
Abstract
Background
The prevalence and incidence of stroke vary from community to community worldwide. Nonetheless, not much is known about the current epidemiology of stroke in rural Nigeria and indeed Africa.
Methods
We carried out a two-phase door-to-door survey in a rural, predominantly low-income, community in Anambra, Southeastern Nigeria. We used a modified World Health Organization (WHO) protocol for detecting neurological diseases in the first phase, and a stroke-specific questionnaire and neurological examination in the second phase. An equal number of sex- and age-matched stroke-negative subjects were examined.
Results
We identified ten stroke subjects in the study. The crude prevalence of stroke in rural Nigeria was 1.63 (95% confidence interval [CI] 0.78–3.00) per 1,000 population. The crude prevalence of stroke in males was 1.99 (95% CI 0.73–4.33) per 1,000, while that for females was 1.28 (95% CI 0.35–3.28) per 1,000 population. The peak age-specific prevalence of stroke was 12.08 (95% CI 3.92–28.19) per 1,000, while after adjustment to WHO world population, the peak was 1.0 (95% CI 0.33–2.33) per 1,000.
Conclusion
The prevalence of stroke was found to be higher than previously documented in rural Nigeria, with a slightly higher prevalence in males than females. This is, however, comparable to data from rural Africa.
Keywords:
Introduction
Stroke has existed since medieval times and considerable progress has been made in the knowledge of its nature and epidemiology.Citation1,Citation2 It is the second leading cause of death worldwide.Citation3 The prevalence and incidence of stroke vary from community to community and from time to time worldwide. However, not much is known about the burden of stroke in sub-Saharan Africa.
The crude prevalence of stroke reported in a rural study in Southwestern Nigeria was 0.58 per 1,000 population,Citation4 while the incidence of stroke was found to be 26 per 100,000 in a Southwestern urban register-based study in Nigeria.Citation5 These studies were conducted more than two decades ago. Another relatively recent prevalence study in a Southwestern Nigerian urban community was found to be 1.14 per 1,000 population.Citation6 The current epidemiology of stroke in rural Nigeria is yet unknown.
Therefore, the purpose of this study was to determine the current epidemiology of stroke in a rural community in Southeastern Nigeria while maintaining a continuous register for the incidence of stroke.
Methodology
This study was conducted in Ukpo, a predominantly low-income rural community with a population of 17,840 and 3,820 households (based on data from The National Population Commission of Nigeria on the 2006 national population census). Ukpo is the headquarters of Dunukofia Local Government Area in Anambra State, Southeastern region of Nigeria. It is a community with undulating terrain caused by erosion, which makes it not easily accessible by some vehicles. The community’s source of clean water is a privately owned bore-hole. Electricity is sporadic, resulting in a few inhabitants using electricity-generating sets, while most use kerosene lanterns. The residents of the community are essentially monogamists, with few practicing polygamy. The majority are Christians, indigenous, and of the Igbo tribe. The community is stable and does not tolerate intertribal or interreligious marriages. The predominant occupation is peasant farming, and their diet is tuber-based. They are served by one fully functional primary health care center located at the center of the community. There is some labor migration out of the community. They usually return during festive periods and maintain households in the community. They do, however, return home when they become retired or are unable to work due to ill health.
Ethical clearance was obtained from the ethical committee of the Nnamdi Azikiwe University Teaching Hospital (NAUTH), Nnewi prior to commencement of the study. The study was a descriptive community-based door-to-door survey. It was conducted in two phases, preceded by a sensitization meeting with the community leaders (the Igwe-in-council) and a 2-day workshop with the research assistants. The village town criers, church leaders, and schools were engaged to make regular announcements weeks before the commencement of the survey. The research assistants were educated on the research procedures and the use of research instruments. This comprised a detailed review of the questionnaire, demonstration of interview technique, and back-demonstration by the research assistants. The 2-day workshop was fully attended by clinical medical students and other research assistants recruited for the first phase of the study. The medical students further participated in pre-testing the questionnaires on patients attending the medical outpatient clinic at the Nnamdi Azikiwe University Teaching Hospital, Nnewi on three consecutive clinic days and familiarized themselves with the research instrument.
Consent procedure
Informed oral consent was first obtained from the Honourable Commissioner for Health in the state, subsequently the traditional ruler of the community and his council of chiefs, then the heads of households and individual subjects. Furthermore, informed consent was obtained from spouses or close relatives of those subjects who were incapable of giving their informed oral consent. However, an informed written consent was obtained from those who participated in the second phase of the study.
