
Abstract
In 1995, the NINDS (National Institute of Neurological Disorders and Stroke) tPA (tissue plasminogen activator) Stroke Study Group published the results of a large multicenter clinical trial demonstrating efficacy of intravenous tPA by revealing a 30% relative risk reduction (absolute risk reduction 11%–15%) compared with placebo at 90 days in the likelihood of having minimal or no disability. Since approval in 1996, tPA remains the only drug treatment for acute ischemic stroke approved by the US Food and Drug Administration. Over the years, an abundance of research and clinical data has supported the safe and efficacious use of intravenous tPA in all eligible patients. Despite such supporting data, it remains substantially underutilized. Challenges to the utilization of tPA include narrow eligibility and treatment windows, risk of symptomatic intracerebral hemorrhage, perceived lack of efficacy in certain high-risk subgroups, and a limited pool of neurological and stroke expertise in the community. With recent US census data suggesting annual stroke incidence will more than double by 2050, better education and consensus among both the medical and lay public are necessary to optimize the use of tPA for all eligible stroke patients. Ongoing and future research should continue to improve upon the efficacy of tPA through more rapid stroke diagnosis and treatment, refinement of advanced neuroimaging and stroke biomarkers, and successful demonstration of alternative means of reperfusion.
Introduction
In 1995, the NINDS (National Institute of Neurological Disorders and Stroke) tPA (tissue plasminogen activator) Stroke Study Group published the results of a large multicenter clinical trial demonstrating efficacy of intravenous (IV) tPA in acute ischemic stroke (AIS).Citation1 With these practice-changing results, tPA was approved by the US Food and Drug Administration (FDA) for the treatment of AIS and endorsed by the guideline committees of the American Heart Association/American Stroke Association (AHA/ASA),Citation2 the American Academy of Neurology (AAN),Citation3 and recently by the American College of Emergency Physicians (ACEP).Citation4
Although an abundance of research and clinical data has supported the findings from the original NINDS trial, tPA in the acute stroke setting remains substantially underutilized.Citation5,Citation6 Stemming from an original series of debates published shortly after tPA approval,Citation7–Citation10 apprehension still exists that risks may outweigh benefits in a large number of stroke patients, violating the code of “primum non nocere (first do no harm).”Citation11 In the United States, tPA remains the only FDA-approved drug treatment for AIS. Therefore, addressing these decades-old controversies continues to hold strong relevance for clinical practice to this day. In this review article, we will highlight many of the debated issues, relevant research, and current perspectives concerning the use of IV tPA for treatment of AIS. The scope of this review will not cover alternative thrombolytics (eg, urokinase and tenecteplase) or intra-arterial administration of tPA. This review will also not address other endovascular therapies unless specifically relevant to the current use of IV tPA.Citation12–Citation14
Seminal clinical trials of IV tPA in stroke
In the early 1990s, a group of investigators began translating preclinical data to the earliest human trials of tPA in AIS to verify dosing, mechanism of action, and safety profile for stroke thrombolysis.Citation15–Citation18 Shortly after these early studies, several large randomized, placebo-controlled, double-blinded trials commenced to determine the safety and efficacy of tPA in AIS ().Citation1,Citation19,Citation20 In 1993, the ATLANTIS (Alteplase Thrombolysis for Acute Noninterventional Therapy in Ischemic Stroke)-A trial was halted due to increased risk of symptomatic intracerebral hemorrhage (sICH) in the 5–6-hour window from stroke onset; unfortunately, interim enrollment fell short of demonstrating any efficacy up to 5 hours.Citation19
Table 1 Early prospective randomized clinical trials of intravenous tPA in acute ischemic stroke
In 1995, the landmark NINDS tPA study results were published (including Parts I and II), establishing efficacy between 0 and 3 hours from stroke onset by revealing a 30% relative risk reduction (absolute risk reduction 11%–15%) compared with placebo at 90 days in the likelihood of having minimal or no disability. Benefit was compared against a significantly increased risk of sICH in the tPA group during the first 36 hours (tPA 6% versus placebo 0.6%); nevertheless, there was no statistically significant difference in overall mortality between the groups (tPA 17% versus placebo 21%; P=0.30).Citation1
A principal criticism of the results focused on the lack of significant improvement in neurological deficits at 24 hours by the outcome of 4 or more point reduction in the National Institutes of Health (NIH) Stroke Scale (NIHSS) (0–42, 0= no deficits).Citation21 However, post hoc analyses revealed that there was a significant neurological improvement at 24 hours if the defined outcome had been a 5 or more point reduction on the NIHSS. That is to say, the efficacy of tPA would have been appreciated with more substantial improvement between the treatment and placebo arms at 24 hours, but the study did not adequately estimate the natural history of recovery at 3 months.Citation22,Citation23
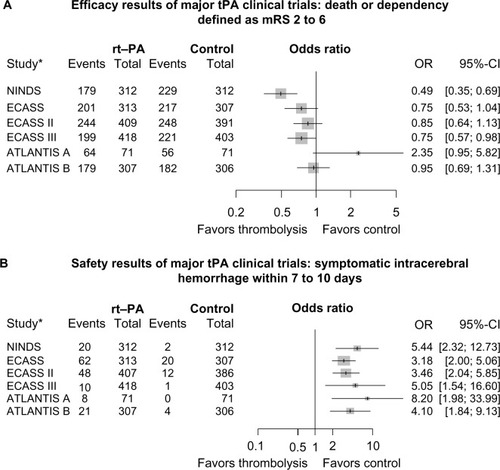
Other large randomized trials were published during that time period yielding conflicting results that revealed no benefit of IV thrombolysis in acute stroke care and increase in risk of hemorrhage.Citation20 Study design and criteria utilized by these studies were different from the NINDS tPA study, such as: use of different thrombolytic agents (eg, streptokinase), time period for treatment (eg, up to 6 hours), and use of increased doses of tPA and/or concomitant antithrombotics.Citation20,Citation24,Citation25 Based on the results of the NINDS study, the ATLANTIS-B and ECASS (European Cooperative Acute Stroke Study) II studies were designed to evaluate the safety and efficacy of tPA within 3–5 hours and up to 6 hours from stroke onset, respectively; both failed to demonstrate primary efficacy.Citation20,Citation26 However, when the same global endpoint analysis used in the NINDS trial was applied to the ECASS I data, a favorable outcome in the tPA-treated group was observed.Citation27 and demonstrate point estimates for odds ratios (ORs) and 95% confidence intervals (CIs) between the tPA and control groups for each of the trials listed in . With the exception of ATLANTIS-A, which had the fewest numbers and least precision, ORs ranged from 0.49 to 0.95 for death or dependency, defined as modified Rankin scale (mRS) 2–6 favoring tPA (). For sICH within 7–10 days, ORs ranged from 3.18 to 8.20, favoring control ().Citation1,Citation19,Citation20,Citation28,Citation29,Citation33,Citation49 These findings are supported by Wardlaw et al,Citation28 who reviewed all randomized trials of any thrombolytic agent versus control conducted from 1966 to 2008. The early clinical trials of IV tPA in AIS supported its efficacy and ultimate FDA-approval for patients presenting within 0–3 hours from onset; an additional common result of these early studies revealed an increased risk of sICH without affecting overall mortality.Citation19,Citation20,Citation26,Citation28,Citation29 In addition, it became evident that two main factors play a vital role in the overall efficacy and risk of hemorrhage: time-to-treatment and adherence to treatment protocol.
