Abstract
Angiogenesis inhibitors may provide a new approach to the treatment of metastatic breast cancer. Bevacizumab is a monoclonal antibody against pathologic angiogenesis. A pivotal study (ECOG 2100) showed that bevacizumab in combination with paclitaxel increased progression-free survival for patients with metastatic breast cancer by 6 months. Subsequently, several clinical trials have shown that the combination of bevacizumab with a taxane can improve disease-free survival but does not prolong overall survival. While generally well tolerated, bevacizumab is potentially toxic for some patients who develop hypertension, proteinuria, bleeding, impaired wound healing, bowel perforation or thromboembolic events. Here, we review the current evidence for the use of bevacizumab in breast cancer and ongoing studies that address the questions of how to optimize regimens and schedules for the use of anti-angiogenic agents and the identification of those patients who would benefit the most from treatment with regimens that include antiangiogenic therapy.
Introduction
The umbilical vessels join on the uterus like the roots of plants and through them the embryo receives its nourishment.
– Aristotle, On the Generation of Animals, ca. 340 B.C.
Breast cancer remains the most common cancer among women and the second leading cause of cancer deaths in women. Globally, there are an estimated 4.4 million women alive who have been diagnosed with breast cancer within the last 5 years. Approximately 30% of women with earlier stages of breast cancer will eventually progress to metastatic disease.Citation1 Women with aggressive basal subtype or triple negative cancers (negative estrogen receptors, negative progesterone receptors and HER2 negative) are at particularly high risk of developing metastases even when they present at early stages.Citation2,Citation3 As large numbers of women are living with metastatic breast cancer (MBC) for longer periods of time, the need for clinical trials programs and services for this population is becoming increasingly important. Despite advances in breast cancer therapeutics and drug development, it remains difficult to adequately predict whether patients will even respond at all to treatment and which MBC patients will respond to specific regimens. Angiogenesis inhibitors provide new possibilities for the treatment of women.
Angiogenesis (from the Greek angeion meaning vase and genesis meaning birth) is defined as the outgrowth of new blood vessels from pre-existing vessels. The term angiogenesis was first used in the 1700s by John Hunter to describe blood vessel growth in reindeer antlers in response to cold exposure.Citation4 Angiogenesis was later used to describe the formation of new vessels in the placenta and developing embryo of monkeys by Arthur Hertig in 1935.Citation5 In the 1940s, Algire and Chalkeley at the National Cancer Institute observed that blood vessels migrate toward tumors in wound chambers, demonstrating that tumors actively attract new blood vessels.Citation6
Dr Judah Folkman at Harvard Medical School was the first to postulate that the process of tumor angiogenesis could potentially be targeted for cancer treatment.Citation7 The first angiogenesis inhibitor was identified in cartilage by Brem and Folkman in 1971.Citation8 Using the rabbit cornea as an assay, they demonstrated that a cartilage implant decreased the rate of capillary growth, induced by tumor, by an average of 75%.
In 1989, Napoleone Ferrara and Jean Plouet discovered a growth factor for vascular endothelial cells in conditioned media they named vascular endothelial growth factor (VEGF).Citation9 VEGF was later demonstrated to be identical to a factor in tumor ascites that rapidly increased microvascular permeability, identified by Dr Harold Dvorak in 1983 as vascular permeability factor (VPF).Citation10
Elevated levels of VEGF were observed in solid tumors and correlated with worse clinical outcomes. Ultimately, angiogenesis became recognized as an essential step in tumor growth and metastasis.Citation11 Antiangiogenesis has provided exciting possibilities for cancer treatment and in 2004 the United States Food and Drug Administration (FDA) Commissioner Mark McClellan pronounced antiangiogenic therapy “the fourth modality for cancer treatment”, establishing that this therapy was potentially as important as surgery, chemotherapy and radiation in the treatment of cancer.
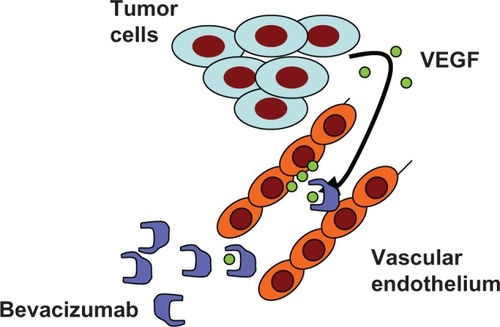
Bevacizumab (Avastin®) was developed as a monoclonal antibody against all isoforms of VEGF-A, which is the isoform responsible for pathologic angiogenesis.Citation12,Citation13 The original mouse monoclonal antibody that was most effective in neutralizing VEGF was then humanized using recombinant technology ().