Phase 1: census and door-to-door survey using modified World Health Organization (WHO) questionnaire
A census of the community was conducted in computer-generated random samples of 33% of the total enumeration areas 3 weeks prior to the survey to determine the average number of persons per enumeration area. The persons in each enumeration area were listed according to households using the name of the most prominent member. There was an average of 252 persons per enumeration area, estimating to a total Ukpo population of 18,648 using the 74 enumeration areas as obtained from the National Population Commission. Therefore 33% of the population, which was approximately 6,150 persons (25 enumeration areas), was selected for interview from the estimated Ukpo population using a table of computer-generated randomization. All the persons resident in the 25 randomly selected enumeration areas at the time of the study were included in both the census and the survey.
The first phase was conducted January 14–28, 2011. It was a door-to-door survey carried out by eight teams of trained research assistants, each comprising a health attendant, two medical students with at least 2 years of clinical experience, and a literate Ukpo resident as their liaison officer. The teams of research assistants administered the screening instrument on a total of 6,150 Ukpo residents. The screening instrument was the modified WHO questionnaire for detecting neurological diseases, and it was interviewer-administered to detect persons with probable stroke. It was adapted from the WHO protocol for detecting neurological diseases for the purpose of this study. The modifications included rearranging the order of the questions by bringing forth less probing questions before the more probing ones to improve participant cooperation, and exclusion of the physical examination components of the protocol to reduce administration time as the second phase of the study also had a physical examination component. Also, the questions for detecting tremors and Parkinsonism were removed for the above reasons. The questionnaire was translated to the local dialect and back-translated to English by two bilingual Igbo West African Examination Council examiners. The translated version was crosschecked by the neurologists who are versed in the Igbo language before back-translation and adjustments were made to remove or improve ambiguous questions. These were fully explained to the research assistants. The research instrument (stroke-specific questionnaire) was validated in the Medical Out-Patient Department of NAUTH Nnewi using 20 patients and 20 students as controls. This yielded 20 as true negative, 8 as false positive, 12 as true positive, and 0 as false negative. Therefore, the sensitivity was 100% while the specificity was 71%.
The cases identified in this phase of the study as having probable stroke were enlisted for the second phase of the study. A positive response to any of questions 4, 7, and 8 in the screening instrument was considered as probable stroke and a formal invitation extended to the person to come to the Neuroepidemiology outpatient clinic in NAUTH Health Centre Ukpo for the second phase of the study.
Phase 2: screening with stroke-specific questionnaire and examination of participants
The second phase of the study was conducted in the outpatient clinic of the NAUTH Health Centre Ukpo by means of a semi-structured stroke-specific questionnaire and focused clinical examination (Supplementary material; Figures S1–S4). The radial pulse and all other peripheral pulses were checked, blood pressure measured, carotid bruits listened for, and the heart checked for evidence of likely embolic sources and hypertensive end-organ damage. A neurologic examination was done independently on each subject to detect residual paralysis, hemisensory loss, exaggerated deep tendon jerks, and an extensor plantar response by two consultant neurologists blinded to each other’s results. Where there was disagreement, both neurologists reexamined the subject together and agreed on a common finding. An equal number of stroke-negative controls were randomly selected from those who screened negative for stroke to match subjects by age (±2 years) and sex. These controls were screened and examined for risk factors, as was done for the stroke subjects. The diagnosis of stroke was clinical, based on the WHO definition.
Data analysis
Data were confidentially collected with study codes, recorded, cleaned, and analyzed using Epi Info™ (Centers for Disease Control and Prevention, Atlanta, GA, USA) 3.5.1 2008 statistical software. Continuous variables were presented as means with standard deviations, while categorical variables were presented as proportions. Crude, age-specific, and age-adjusted prevalences (WHO World Standard Population)Citation7 were calculated alongside their confidence intervals (CIs). Student’s t-test was used to compare means, while Fisher’s exact test was used to compare categorical variables. P-value <0.05 was considered statistically significant.
Results
Demography of study population
A total of 6,150 persons were screened in the first phase of the study. shows age and sex distribution of the 6,150 persons, comprising 3,017 (49.06%) males and 3,133 (50.94%) females, with a male to female ratio of approximately 1:1. The ages of the respondents ranged from 1 month to 103 years (mean 29.4±20.8 years). Those aged less than 45 years were 75.27% of the screened population, while those aged above 45 years comprised 24.73% of the population.