Figure 1 (A) Death or dependency defined as mRS 2–6. (B) Risk of symptomatic intracerebral hemorrhage.
Notes: A and B demonstrate point estimates for ORs and 95% CIs between the tPA and control groups for each of the trials. *References for the listed trials: NINDS,Citation1 ECASS,Citation20 ECASS II,Citation29 ATLANTIS-A,Citation19,Citation28 ATLANTIS-B,Citation49 and ECASS III.Citation33
The importance of time-to-treatment
From the practice-changing results of the NINDS study, the precise therapeutic window for tPA in AIS was still debated. Ongoing clinical trials continued to test extended thrombolysis times.Citation30,Citation31 While both ECASS II and ATLANTIS-B failed to show benefit from 3 to 6 hours, with an increased risk of sICH, it was unclear whether there was any benefit within 3–4 hours given low statistical power.Citation20,Citation21,Citation26,Citation29 A pooled analysis of the ATLANTIS, ECASS, and NINDS tPA studies in 2004 suggested a favorable outcome up to 4.5 hours, with an OR of 1.40 (CI 1.05–1.85).Citation32 The results of the pooled analysis prompted the ECASS III study, which was designed to evaluate the efficacy and safety of tPA in AIS between 3 and 4.5 hours. The study applied additional exclusion criteria to comply with the European Medicines Evaluation Agency, including history of diabetes and a prior stroke, age >80 years, and NIHSS >25. The primary results demonstrated a favorable outcome for patients treated with tPA compared with placebo within 4.5 hours of symptom onset (tPA 52.4% versus placebo 45.2%; OR 1.34 [CI 1.02–1.76]; P=0.04).Citation33 Notable differences in ECASS III compared with the NINDS study were a lower enrollment stroke severity in both groups, a higher percentage of the placebo arm with a history of prior stroke, and the additional exclusions limiting generalizability for older patients with more severe strokes. Nonetheless, the AHA/ASA updated guidelines to support the use of tPA in this extended time window for carefully selected patients.Citation34 To date, the use of tPA beyond 3 hours from stroke onset has not been approved for extended labeling by the FDA and remains an off-label indication in the United States.
Early laboratory and clinical pilot studies have alluded to the concept of time-to-treatment as a predictor for a good outcome.Citation1,Citation28,Citation35,Citation36 In the initial NINDS analysis, there was no significant observed difference between the stratification of 0–90 minutes versus 91–180 minutes.Citation1,Citation37 However, further analysis suggested increased odds for early clinical improvement and favorable outcome at 3 months in patients stratified to 0–90 minutes. The pooled analyses by Marler et alCitation38 and Hacke et alCitation32 further demonstrated a direct relationship between time and treatment effect. Saver et alCitation39 in 2006 further elucidated, “time is brain” quantitatively in humans by utilizing magnetic resonance imaging (MRI)-based infarct volumetrics. The author identified that with every passing minute until reperfusion is achieved, about 2 million neurons and 14 billion synapses are lost.Citation39 Most recently, a study of 58,353 tPA-treated patients highlighted that for every 15-minute improvement in time-to-treatment, patients were less likely to die (OR 0.96 [CI 0.95–0.98]; P<0.001), experience sICH (OR 0.96 [CI 0.95–0.98]; P<0.001), and were more likely to be ambulatory at discharge (OR 1.04 [CI 1.03–1.05]; P<0.001).Citation40 This study underscores the importance of innovative models of pre-hospital care to improve the rapidity of treatment.Citation41–Citation43
Based on the most current 2013 AHA/ASA guideline update regarding fibrinolysis in acute stroke, tPA is recommended for eligible patients who present within 3 hours of stroke onset and up to 4.5 hours in eligible patients, with the following additional exclusions: patients >80 years of age, those taking oral anticoagulants regardless of international normalized ratio (INR), baseline NIHSS >25, those with imaging evidence of ischemic injury involving more than one third of the middle cerebral artery territory, and those with a history of both stroke and diabetes mellitus.Citation28,Citation34
Side effects of IV tPA and risk of hemorrhagic outcomes
Although intracerebral hemorrhage (ICH) is the most feared complication of tPA, other potential adverse reactions including anaphylaxis/angio edema, systemic bleeding, and myocardial rupture occur less commonly. Myocardial rupture has been associated with patients receiving IV tPA within days of an acute myocardial infarction (MI).Citation34 While comorbid acute MI is listed as a relative contraindication to IV tPA, treatment in this setting must be assessed on a case-by-case basis regarding stroke severity and overall risk to benefit; particularly considering that fibrinolytic therapy is actually in the treatment pathway for acute STEMI (ST segment elevation MI) when percutaneous coronary intervention is delayed.Citation44 Signs of pericarditis are a more concerning contraindication for use of systemic tPA given the possibility of pericardial hemorrhage and tamponade.
