%. These numbers are similar to those in Germany and Austria, but higher than in other northern European countries, such as Belgium, The Netherlands (5.3%), and France (6.7%).Citation6 However, accurate prevalences of diabetes can only be derived from structured, population-based studies. From a methodologic perspective, our investigation does not fullfill all the criteria of a proper population-based study and the willingness to undergo voluntary blood glucose testing might favor the enrollment of the more health-conscious subjects. Nevertheless, participants consulting a pharmacist can be considered as a largely unselected population due to the large age spectrum and the variety of reasons for a pharmacy visit. One population-based study was conducted in the French-speaking region of Switzerland (Lausanne), and reported an overall diabetes prevalence of 6.6% in participants aged 35–75 years, of which only 66.3% were known cases of diabetes.Citation4 Even though the low number of study participants in the canton of Waadtland (Lausanne region) in our study does not allow for any conclusions, the overall prevalence of 6.8% in the SUI-FR/IT region (4.9% with known/1.9% with newly diagnosed diabetes) corresponds well to these published data, mostly driven by the comparatively high number of diabetic participants in the canton of Geneva (9.6% new and known diabetes combined). Interestingly, the overall prevalence for diabetes appears to be lower in the SUI-GER part of Switzerland, especially in the cantons of Bern, Basel-Stadt, and Graubünden, but there was considerable heterogeneity observed between cantons, which remains unexplained.
Diabetes and risk factor control
The recently published Swiss health survey shows self-reported diabetes control rates of 65.5% for the year 2007.Citation3 In line with these findings, data from our survey suggest the presence of uncontrolled diabetes in about 45% of participants with known diabetes (29% with a diabetic profile/15.3% with impaired fasting glucose) based on a single random blood glucose test and where the majority of participants were treated with oral antidiabetic drugs alone. However, these data have to be interpreted with extreme caution, given that a single capillary blood glucose test is not a suitable tool to establish the level of blood glucose control in participants with diabetes, but rather a prescreening tool.Citation7 Further, the total number of diabetic participants was low in our study, which also represents a major limitation for making conclusions on blood glucose control in diabetic participants in Switzerland.
In our study, established cardiometabolic risk factors, such as elevated body mass index, a family history of diabetes, hypertension, hypercholesterolemia, smoking and a low level of physical exercise appeared to be associated with impaired glucose metabolism, confirming well known previous observations in this Swiss population.Citation8–Citation10 Even though the prognostic relevance of treating diabetes and impaired fasting glucose with regards to microvascular and macrovascular complications are undisputed, there is a lack of prospective data supporting the cost-effectiveness of structured screening initiatives.Citation11–Citation13 However, screening allows for early identification of individuals affected by diabetes or at risk of diabetes, and such initiatives, even when conducted at unconventional locations such as optometry practices, have been shown to be useful.Citation14
Diabetes screening
Screening for diabetes in asymptomatic patients has been challenged recentlyCitation15 for having no beneficial effect on overall health outcomes. To our knowledge, there are no randomized, controlled trial data and only one relevant case-control study, and neither showing a benefit when considering microvascular complications. However, there are data to support screening being effective in hypertensive persons when macrovascular benefits are considered. Therefore, targeted screening might be more effective than mass screening.
The most recent guidelines of the American Diabetes Association for screening and diagnosis of diabetes require a glycosylated hemoglobin ≥ 6.5%, a fasting plasma glucose ≥ 126 mg/dL or a 2-hour plasma glucose ≥ 200 mg/dL, or symptoms of hyperglycemia in patients with a random plasma glucose ≥ 200 mg/dL.Citation16 Fasting is defined as no caloric intake for at least 8 hours. Just as there is less than 100% concordance between fasting plasma glucose and 2-hour plasma glucose tests, there is not full concordance between glycosylated hemoglobin and either glucose-based test. Analyses of National Health and Nutrition Examination Survey data indicate that, assuming universal screening of the undiagnosed, the glycosylated hemoglobin cut point ≥ 6.5% identifies one-third fewer cases of undiagnosed diabetes than a fasting glucose cut point ≥ 126 mg/dL (7.0 mmol/L).Citation16
In the clinical as well as in the research environment, the required fasting status is a challenging task. For clinicians and patients it is much simpler to obtain random glucose values irrespective of the fasting duration. In studies, especially epidemiologic ones, the fasting requirement influences the study design, complicates the field work, and increases the costs of the study. Moreover, and most important, it is not feasible to control reliably for self-reported fasting status. Therefore, random blood glucose values have been used as a type of prescreening measure to identify individuals in which a repeat testing under fasting conditions is necessary.Citation7,Citation17 For the results of the present study, this means that a number of patients (ie, those with indeterminate blood glucose) may be either normal or have impaired fasting glucose or diabetes. The conclusion is that the prevalence rates reported in our survey for new diabetes are a conservative estimate of the true prevalence.