Table 1 Age and sex distribution of the 6,150 persons screened
A total of 20 persons were recruited for the second phase (post-stroke-specific questionnaire) of the study. They were made up of ten subjects and ten controls that were matched for age and sex. The mean age of subjects was 60.7±11.4 years (range 47–86 years), while the mean age of controls was 60.4±11.9 years (range 45–84 years). There was no statistical significance between the age of the subjects and that of controls (P=0.853).
Prevalence of stroke
shows that the crude prevalence at the time of the survey on January 14, 2011 (point prevalence) of stroke was 1.63 (95% CI 0.78–3.00) per 1,000 population. The peak age-specific prevalence of stroke was found to be 1.0 (95% CI 0.33–2.33) when age-adjusted per 1,000 WHO world population. It also showed a higher crude prevalence of stroke in males of 1.99 (95% CI 0.73–4.33) per 1,000 than in females, which was 1.28 (95% CI 0.35–3.28) per 1,000 population (relative risk =1.55; P=0.44).
Table 2 Sex-specific, age-specific, and age-adjusted (WHO World Population) prevalence of stroke
Discussion
Previous studies in both developed and developing countries have reported crude prevalence of stroke ranging from 0 to 10.2 per 1,000 population, and the burden of stroke has also been projected to be on the rise.Citation3,Citation6 The crude prevalence of stroke in this study was comparatively higher than reported in previous community-based studies in Nigeria (1.63 versus 1.14, 0.58, and 0.68 per 1,000)Citation4,Citation6,Citation8 but lower than reported in Aiyete, Southwestern Nigeria (4.43 per 1,000).Citation9 Furthermore, we standardized our results to the WHO World Standard Population to compare better with data from other studies. In those aged above 7 years, our study’s age-adjusted prevalence remained higher than those of Danesi et alCitation6 and Osuntokun et alCitation4 (1.70 versus 1.10 and 0.53 per 1,000 population, respectively). Apart from the Danesi et al study, which was conducted less than one decade ago, all the other Nigerian studies were done more than two decades ago. However, unlike ours and the earlier Nigerian studies which were conducted in predominantly low-income rural communities, Danesi et al’s study was conducted in a mixed-income, urban community. Also, the proportion of the population at particular risk for stroke (45 years and above) was higher in our study than that of Danesi et al (24.73% versus 15.24%).Citation6 This may be partly explained by the common practice in Nigeria of urban to rural migration after retirement of about 67% of retirees.Citation10
Furthermore, our results were compared with other populations as detailed in . In a rural South African survey, the age-adjusted prevalence among populations aged above 15 years was higher than ours (3.3 versus 1.90 per 1,000).Citation11 Also, an Asian study in urban Singapore reported a higher age-adjusted prevalence than ours in the population aged 65 years and above (6.31 versus 0.40 per 1,000).Citation12 Nonetheless, the study in urban Nigeria when compared with ours showed a lower age-adjusted prevalence in the population 15 years and above of 1.10 per 1,000 but a higher age-adjusted prevalence of 1.99 per 1,000 in the population 65 years and above.Citation6 The small population size of our study, as is common in many Sub-Saharan African studies, makes it difficult to give statistical interpretation to these differences with certainty.
Table 3 Characteristics of stroke prevalence studies compared with this study
The mean age for stroke obtained in this study is comparable to hospital-based data reported by Owolabi et alCitation13 and Ogun et alCitation14 in Southwestern Nigeria (60.7 versus 59.4 and 61.5 years, respectively). However, our result was lower than the mean age for stroke reported by Danesi et alCitation6 of 63.4 years, although their peak age-adjusted prevalence for stroke was also higher than ours at 1.11 (75–84 years age group) versus 1.00 (55–64 years age group) per 1,000 population, respectively. The low mean age for stroke has been variously attributed to the lower life expectancy and high prevalence of fatal stroke in developing countries.Citation14,Citation15 The mean ages and peak prevalence for stroke in developed countries have been reported to be higher than those of developing countries.Citation13 Also, the male preponderance of stroke noted in our study is comparable to data obtained in Sub-Saharan African studies.Citation3,Citation6,Citation11,Citation16
Conclusion
The interpretative challenges experienced with variations in prevalence data from different communities notwithstanding, the prevalence of stroke is higher than previously reported in rural Nigeria. However, the study site is rural, with inhabitants predominantly of low socioeconomic status and a relatively higher proportion of the population being at risk of stroke. These are factors that may potentially affect the prevalence of stroke in the community.