Orolingual angioedema occurs in roughly 1%–5% of AIS patients treated with IV tPA. The reaction is typically contralateral to the location of the stroke and associated with infarcts involving the frontal and insular cortices. The concomitant use of angiotensin-converting enzyme inhibitors increases the risk due to excess bradykinin, and the reaction, although typically transient, can be treated with antihistamines or steroids.Citation34,Citation45
As stated above, the most important concern associated with the use of tPA in acute stroke patients is the fear of hemorrhagic complications. A number of factors pertain to risk of poor outcome from hemorrhage, such as location, nature of hemorrhage (hemorrhagic infarcts versus parenchymal hematomas), clinical status (symptomatic versus asymptomatic), and temporal relationship to treatment.Citation46–Citation48 In the NINDS study, the disease-related mortality rate in sICH cases was 47%, but the global mortality rate in all tPA-treated patients was lower compared with placebo. Other subsequent trials, except for ATLANTIS-A, revealed a similar increase in sICH for tPA-treated patients, with no difference in overall mortality.Citation1,Citation19,Citation20,Citation26,Citation29,Citation49 Analysis of ECASS II revealed an association of parenchymal hematomas and sICH with tPA but not hemorrhagic infarcts.Citation50 Additional studies and meta-analysis have reported differing rates of hemorrhage,Citation32,Citation48,Citation51,Citation52 in part due to varying definitions of sICH, including differences in measures of neurological symptoms, temporal relationship to treatment, and radiographic characteristics ().Citation53,Citation54 For instance, the sICH rate in ECASS III was 5% lower than in the NINDS study. However, when the NINDS definition is applied, the rate is higher than in the NINDS study (7.9%).Citation33
Table 2 tPA-related hemorrhage as defined by different stroke studies
Hemorrhagic risk and prognostic factors
Over the years, several pretreatment risk factor profiles have been studied to discern which individuals are more likely to benefit from tPA or to be at risk of sICH.Citation55–Citation59 In 1997, a post hoc subgroup analysis of the NINDS tPA data identified age-by-deficit severity interaction, history of diabetes, age-by-blood pressure interaction, and early computed tomography (CT) findings as factors altering long-term outcome in both groups, but no interaction was found with efficacy of tPA; therefore, tPA-treated patients in both groups still benefited. In addition, the only variables associated with increased risk of sICH were stroke severity, presence of brain edema, and mass effect on CT prior to treatment.Citation60 Since then, a number of analyses have reported additional baseline factors associated with tPA-related functional outcomes and risk of hemorrhagic transformation ().Citation50,Citation52,Citation56,Citation57 Moreover, the occurrence of sICH has been correlated with worsened 3-month outcomes.Citation53,Citation54,Citation57 Using NINDS trial data, SaverCitation61 calculated a number-needed-to-harm of 126 tPA-treated patients for every one case of sICH leading to severe disability or death, and a number-needed-to-treat of 17 to cause one protocol-defined sICH. A similar analysis of the 3.0–4.5-hour window using ECASS III data revealed an number-needed-to-harm of 35.Citation62 These figures are countered, however, by a number-needed-to-benefit of 7–8 in both trials favoring treatment.
Table 3 Risk factor profiles associated with negative outcomes after use of tPA in acute ischemic stroke
Risk and prognostic stratification scales
A number of statistical prognostic models have derived scores attempting to stratify treatment by predicted risk and outcomes (). However, such decision-support tools raise ethical questions regarding whether tPA can be withheld in an otherwise eligible patient based on a risk/prognostic stratification score. Additionally, further external validation in independent cohorts is required prior to utilization in clinical practice.Citation63 Ongoing research of advanced multimodal imaging and other biomarkers may someday potentiate the utility of decision-support tools for acute stroke treatment.
Table 4 Risk and prognostic stratification scales
Imaging-guided thrombolysis
Rapid acquisition of a non-contrasted CT scan of the head is universally part of acute stroke treatment protocol, primarily to rule out ICH as exclusion for tPA treatment, although other exclusions such as early infarction in more than two-thirds of a vascular territory have been suggested.Citation34,Citation64 With technological advancements in multimodal CT and MRI, imaging-guided thrombolysis has gained interest as a potential tool to identify the extent of salvageable tissue, otherwise known as the ischemic penumbra. Davalos et alCitation64 initially proposed a clinical–radiological mismatch in 2004 as a means of estimating treatment outcome. The DEFUSE (Diffusion and Perfusion Imaging Evaluation for Understanding Stroke Evolution), EPITHET (Echoplanar Imaging Thrombolytic Evaluation Trial), and MR RESCUE (Magnetic Resonance and Recanalization of Stroke Clots Using Embolectomy) studies all proposed varying definitions of imaging-based penumbral assessment, but none of these trials has demonstrated that the use of such imaging can identify a population that has improved outcomes with intervention than those without it.Citation65–Citation67 For now, the utility of perfusion-based imaging to guide tPA treatment decisions remains to be proven.
The benefits and risks of IV thrombolysis in certain subgroups
Based on both the clinical trial and subsequent clinical practice experience, a number of subgroups of stroke patients have been identified in whom effectiveness and safety of tPA varies. Here, we highlight a few of the more commonly encountered subgroups for which treatment decisions remain challenging in clinical practice.