Figure 1 Tumor cells secrete various isoforms of VEGF in a paracrine fashion. VEGFs stimulate the growth, division and permeability of vascular endothelial cells through interaction with cellular VEGF-receptors (VEGFR1 and VEGFR2). This process of neovascularization can be disrupted by the neutralizing humanized monoclonal antibody bevacizumab.
The efficacy of bevacizumab has been shown in colorectal cancer,Citation14 non-small-cell lung cancer (NSCLC)Citation15,Citation16 renal cancer and ovarian cancer.Citation17,Citation18 Clinically, bevacizumab has been investigated in combination with a range of chemotherapeutic agents, and the pharmacokinetics and toxicities have generally been non-overlapping. Bevacizumab is currently approved in the US for the treatment of NSCLC in combination with paclitaxel and carboplatin, based on the outcome of ECOG (Eastern Cooperative Oncology Group) E4599.Citation16 Bevacizumab is also approved for the first-line treatment of patients with MBC in combination with paclitaxel, based on ECOG 2100;Citation19 and in metastatic colorectal cancer in combination with irinotecan and 5-fluorouracil/leucovorin.Citation20 In addition to metastatic lung and colorectal cancer, bevacizumab was recently also approved for the treatment of metastatic renal cell cancer, based on the results of the Avastin + Interferon vs Placebo + Interferon (AVOREN) trial. The AVOREN study showed an increase in progression-free survival (PFS) for renal cancer patients who received bevacizumab plus interferon alpha, compared to patients who were treated with interferon alpha alone.Citation21 Additionally, the FDA granted approval for the use of single agent bevacizumab for the treatment of recurrent glioblastoma multiforme, based on two single arm studies.Citation22,Citation23 While the approvals in lung and colorectal cancer were based on an improved overall survival with bevacizumab,Citation16,Citation20 the approvals in metastatic renal and breast cancer as well as in glioblastoma were based on an improvement in progression-free survival.
Bevacizumab is being studied worldwide in more than 300 clinical trials and in more than 20 different tumor types, leading to high expectations for its potential to help conquer breast cancer as well.
Pharmacology and pharmacokinetics
The crucial step in neo-vascularization is the “angiogenic switch”,Citation24 which allows tumors to usurp the growth mechanisms of normal vascular endothelial cells and develop to macroscopic size. This process is mediated by the interaction of VEGFs with their membrane-bound receptors (VEGF-Rs).
To date, there are 6 known VEGFs (A, B, C, D, E and placental growth factor) that bind and activate 3 different endothelial cell-bound receptor-tyrosine kinases (VEGFR-1, -2 and -3). Best examined in the context of tumor angiogenesis is VEGF-A, which is expressed in 6 differentially spliced isoforms that bind both VEGFR-1 (flt) and VEGFR-2 (flk), and that stimulate the proliferation of endothelial cells as well as increase the permeability of vasculature.Citation25,Citation26
Upregulation of VEGF expression is a hallmark of many tumors, including invasive ductal carcinomas of the breast,Citation27,Citation28 and has been closely linked to expression of other growth factors such as TNF-α, EGF, insulin, insulin-like growth factor 1 and estrogen.Citation12,Citation29In vitro VEGF secretion is increased upon loss of the tumor suppressor p53 or amplification of oncogenes such as HER2.Citation30,Citation31
Therapeutic disruption of tumor neo-vascularization has been achieved in two ways. Firstly, the VEGFs can be neutralized by using bevacizumab, which recognizes all isoforms of human VEGF,Citation32 thereby eliminating the ligands required for VEGFR activation and the mitogenic and permeability-enhancing stimuli necessary for neo-vascularization. Secondly, the signal transduction cascade downstream from VEGFRs can be disrupted by using the small molecule inhibitors sorafenib and sunitinib.Citation32
Given that bevacizumab is a monoclonal antibody, it is distributed to highly perfused areas with a linear kinetic profile. The terminal elimination half-life of bevacizumab is measured in weeks.Citation33 Currently, recommended dosing is 10 mg/kg every 2 weeks, for complete suppression of serum VEGF.Citation34,Citation35
Efficacy in clinical trials
One of the first trials of bevacizumab in breast cancer was a phase 1 and 2 trial of 75 patients with previously treated metastatic breast cancer.Citation36 In this study bevacizumab monotherapy resulted in an overall response rate of 9.3%; 17% of patients had a response or were stable at 22 weeks. The treatment toxicity of bevacizumab monotherapy was low and differed from toxicity profiles of classical cytotoxic therapies, which lent support for subsequent trials in metastatic breast cancer combining bevacizumab with chemotherapy.Citation36
Given these findings, a phase 3 trial to look at the addition of bevacizumab to capecitabine (Xeloda®) was undertaken, also in pretreated breast cancer patients.Citation37 The combination of bevacizumab with capecitabine in patients with previously treated metastatic cancer demonstrated a significant increase in the response rate from 9.1% to 19.8%, but PFS and overall survival did not improve.Citation37 Unfortunately, the improvements in response appeared to be short-lived.