We acknowledge the limitations of our study, as a larger population size would have been more representative; however, this is a modest attempt in our predominantly low income setting to assess the current prevalence of stroke in Nigeria. A longitudinal register is being kept to ascertain the current incidence of stroke in our study population. More studies to define the risk factors for stroke are recommended.
Supplementary material
Figure S1 Modified World Health Organization questionnaire for detecting neurological diseases.
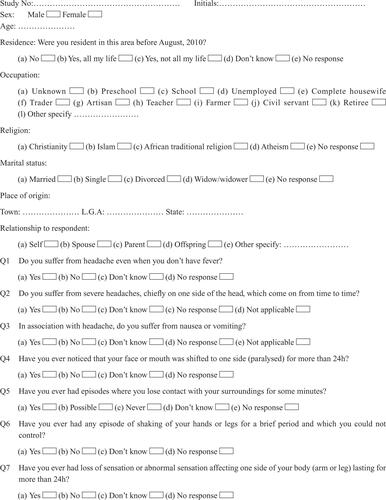
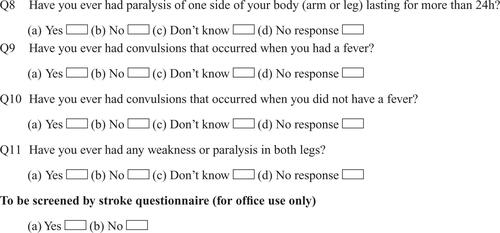
Figure S2 Stroke-specific questionnaire used in Stage II of the study.
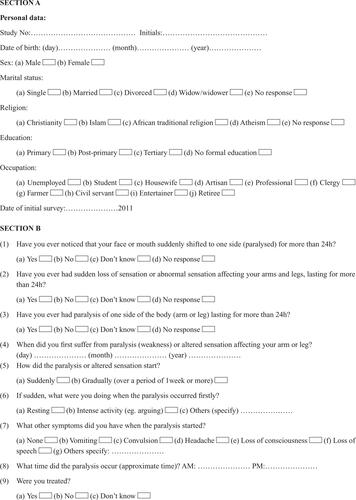
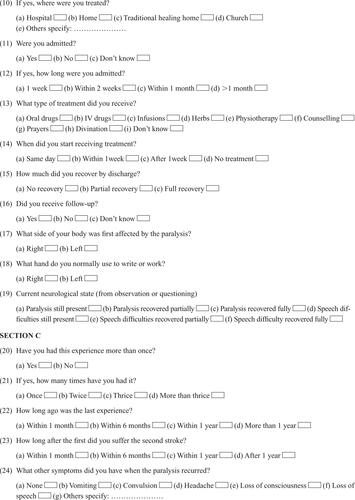
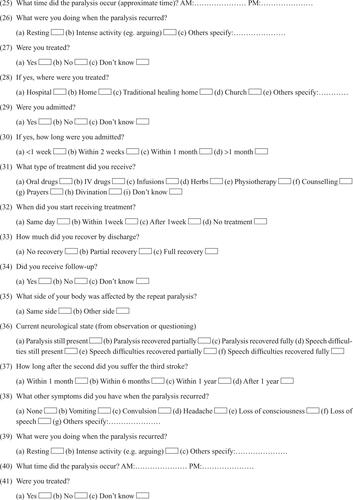
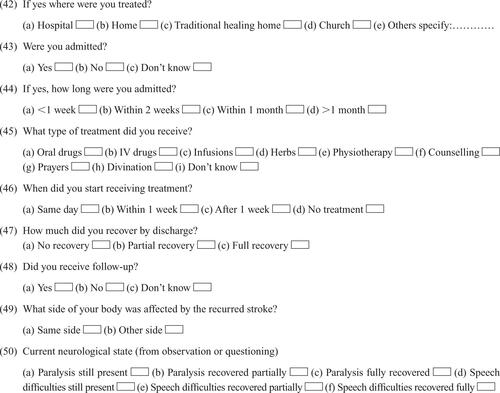
Figure S3 Risk factors for stroke questionnaire used in Stage II of the study.