Mild and rapidly improving
Studies evaluating exclusion criteria for receiving tPA highlight that 29%–43% of patients are excluded from thrombolysis for rapidly improving or mild symptoms (RIMS).Citation68–Citation71 The assumption has been made that mild and/or rapidly improving strokes will follow a natural course of favorable functional outcome in spite of accepting the additional risk of tPA. However, a few small studies have demonstrated that about a third of these patients left untreated will die or are unable to be discharged home due to neurological dysfunction.Citation72,Citation73 Rajajee et alCitation73 identified a large-vessel occlusion on magnetic resonance angiography corresponding to the acute stroke in 33% of patients excluded from tPA due to RIMS. The findings were later supported using results from a large nationwide database, with 28.3% of untreated patients with RIMS not discharged home and 28.5% unable to ambulate without assistance at discharge.Citation72 Whereas all of the above studies evaluated outcomes at time of discharge, Nedeltchev et alCitation74 evaluated 3-month outcomes for untreated patients with RIMS and found that 75% had a favorable outcome. However, three small studies have shown a significant improvement in clinical outcome with no increased risk of hemorrhage in tPA-treated RIMS patients.Citation75–Citation77 These were supported by a subgroup analysis from the ECASS III study, revealing similar efficacy of tPA in both mild and more severe strokes.Citation78 A prospective, randomized placebo-controlled trial has been proposed to evaluate stroke patients with non-disabling deficits within 4.5 hours of onset.Citation79,Citation80
Older age
A third of the patients presenting with ischemic stroke are over the age of 80.Citation81,Citation82 Kammersgaard et alCitation83 evaluated the short- and long-term prognosis in elderly stroke patients and revealed that patients over 80 were more likely to die in the hospital and less likely to have a favorable outcome. In addition, elderly patients may be at an increased risk of ICH due to cerebral amyloid angiopathy, impaired renal clearance, and frail vasculature.Citation84–Citation86 Many clinicians withhold treatment due to fear that age is associated with poor prognosis and increased risk of hemorrhage. With the exception of the NINDS study, patients ≥80 were excluded from the early clinical tPA trials. Of the 49 patients over the age of 75 included in the NINDS tPA trial, outcome was related to age-by-neurologic deficit but did not alter treatment effect. In addition, age did not independently increase the risk of hemorrhage.Citation60 Tanne et alCitation87 found comparable favorable outcomes and risks in patients aged ≥80 versus <80. Conversely, several studies that followed reported a reduction in favorable outcome and increased mortality in tPA-treated patients aged ≥80 compared with their younger counterparts, with conflicting sICH rates.Citation88–Citation92 Notable limitations of the above studies were small sample size, retrospective analysis, and confounding factors (eg, preexisting disability and comorbidities). In 2010, Mishra et alCitation93 compared elderly patients treated with thrombolysis with those not treated, from two large registries. They reported favorable outcomes independently among patients aged ≤80 (OR 1.6 [CI 1.5–1.7]; P<0.001) and in those >80 (OR 1.4 [CI 1.3–1.6]; P<0.001). In addition, there was a slight increase of sICH among patients >80 but not statistically significant (P=0.07).Citation93 Despite the increased power, the treatment allocation was not randomized, and therefore the results are subject to bias and confounding. The Third International Stroke Trial (IST-3) was the first prospective randomized trial to include a sizable number of patients >80 years (53%). A subgroup analysis from IST-3 suggested a greater benefit from tPA in patients older than 80 compared with their younger counterparts (P=0.027).Citation94 Based on these results, tPA should not be withheld based purely on age, and in fact, patients older than 80 may do as well if not better with treatment compared with control. As worldwide life expectancy and incidence of stroke in the elderly continue to increase in the future, the importance of treating older stroke patients will continue to hold relevance.Citation95
Stroke mimics
Complicating treatment decisions, numerous disease processes mimic stroke symptoms. lists some of the more common masqueraders of stroke with conversion disorder, complicated migraine, and seizures being the most frequently encountered.Citation96–Citation100 The need for rapid recognition and treatment of AIS potentiates the likelihood of administering tPA to a stroke mimic. The fraction of stroke mimics among tPA-treated patients in various cohorts has been reported between 1% and 31%, with community hospitals reporting rates as high as 25%–29%.Citation97,Citation100–Citation106 Some variation in these percentages reflect the lack of standard mimic definitions and/or inaccuracies in diagnosis reporting.Citation101 There have been a number of studies evaluating the characteristics, risk, and functional outcome of tPA-treated stroke mimics. Common characteristics of stroke mimics are young age, female sex, no or few baseline risk factors, left hemispheric syndromes, and milder presenting stroke severity.Citation97,Citation100,Citation106,Citation107 In addition, aphasia, particularly when global and not presenting with any other deficits, is one of the most commonly cited presentations of stroke mimics.Citation106,Citation107 The safety of tPA in stroke mimics was evaluated in a multicenter observational study that revealed an sICH rate of 1.0% (CI 0.0–5.0) in mimics compared with 7.9% (CI 7.2–8.7) in imaging-confirmed ischemic stroke. Predictably, treated stroke mimics were more likely to experience an excellent outcome at 3 months compared with AIS (75% versus 39.5%; P<0.0001).Citation107 Further studies have supported the safety of tPA use in stroke mimics, with minimal complicating disability or ICH.Citation98–Citation100,Citation102
Table 5 Common stroke mimics
Translating trials to clinical practice experience
Both academic and community-based studies have sought to evaluate whether tPA is as effective and safe when integrated into clinical practice as demonstrated in the controlled setting of clinical trials. Indeed, community-based studies and large clinical databases have elicited similar and, in some cases, lower rates of sICH than those revealed in trials (). In populations where sICH rates were higher, adherence to strict guidelines and protocols likely varied.Citation108 Hill and BuchanCitation109 reported an association between sICH and frequency of protocol violations, but no correlation with worse functional outcomes. Not surprisingly, a survey of practice patterns has found that tPA experience and neurological expertise are associated with fewer protocol violations in general.Citation110 Overall, results from clinical trials of IV tPA in stroke have been widely generalizable to the clinical practice experience.
Table 6 Community-based studies on the experience of tPA utilization for acute ischemic stroke
Despite the overwhelming body of evidence supporting the use of IV tPA in all eligible AIS patients, there remains an undercurrent of reservation in the practicing community at large. In 2005, a national survey of emergency medicine physicians found that 40% were unlikely to use tPA for ischemic stroke under ideal conditions. Of those unlikely to use tPA, 65% were apprehensive about risk of hemorrhage, while 23% believed there was a lack of benefit.Citation111 More recently, the emergency medicine community has offered support for the use of tPA for AIS as standard care as demonstrated by guidelines.Citation4 In 2013, a survey of Canadian neurologists who routinely take acute stroke call demonstrated that concerns are not limited to emergency medical physicians. The majority of respondents (79%) were less likely to treat at ages older than 80, those with dementia, or even patients with severe strokes or from nursing homes. However, a significant percentage (70%) believed a large left middle cerebral artery territory stroke was a fate worse than death, with the overwhelming majority (96%) believing IV tPA to be an effective stroke treatment.Citation112
Apart from individual or group biases, the medical-legal implications of tPA use in clinical practice are difficult to ignore. Over the years, the agreed-upon standard of care in AIS has shifted liability from risk of sICH with tPA to litigation for not offering treatment in otherwise eligible stroke patients.Citation113,Citation114 Guideline statements from AHA/ASA, AAN, and ACEP all suggest IV tPA is standard care for treatment of AIS.Citation2–Citation4,Citation34
Conclusion
From the first human trials to today’s current practice, effective tPA treatment for AIS continues to rely on appropriate patient screening, rapid diagnosis and decision making, strict adherence to protocol, and one-size-fits-all time windows. Current evidence-based recommendations for the use of IV tPA in AIS can be referenced from the AHA/ASA 2013 update, titled Guidelines for the Early Management of Patients With Acute Ischemic Stroke (see Tables 10–12 for eligibility criteria and general recommendations for appropriate use).Citation34 Prognostic and risk stratification scales and advanced multimodal imaging may one day guide treatment decisions, but these tools have not yet been established to guide clinical practice.