Limitations
Despite the straightforward approach of testing patients for the presence for dysglycemia in a large number of pharmacies in Switzerland, a number of limitations have to be considered when assessing the results of this study. A confirmation of the results of random blood glucose monitoring in largely nonfasting subjects in the same subjects after 8 hours of fasting or by assessing glycosylated hemoglobin, as suggested by the recent American Diabetes Association recommendation, would have been useful, but was not possible for logistic reasons. We obtained no data on subjects who did not participate in the study, so we cannot rule out the possibility that males, for example, who comprised 27% of the study population, were not visiting pharmacies because of having to work. Finally, the population visiting pharmacies may not be totally representative of the overall population, or may have been affected by common cold, for example, which may introduce bias into blood glucose determination.
Conclusion
In our survey, a total of 59 participants were identified with newly diagnosed diabetes by 102 pharmacies. Given that there are about 1700 retail pharmacies in Switzerland, such an initiative may contribute to identification of a substantial number of participants with unknown diabetes. This would enable early treatment and prevention of diabetes and/or diabetes-related complications.
Disclosure
The present study was conducted as a collaboration between Sanofi Aventis Switzerland and the AMAVITA pharmacy chain. At the time of this survey, AR and MT were employees of Sanofi Aventis, Switzerland. PB has received honoraria for lectures and consulting fees from a number of companies producing antidiabetic drugs, including Sanofi Aventis, Bristol Myers Squibb, AstraZeneca, and Takeda. CAM and RF report no conflicts of interest with respect to the current manuscript. The study was supported by Sanofi-Aventis, Meyrin, Switzerland.
References
- WildSRoglicGGreenASicreeRKingHGlobal prevalence of diabetes: estimates for the year 2000 and projections for 2030Diabetes Care20042751047105315111519
- HermanWThe economics of diabetes preventionMed Clin North Am201195237338421281839
- EstoppeyDPaccaudFVollenweiderPMarques-VidalPTrends in self-reported prevalence and management of hypertension, hypercholesterolemia and diabetes in Swiss adults, 1997–2007BMC Public Health20111111421332996
- FirmannMMayorVVidalPMThe CoLaus study: a population-based study to investigate the epidemiology and genetic determinants of cardiovascular risk factors and metabolic syndromeBMC Cardiovasc Disord20088618366642
- Schmitt-KoopmannISchwenkglenksMSpinasGASzucsTDDirect medical costs of type 2 diabetes and its complications in SwitzerlandEur J Public Health20041413915080382
- The International Diabetes Federation Diabetes Atlas Available from: http://www.idf.org/diabetesatlas/mapsAccessed August 29, 2012
- MoebusSGoresLLoschCJockelKHImpact of time since last caloric intake on blood glucose levelsEur J Epidemiol201126971972821822717
- KnightJADiseases and disorders associated with excess body weightAnn Clin Lab Sci201141210712121844568
- Rodriguez-MoranMGuerrero-RomeroFAradillas-GarciaCObesity and family history of diabetes as risk factors of impaired fasting glucose: implications for the early detection of prediabetesPediatr Diabetes201011533133619895410
- SanzCGautierJFHanaireHPhysical exercise for the prevention and treatment of type 2 diabetesDiabetes Metab201036534635120675173
- UK Prospective Diabetes Study (UKPDS) GroupIntensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) GroupLancet199835291318378539742976
- FordESZhaoGLiCPre-diabetes and the risk for cardiovascular disease: a systematic review of the evidenceJ Am Coll Cardiol201055131310131720338491
- NorrisSKansagaraDBougatsosCNygrenPFuRScreening for Type 2 diabetes mellitus: Update of 2003 systematic evidenceReview for the US Preventive Services Task Force Report 08-05116-EF1Rockville (MD)Agency for Healthcare Research and Quality2008
- HowseJHJonesSHunginAPScreening for diabetes in unconventional locations: resource implications and economics of screening in optometry practicesHealth Policy20111022–319319921835490
- NorrisSLKansagaraDBougatsosCFuRScreening adults for type 2 diabetes: a review of the evidence for the US Preventive Services Task ForceAnn Intern Med20081481185586818519931
- American Diabetes ADiagnosis and classification of diabetes mellitusDiabetes Care201235Suppl 1S647122187472
- MoebusSHanischJUNeuhäuserMAidelsburgerPWasemJJöckelKHAssessing the metabolic syndrome according to NCEP ATP III in Germany: feasibility of a two step approach in 1 550 randomly selected primary health care practicesGer Med Sci20064 Doc7 (20061009)