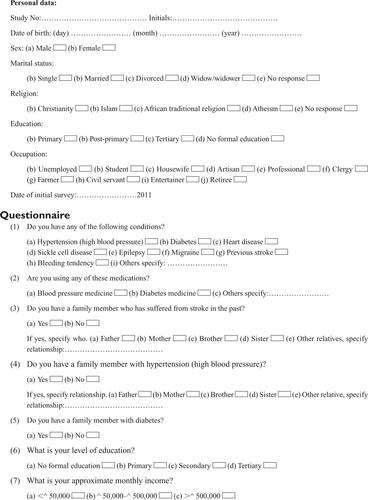
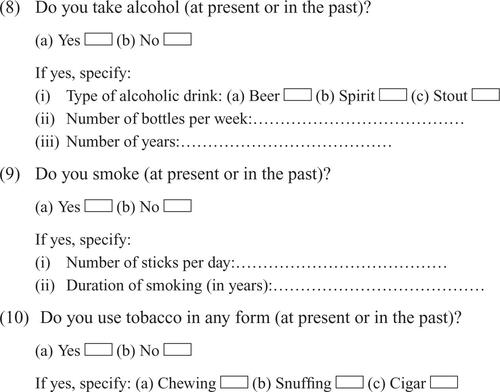
Figure S4 Clinical examination findings (Proforma).
Abbreviations: LDL, low density lipoprotein; HDL, high density lipoprotein; Hb, hemoglobin; WBC, white blood cells.
Disclosure
The authors report no conflicts of interest in this work.
References
- AshrafianHFamilial stroke 2700 years agoStroke2010414e18720185778
- National Institute of Neurological Diseases and Stroke; Stroke: Hope Through Research2004 NIH Publication No 99-2222 Available at http://www.ninds.nih.gov/disorders/stroke/detail_stroke.htmAccessed May 8, 2014
- FeiginVLLawesCMBennettDAAndersonCSStroke epidemiology: a review of population-based studies of incidence, prevalence and case-fatality in the late 20th centuryLancet Neurol20032435312849300
- OsuntokunBOAdeujaAOSchoenbergBSNeurological disorders in Nigerian Africans: a community based studyActa Neurol Scand19877513213033973
- OsuntokunBOBademosiOAkinkugbeOOOyediranABCarlisleRIncidence of stroke in an African city: results from the stroke registry at Ibadan, Nigeria,1973–1975Stroke197910205207442145
- DanesiMOkubadejoNOjiniFPrevalence of stroke in an urban, mixed-income community in Lagos, NigeriaNeuroepidemiology20072821622317851261
- AhmadOEBoschi-PintoCLopezADMurrayCJLLozanoRInnoueMAge Standardization of Rates: a New WHO StandardGPE Discussion Paper Series No 31GenevaWorld Health Organization2001 Available from: http://www.who.int/healthinfo/paper31.pdfAccessed April 7, 2014
- LongeACOsuntokunBOPrevalence of neurological disorders in Udo, a rural community in Southern NigeriaTrop Geogr Med19894136402763344
- OsuntokunBOSchoenbergBSNottidgeVAResearch protocol for measuring the prevalence of neurologic disorders in developing countriesNeuroepidemiology198213143153
- AdeboGMSekumadeABSocio-economic influence of retiree’s migration on rural development in Ekiti State, NigeriaInt J Humanit Soc Sci2012212164172
- ConnorMDThorogoodMCasserlyBDobsonCWarlowCPSASPI Project TeamPrevalence of stroke survivors in rural South Africa: results from the Southern Africa Stroke Prevention Initiative (SASPI) Agincourt field siteStroke20043562763214963282
- VenketasubramanianNTanLCSahadevanSChinJJPrevalence of stroke among Chinese, Malay and Indian Singaporeans: a community-based tri-racial cross-sectional surveyStroke20053655155615692124
- OwolabiMOUgoyaSPlatzTRacial disparity in stroke risk factors: the Berlin-Ibadan experience: a retrospective studyActa Neurol Scand2009119818718638038
- OgunSAOjiniFIOgungboBKolapoKODanesiMstroke in South West Nigeria: a 10-year reviewStroke2005366112122
- OnwuekweIOEzeala-AdikaibeBAOhaegbulamSCChikaniMCAmutaJUlohHNStroke mimics – a study of CT images in Nigerian African stroke patientsJ Neurol Sci Turk2008253148154
- AmuEOgunrinODanesiMReappraisal of risk factors for stroke in Nigerian Africans – a prospective case-control studyAfr J Neurol Sci200522027