Analysis of recent census data suggests that the incidence of AIS will nearly double to 1.5 million per year by 2050.Citation95 In the meantime, stroke remains a leading cause of serious long-term disability and death worldwide, and almost 20 years since its approval, IV tPA remains an underutilized, yet highly efficacious first-line treatment. Ongoing and future research investigating innovative approaches to timelier treatment and novel means of stroke thrombolysis will no doubt continue to revolutionize acute stroke care.
In addition to research focused on acute stroke treatment delivery, there continue to be a number of ongoing trials regarding the risk and efficacy of IV tPA in a number of patient subgroups. Active studies are investigating a variety of potential variables affecting the use of tPA in stroke including but not limited to age, weight, hyperglycemia, dialysis, time-to-presentation, and mild or rapidly improving symptoms. Reference to these and other ongoing studies of IV tPA in stroke can be found at http://www.clinicaltrials.gov. For now, promoting education within both the medical community and general public is a sure path to advance the use of IV tPA in all eligible stroke patients and further alleviate the burden of stroke for our society. After all, in addition to the code of “primum non nocere”, we must also consider autonomy and beneficence.
Author contributions
Sherita N Chapman conceived and designed the manuscript, carried out data acquisition, and critically revised the manuscript. Prachi Mehndiratta designed the manuscript, carried out data acquisition, and critically revised the manuscript. Michelle C Johansen conceived and designed the manuscript, carried out data acquisition, and critically revised the manuscript. Timothy L McMurry carried out statistical analysis and drafted forest plots, and helped design and critically revise the manuscript. Karen C Johnston and Andrew M Southerland conceived, drafted, and critically revised the manuscript.
Disclosure
Karen C Johnston reports her role as chair of the Data and Safety Monitoring Board for PRISMS trial. The other authors report no conflicts of interest in this work.
References
- Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study GroupN Engl J Med1995333158115877477192
- AdamsHPJrBrottTGFurlanAJGuidelines for thrombolytic therapy for acute stroke: a supplement to the guidelines for the management of patients with acute ischemic stroke. A statement for healthcare professionals from a special writing group of the stroke council, American Heart AssociationStroke199627171117188784157
- Practice advisory: thrombolytic therapy for acute ischemic stroke – summary statement. Report of the Quality Standards Subcommittee of the American Academy of NeurologyNeurology1996478358398797492
- American College of Emergency PhysiciansAmerican Academy of NeurologyClinical policy: use of intravenous tPA for the management of acute ischemic stroke in the emergency departmentAnn Emerg Med20136122524323331647
- GoASMozaffarianDRogerVLHeart disease and stroke statistics – 2013 update: a report from the American Heart AssociationCirculation2013127e6e24523239837
- FonarowGCSmithEESaverJLImproving door-to-needle times in acute ischemic stroke: the design and rationale for the American Heart Association/American Stroke Association’s Target: Stroke initiativeStroke2011422983298921885841
- CaplanLRMohrJPKistlerJPKoroshetzWShould thrombolytic therapy be the first-line treatment for acute ischemic stroke? Thrombolysis – not a panacea for ischemic strokeN Engl J Med199733713091310 discussion 13139345084
- FirstenbergMSThrombolytic therapy in acute ischemic strokeN Engl J Med199733666 author reply 66–678984334
- ClarkWMLydenPDMaddenKPZivinJAThrombolytic therapy in acute ischemic strokeN Engl J Med19973366566 author reply 66–678984333
- FrankelMRThrombolytic therapy in acute ischemic strokeN Engl J Med199733665 author reply 66–678984332
- KirshnerHSShould thrombolytic therapy be the first-line treatment for acute ischemic stroke?N Engl J Med1998338761762 author reply 762–7639499171
- LevinBThompsonJLChakrabortyBLevyGMacArthurRHaleyECStatistical aspects of the TNK-S2B trial of tenecteplase versus alteplase in acute ischemic stroke: an efficient, dose-adaptive, seamless Phase II/III designClin Trials2011839840721737464
- HackeWFurlanAJAl-RawiYIntravenous desmoteplase in patients with acute ischaemic stroke selected by MRI perfusion-diffusion weighted imaging or perfusion CT (DIAS-2): a prospective, randomised, double-blind, placebo-controlled studyLancet Neurol2009814115019097942
- HackeWAlbersGAl-RawiYThe Desmoteplase in Acute Ischemic Stroke Trial (DIAS): a phase II MRI-based 9-hour window acute stroke thrombolysis trial with intravenous desmoteplaseStroke200536667315569863
- del ZoppoGJPoeckKPessinMSRecombinant tissue plasminogen activator in acute thrombotic and embolic strokeAnn Neurol19923278861642475
- BrottTGHaleyECJrLevyDEUrgent therapy for stroke. Part I. Pilot study of tissue plasminogen activator administered within 90 minutesStroke1992236326401579958
- HaleyECJrLevyDEBrottTGUrgent therapy for stroke. Part II. Pilot study of tissue plasminogen activator administered 91–180 minutes from onsetStroke1992236416451579959
- MoriEYonedaYTabuchiMIntravenous recombinant tissue plasminogen activator in acute carotid artery territory strokeNeurology1992429769821579252
- ClarkWMAlbersGWMaddenKPHamiltonSThe rtPA (alteplase) 0- to 6-hour acute stroke trial, part A (A0276g): results of a double-blind, placebo-controlled, multicenter study. Thromblytic therapy in acute ischemic stroke study investigatorsStroke20003181181610753980
- HackeWKasteMFieschiCIntravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. The European Cooperative Acute Stroke Study (ECASS)JAMA1995274101710257563451
- BrottTAdamsHPJrOlingerCPMeasurements of acute cerebral infarction: a clinical examination scaleStroke1989208648702749846
- BrownDLJohnstonKCWagnerDPHaleyECJrPredicting major neurological improvement with intravenous recombinant tissue plasminogen activator treatment of strokeStroke20043514715014657446
- HaleyECJrLewandowskiCTilleyBCMyths regarding the NINDS rt-PA Stroke Trial: setting the record straightAnn Emerg Med1997306766829360581