Following this, two major trials, the ECOG 2100 and the Avastin and Docetaxel (AVADO) trials were designed to look at the addition of bevacizumab to a taxane. The ECOG trial 2100 employed paclitaxel and the AVADO trial docetaxel. The truly pivotal study for metastatic breast cancer was ECOG 2100.Citation19 ECOG 2100 compared paclitaxel alone with paclitaxel plus bevacizumab as initial treatment in a multi-institutional randomized phase 3 trial of 722 patients with metastatic breast cancer. The paclitaxel was given weekly, with biweekly bevacizumab at 10 mg/kg dosing. Results showed that the median progression free survival (PFS) was increased from 6.7 to 13.3 months with the addition of bevacizumab, resulting in a 52% reduction in the risk of disease progression (P < 0.0001). The study was stopped early, following a recommendation of the Independent Data Monitoring Committee. However, despite the improvement in disease-free survival, bevacizumab did not prolong overall survival.Citation38
Simultaneously, the AVADO study investigated the efficacy of bevacizumab in addition to standard first-line treatment of metastatic breast cancer with docetaxel. This study has a 3-arm design, with all patients receiving docetaxel at 100 mg/m2, in combination with either placebo, bevacizumab at 7.5 mg/kg or 15 mg/kg respectively every 3 weeks. A total of 736 patients with metastatic breast cancer were enrolled internationally, and the findings were presented at a median follow-up of 11 months at the 2008 ASCO meeting.Citation39 The study showed that the median time to disease progression was 8 months with docetaxel alone, 8.7 months with docetaxel plus low-dose bevacizumab, and 8.8 months with docetaxel plus high-dose bevacizumab. Thus, while the addition of bevacizumab to docetaxel did not appear to add significantly to the treatment toxicity, the magnitude of the benefit that bevacizumab added to treatment with docetaxel appeared to be much lower then the benefit observed in combination with weekly paclitaxel (ECOG 2100). After a median follow-up of 11 months, the AVADO trial showed a statistically significant difference in overall response rate and PFS overall; the high dose had better efficacy than the low dose.Citation39 Mature data after a median follow up of 25 months confirmed the improvement in PFS and overall response rate, but no difference in overall survival.Citation40
Based on promising results of ECOG 2100 and the AVADO studies, both of which showed improvements in progression free survival, the FDA approved bevacizumab, in combination with paclitaxel, as a treatment of HER2-negative metastatic breast cancer in February 2008. Bevacizumab was approved for patients with advanced breast cancer under the FDA’s accelerated approval program, which allows the FDA to approve products for cancer or other life-threatening diseases based on initial positive clinical data. This decision was somewhat unexpected as a previous FDA advisory committee had recommended against approval.
The FDA approval allowed the next set of trials to proceed. The Avastin + Chemotherapy vs Placebo + Chemotherapy (RiBBON) trials are large multicenter, randomized phase 3 studies that are being conducted to examine the impact of bevacizumab in combination with standard first line chemotherapy regimens for metastatic breast cancer.Citation41,Citation42 The RiBBON 1 trial enrolled patients with previously untreated metastatic breast cancer while the RiBBON 2 trial enrolled those with previously treated metastatic disease.
In the RiBBON 1 trial (AVF3694 g) patients were randomized to receive bevacizumab plus chemotherapy or placebo plus chemotherapy. RiBBON-1 is a global, double-blind, randomized phase III trial with 1,237 patients in 22 countries who did not receive previous chemotherapy for their HER2-negative metastatic breast cancer. RiBBON-1 evaluated bevacizumab with different types of chemotherapies in patients with advanced HER2-negative breast cancer. One group received capecitabine in combination with bevacizumab, the other taxane- or anthracycline-based chemotherapy. Bevacizumab was administered at 15 mg/kg dose every 3 weeks. The median follow-up was 15.6 months in the cohort that received capecitabine and 19.2 months in the cohort that received a taxane and anthracycline. This resulted in a statistically significant improvement in progression free survival. While there was a modest increase in progression-free survival (from 6.2 to 9.8 months in the capecitabine arm, and from 8.3 to 10.7 months in the taxane/anthracycline arm), there was again no significant benefit for overall survival in the RiBBON study, as reported at the 2009 ASCO meeting.Citation41,Citation42 A full review of both the AVADO and RiBBON I data by the FDA will be required for the accelerated approval to be converted into a full approval.