- DonnanGADavisSMChambersBRStreptokinase for acute ischemic stroke with relationship to time of administration: Australian Streptokinase (ASK) Trial Study GroupJAMA19962769619668805730
- HortonRMAST-I: agreeing to disagree. Multicentre Acute Stroke Trial – Italy GroupLancet199534615047491039
- AlbersGWClarkWMMaddenKPHamiltonSAATLANTIS trial: results for patients treated within 3 hours of stroke onset. Alteplase Thrombolysis for Acute Noninterventional Therapy in Ischemic StrokeStroke20023349349511823658
- HackeWBluhmkiESteinerTDichotomized efficacy end points and global end-point analysis applied to the ECASS intention-to-treat data set: post hoc analysis of ECASS IStroke199829207320759756584
- WardlawJMMurrayVBergeEDel ZoppoGJThrombolysis for acute ischaemic strokeCochrane Database Syst Rev20094CD00021319821269
- HackeWKasteMFieschiCRandomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Second European-Australasian Acute Stroke Study InvestigatorsLancet1998352124512519788453
- RinglebPASchellingerPDSchranzCHackeWThrombolytic therapy within 3 to 6 hours after onset of ischemic stroke: useful or harmful?Stroke2002331437144111988629
- MaHParsonsMWChristensenSA multicentre, randomized, double-blinded, placebo-controlled Phase III study to investigate EXtending the time for Thrombolysis in Emergency Neurological Deficits (EXTEND)Int J Stroke20127748022188854
- HackeWDonnanGFieschiCAssociation of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trialsLancet200436376877415016487
- HackeWKasteMBluhmkiEThrombolysis with alteplase 3 to 4.5 hours after acute ischemic strokeN Engl J Med20083591317132918815396
- JauchECSaverJLAdamsHPJrGuidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke AssociationStroke20134487094723370205
- BaronJCvon KummerRdel ZoppoGJTreatment of acute ischemic stroke. Challenging the concept of a rigid and universal time windowStroke199526221922217491639
- AzzimondiGBasseinLFioraniLVariables associated with hospital arrival time after stroke: effect of delay on the clinical efficiency of early treatmentStroke1997285375429056608
- LevyDEBrottTGHaleyECJrFactors related to intracranial hematoma formation in patients receiving tissue-type plasminogen activator for acute ischemic strokeStroke1994252912978303734
- MarlerJRTilleyBCLuMEarly stroke treatment associated with better outcome: the NINDS rt-PA stroke studyNeurology2000551649165511113218
- SaverJLTime is brain – quantifiedStroke20063726326616339467
- SaverJLFonarowGCSmithEETime to treatment with intravenous tissue plasminogen activator and outcome from acute ischemic strokeJAMA20133092480248823780461
- FonarowGCSmithEESaverJLTimeliness of tissue-type plasminogen activator therapy in acute ischemic stroke: patient characteristics, hospital factors, and outcomes associated with door-to-needle times within 60 minutesCirculation201112375075821311083
- LimanTGWinterBWaldschmidtCTelestroke ambulances in prehospital stroke management: concept and pilot feasibility studyStroke2012432086209022693132
- MeretojaAStrbianDMustanojaSTatlisumakTLindsbergPJKasteMReducing in-hospital delay to 20 minutes in stroke thrombolysisNeurology20127930631322622858
- O’GaraPTKushnerFGAscheimDD2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice GuidelinesCirculation2013127e362e42523247304
- HillMDLyeTMossHHemi-orolingual angioedema and ace inhibition after alteplase treatment of strokeNeurology2003601525152712743244
- PessinMSDel ZoppoGJEstolCJThrombolytic agents in the treatment of strokeClin Neuropharmacol1990132712892208179
- TrouillasPvon KummerRClassification and pathogenesis of cerebral hemorrhages after thrombolysis in ischemic strokeStroke20063755656116397182
- DerexLNighoghossianNIntracerebral haemorrhage after thrombolysis for acute ischaemic stroke: an updateJ Neurol Neurosurg Psychiatry2008791093109918223014
- ClarkWMWissmanSAlbersGWJhamandasJHMaddenKPHamiltonSRecombinant tissue-type plasminogen activator (Alteplase) for ischemic stroke 3 to 5 hours after symptom onset. The ATLANTIS Study: a randomized controlled trial. Alteplase Thrombolysis for Acute Noninterventional Therapy in Ischemic StrokeJAMA19992822019202610591384
- LarrueVvon KummerRRMullerABluhmkiERisk factors for severe hemorrhagic transformation in ischemic stroke patients treated with recombinant tissue plasminogen activator: a secondary analysis of the European-Australasian Acute Stroke Study (ECASS II)Stroke20013243844111157179
- HackeWBrottTCaplanLThrombolysis in acute ischemic stroke: controlled trials and clinical experienceNeurology199953S3S1410532643
- WahlgrenNAhmedNErikssonNMultivariable analysis of outcome predictors and adjustment of main outcome results to baseline data profile in randomized controlled trials: Safe Implementation of Thrombolysis in Stroke-MOnitoring STudy (SITS-MOST)Stroke2008393316332218927461
- StrbianDSairanenTMeretojaAPatient outcomes from symptomatic intracerebral hemorrhage after stroke thrombolysisNeurology20117734134821715707
- SoutherlandAMMalikSJohnstonKCSymptomatic ICH and outcomes in patients after IV tPA: a business of risk or risky business?Neurology20117731531621715703
- DemchukAMMorgensternLBKriegerDWSerum glucose level and diabetes predict tissue plasminogen activator-related intracerebral hemorrhage in acute ischemic strokeStroke19993034399880385
- TanneDKasnerSEDemchukAMMarkers of increased risk of intracerebral hemorrhage after intravenous recombinant tissue plasminogen activator therapy for acute ischemic stroke in clinical practice: the Multicenter rt-PA Stroke SurveyCirculation20021051679168511940547
- SaposnikGDi LeggeSWebsterFHachinskiVPredictors of major neurologic improvement after thrombolysis in acute strokeNeurology2005651169117416247041
- BatemanBTSchumacherHCBoden-AlbalaBFactors associated with in-hospital mortality after administration of thrombolysis in acute ischemic stroke patients: an analysis of the nationwide inpatient sample 1999 to 2002Stroke20063744044616397164
- MazyaMEgidoJAFordGAPredicting the risk of symptomatic intracerebral hemorrhage in ischemic stroke treated with intravenous alteplase: safe implementation of treatments in stroke (SITS) symptomatic intracerebral hemorrhage risk scoreStroke2012431524153122442178
- Generalized efficacy of t-PA for acute stroke. Subgroup analysis of the NINDS t-PA Stroke TrialStroke199728211921259368551
- SaverJLDeriving number-needed-to-treat and number-needed-to-harm from the SAINT I trial resultsStroke200738257 author reply 25817185635
- SaverJLGornbeinJGrottaJNumber needed to treat to benefit and to harm for intravenous tissue plasminogen activator therapy in the 3- to 4.5-hour window: joint outcome table analysis of the ECASS 3 trialStroke2009402433243719498197
- RabinsteinARundekTPrediction of outcome after ischemic stroke: the value of clinical scoresNeurology201380151623175728
- DavalosABlancoMPedrazaSThe clinical-DWI mismatch: a new diagnostic approach to the brain tissue at risk of infarctionNeurology2004622187219215210880
- LansbergMGThijsVNHamiltonSEvaluation of the clinical-diffusion and perfusion-diffusion mismatch models in DEFUSEStroke2007381826183017495217
- KidwellCSJahanRSaverJLEndovascular treatment for acute ischemic strokeN Engl J Med20133682434243523802241
- DavisSMDonnanGAParsonsMWEffects of alteplase beyond 3 h after stroke in the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET): a placebo-controlled randomised trialLancet Neurol2008729930918296121
- BarberPAZhangJDemchukAMHillMDBuchanAMWhy are stroke patients excluded from tPA therapy? An analysis of patient eligibilityNeurology2001561015102011320171
- KatzanILHammerMDHixsonEDFurlanAJAbou-CheblANadzamDMUtilization of intravenous tissue plasminogen activator for acute ischemic strokeArch Neurol20046134635015023810
- CochoDBelvisRMarti-FabregasJReasons for exclusion from thrombolytic therapy following acute ischemic strokeNeurology20056471972015728300
- KleindorferDKisselaBSchneiderAEligibility for recombinant tissue plasminogen activator in acute ischemic stroke: a population-based studyStroke200435e27e2914739423
- SmithEEFonarowGCReevesMJOutcomes in mild or rapidly improving stroke not treated with intravenous recombinant tissue-type plasminogen activator: findings from Get With The Guidelines – StrokeStroke2011423110311521903949
- RajajeeVKidwellCStarkmanSEarly MRI and outcomes of untreated patients with mild or improving ischemic strokeNeurology20066798098417000964
- NedeltchevKSchweglerBHaefeliTOutcome of stroke with mild or rapidly improving symptomsStroke2007382531253517673713
- BaumannCRBaumgartnerRWGandjourJvon BudingenHCSiegelAMGeorgiadisDGood outcomes in ischemic stroke patients treated with intravenous thrombolysis despite regressing neurological symptomsStroke2006371332133316556881
- KohrmannMNoweTHuttnerHBSafety and outcome after thrombolysis in stroke patients with mild symptomsCerebrovasc Dis20092716016619092237
- HassanAEHassanzadehBTohidiVKirmaniJFVery mild stroke patients benefit from intravenous tissue plasminogen activator without increase of intracranial hemorrhageSouth Med J201010339840220375952
- BluhmkiEChamorroADavalosAStroke treatment with alteplase given 3.0–4.5 h after onset of acute ischaemic stroke (ECASS III): additional outcomes and subgroup analysis of a randomised controlled trialLancet Neurol200981095110219850525
- SaverJLImproving reperfusion therapy for acute ischaemic strokeJ Thromb Haemost20119Suppl 133334321781270
- KhatriPConawayMRJohnstonKCNinety-day outcome rates of a prospective cohort of consecutive patients with mild ischemic strokeStroke20124356056222052513
- MariniCBaldassarreMRussoTBurden of first-ever ischemic stroke in the oldest old: evidence from a population-based studyNeurology200462778114718701
- DerexLNighoghossianNThrombolysis, stroke-unit admission and early rehabilitation in elderly patientsNat Rev Neurol2009550651119652651
- KammersgaardLPJorgensenHSReithJNakayamaHPedersenPMOlsenTSShort- and long-term prognosis for very old stroke patients. The Copenhagen Stroke StudyAge Ageing20043314915414960430
- SloanMAPriceTRPetitoCKClinical features and pathogenesis of intracerebral hemorrhage after rt-PA and heparin therapy for acute myocardial infarction: the Thrombolysis in Myocardial Infarction (TIMI) II Pilot and Randomized Clinical Trial combined experienceNeurology1995456496587723950
- GreenbergSMVonsattelJPDiagnosis of cerebral amyloid angiopathy. Sensitivity and specificity of cortical biopsyStroke199728141814229227694
- HaleyKEGreenbergSMGurolMECerebral microbleeds and macrobleeds: should they influence our recommendations for antithrombotic therapies?Curr Cardiol Rep20131542524122195
- TanneDGormanMJBatesVEIntravenous tissue plasminogen activator for acute ischemic stroke in patients aged 80 years and older: the tPA stroke survey experienceStroke20003137037510657408
- MeretojaAPutaalaJTatlisumakTOff-label thrombolysis is not associated with poor outcome in patients with strokeStroke2010411450145820538701
- SylajaPNCoteRBuchanAMHillMDThrombolysis in patients older than 80 years with acute ischaemic stroke: Canadian alteplase for stroke effectiveness studyJ Neurol Neurosurg Psychiatry20067782682916505004
- van OostenbruggeRJHuppertsRMLodderJThrombolysis for acute stroke with special emphasis on the very old: experience from a single Dutch centreJ Neurol Neurosurg Psychiatry20067737537716484647
- EngelterSTBonatiLHLyrerPAIntravenous thrombolysis in stroke patients of > or =80 versus <80 years of age – a systematic review across cohort studiesAge Ageing20063557258017047006
- MouradianMSSenthilselvanAJicklingGIntravenous rt-PA for acute stroke: comparing its effectiveness in younger and older patientsJ Neurol Neurosurg Psychiatry2005761234123716107357
- MishraNKAhmedNAndersenGThrombolysis in very elderly people: controlled comparison of SITS International Stroke Thrombolysis Registry and Virtual International Stroke Trials ArchiveBMJ2010341c604621098614
- SandercockPWardlawJMLindleyRIThe benefits and harms of intravenous thrombolysis with recombinant tissue plasminogen activator within 6 h of acute ischaemic stroke (the Third International Stroke Trial [IST-3]): a randomised controlled trialLancet20123792352236322632908
- HowardGGoffDCPopulation shifts and the future of stroke: forecasts of the future burden of strokeAnn N Y Acad Sci20121268142022994216
- RudolfJTsivgoulisGDeretziGFeasibility and safety of intravenous thrombolysis for acute ischaemic stroke in northern GreeceInt J Stroke20116919221205250
- ChernyshevOYMartin-SchildSAlbrightKCSafety of tPA in stroke mimics and neuroimaging-negative cerebral ischemiaNeurology2010741340134520335564
- WinklerDTFluriFFuhrPThrombolysis in stroke mimics: frequency, clinical characteristics, and outcomeStroke2009401522152519164790
- ScottPASilbergleitRMisdiagnosis of stroke in tissue plasminogen activator-treated patients: characteristics and outcomesAnn Emerg Med20034261161814581912
- TsivgoulisGAlexandrovAVChangJSafety and outcomes of intravenous thrombolysis in stroke mimics: a 6-year, single-care center study and a pooled analysis of reported seriesStroke2011421771177421493900
- GuerreroWRSavitzSITissue-type plasminogen activator for stroke mimics: continuing to be swift rather than delaying treatment to be sureStroke2013441213121423579589
- HandPJKwanJLindleyRIDennisMSWardlawJMDistinguishing between stroke and mimic at the bedside: the brain attack studyStroke20063776977516484610
- LibmanRBWirkowskiEAlvirJRaoTHConditions that mimic stroke in the emergency department. Implications for acute stroke trialsArch Neurol199552111911227487564
- AndersonCSJamrozikKDBurvillPWChakeraTMJohnsonGAStewart-WynneEGAscertaining the true incidence of stroke: experience from the Perth Community Stroke Study, 1989–1990Med J Aust199315880848419780
- EllekjaerHHolmenJIndredavikBTerentAEpidemiology of stroke in Innherred, Norway, 1994 to 1996. Incidence and 30-day case-fatality rateStroke199728218021849368561
- ArttoVPutaalaJStrbianDStroke mimics and intravenous thrombolysisAnn Emerg Med201259273222000770
- ZinkstokSMEngelterSTGensickeHSafety of thrombolysis in stroke mimics: results from a multicenter cohort studyStroke2013441080108423444310
- Marti-FabregasJBravoYCochoDFrequency and predictors of symptomatic intracerebral hemorrhage in patients with ischemic stroke treated with recombinant tissue plasminogen activator outside clinical trialsCerebrovasc Dis200723859017114877
- HillMDBuchanAMThrombolysis for acute ischemic stroke: results of the Canadian Alteplase for Stroke Effectiveness StudyCMAJ20051721307131215883405
- MeschiaJFWilliamsLSFleckJDBrunoABillerJViews on the use of tissue plasminogen activator in acute ischemic stroke: a state-wide survey among neurologists and emergency medicine physicians in IndianaJ Stroke Cerebrovasc Dis1999820721017895166
- BrownDLBarsanWGLisabethLDGalleryMEMorgensternLBSurvey of emergency physicians about recombinant tissue plasminogen activator for acute ischemic strokeAnn Emerg Med200546566015988427
- ShamyMCJaigobinCSThe complexities of acute stroke decision-making: a survey of neurologistsNeurology2013811130113323946306
- WeintraubMIThrombolysis (tissue plasminogen activator) in stroke: a medicolegal quagmireStroke2006371917192216728683
- LiangBAZivinJAEmpirical characteristics of litigation involving tissue plasminogen activator and ischemic strokeAnn Emerg Med20085216016418313798
- CucchiaraBTanneDLevineSRDemchukAMKasnerSA risk score to predict intracranial hemorrhage after recombinant tissue plasminogen activator for acute ischemic strokeJ Stroke Cerebrovasc Dis20081733133318984422
- LouMSafdarAMehdirattaMThe HAT score: a simple grading scale for predicting hemorrhage after thrombolysisNeurology2008711417142318955684
- MenonBKSaverJLPrabhakaranSRisk score for intracranial hemorrhage in patients with acute ischemic stroke treated with intravenous tissue-type plasminogen activatorStroke2012432293229922811458
- StrbianDEngelterSMichelPSymptomatic intracranial hemorrhage after stroke thrombolysis: the SEDAN scoreAnn Neurol20127163464122522478
- StrbianDMeretojaAAhlhelmFJPredicting outcome of IV thrombolysis-treated ischemic stroke patients: the DRAGON scoreNeurology20127842743222311929
- SaposnikGGuzikAKReevesMOvbiageleBJohnstonSCStroke prognostication using age and NIH Stroke Scale: SPAN-100Neurology201380212823175723
- SaposnikGFangJKapralMKThe iScore predicts effectiveness of thrombolytic therapy for acute ischemic strokeStroke2012431315132222308252
- KentDMSelkerHPRuthazerRBluhmkiEHackeWThe stroke-thrombolytic predictive instrument: a predictive instrument for intravenous thrombolysis in acute ischemic strokeStroke2006372957296217068305
- NtaiosGFaouziMFerrariJLangWVemmosKMichelPAn integer-based score to predict functional outcome in acute ischemic stroke: the ASTRAL scoreNeurology2012781916192222649218
- ChiuDKriegerDVillar-CordovaCIntravenous tissue plasminogen activator for acute ischemic stroke: feasibility, safety, and efficacy in the first year of clinical practiceStroke19982918229445322
- GrondMStenzelCSchmullingSEarly intravenous thrombolysis for acute ischemic stroke in a community-based approachStroke199829154415499707190
- KatzanILFurlanAJLloydLEUse of tissue-type plasminogen activator for acute ischemic stroke: the Cleveland area experienceJAMA20002831151115810703777
- WangSLPanWHLeeMCChengSPChangMCPredictors of survival among elders suffering strokes in Taiwan: observation from a nationally representative sampleStroke2000312354236011022063
- AlbersGWBatesVEClarkWMBellRVerroPHamiltonSAIntravenous tissue-type plasminogen activator for treatment of acute stroke: the Standard Treatment with Alteplase to Reverse Stroke (STARS) studyJAMA20002831145115010703776
- Lopez-YunezAMBrunoAWilliamsLSYilmazEZurruCBillerJProtocol violations in community-based rTPA stroke treatment are associated with symptomatic intracerebral hemorrhageStroke200132121611136907
- GrottaJCBurginWSEl-MitwalliAIntravenous tissue-type plasminogen activator therapy for ischemic stroke: Houston experience 1996 to 2000Arch Neurol2001582009201311735774
- KoenneckeHCNohrRLeistnerSMarxPIntravenous tPA for ischemic stroke team performance over time, safety, and efficacy in a single-center, 2-year experienceStroke2001321074107811340212
- BravataDMKimNConcatoJKrumholzHMBrassLMThrombolysis for acute stroke in routine clinical practiceArch Intern Med20021621994200112230423
- KatzanILHammerMDFurlanAJHixsonEDNadzamDMQuality improvement and tissue-type plasminogen activator for acute ischemic stroke: a Cleveland updateStroke20033479980012624312