The investigation of the best use of bevacizumab is ongoing. Given its efficacy in combination with chemotherapy, and its likely function as an enhancer of the treatment efficacy rather than an independent agent, bevacizumab is currently under investigation in combination with a range of chemotherapeutic agents. Current trials are being conducted to examine the impact of bevacizumab in combination with standard first line chemotherapy regimens for metastatic breast cancer. The most promising combination, paclitaxel in combination with bevacizumab, is currently being investigated in the adjuvant setting (ECOG 5103) for patients with early-stage HER2-negative breast cancer. This phase 3 trial began enrollment in November 2007 and 3,487 of the planned 4,950 patients have been enrolled to date.
A second area of intense interest is whether bevacizumab increases the activity of targeted agents in breast cancer. Combining small molecule tyrosine kinase inhibitors with bevacizumab is being explored ().Citation43 Of particular importance are combinations with trastuzumab in HER2-positive breast cancer as erbB2 amplification has been shown to increase VEGF secretion by breast cancer cells.Citation44
Table 1 Bevacizumab combinations with targeted agents currently under investigation
Toxicity
Because bevacizumab is a humanized monoclonal antibody, allergic reactions necessitating discontinuation of the drug are relatively infrequent.Citation45 The most common toxicities of bevacizumab are hypertension and proteinuria.Citation20,Citation46 The hypertension is due to a decrease in endothelial nitric oxide synthase activity, resulting in lower nitric oxide levels which lead to vasoconstriction and elevated blood pressure. Treatment for hypertension is instituted before starting bevacizumab.Citation47 Once the patient is receiving bevacizumab, blood pressure should be monitored closely and appropriate antihypertensive therapy instituted if hypertension occurs or worsens. Interestingly, development of hypertension during treatment with bevacizumab may serve as prognostic factor for clinical outcome in patients receiving bevacizumab.Citation47 However, patients who develop hypertension are also at risk for proteinuria, which can develop into the nephrotic range, necessitating discontinuation of the bevacizumab.
Other common side effects include bleeding, problems with wound healing, bowel perforation and serious arterial thromboembolic events, including transient ischemic attack, cerebrovascular accident, angina, and myocardial infarction. Most of the bevacizumab-associated bleeding is epistaxis which is easily controlled.Citation20 However, serious hemoptysis has been reported in patients receiving bevacizumab for metastatic non-small-cell lung carcinoma.Citation15 Bevacizumab should not be used in patients receiving full dose anticoagulation or with a history of a bleeding diathesis.Citation45
Bevacizumab has been associated with delayed wound healing, as well as dehiscence, ecchymosis, surgical site bleeding, and wound infection.Citation48 Elective surgery should be postponed until at least 40 days after the cessation of bevacizumab. Postoperative re-initiation of bevacizumab should not take place until the surgical incision has fully healed and at least 28 days after surgery to prevent increased wound healing complications.
Gastrointestinal perforation has been reported in a small percentage of patients treated with bevacizumab for colorectal cancer.Citation14,Citation49,Citation50 Perforation typically presented with abdominal pain with constipation and vomiting. Gastrointestinal perforations are rare in patients with breast cancer. Even when breast cancer patients have peritoneal implants or a high volume of visceral disease perforations occur in less than 3%.Citation51 Bevacizumab should be permanently discontinued in patients who develop gastrointestinal perforation.
Serious arterial and venous thromboembolic events have been reported in patients receiving bevacizumab. Patients at highest risk of arterial thromboembolic events are those with a prior history of an arterial thrombotic event and patients over the age of 65. Bevacizumab should be permanently discontinued in patients who develop thrombotic events during treatment.
There has been concern that bevacizumab would cause hemorrhagic complications in patients with brain metastases. However, a recent analysis of several hundred patients with brain metastases who had received bevacizumab showed that the administration of bevacizumab did not significantly affect the risk of intracranial hemorrhage for patients with brain metastases from epithelial cancers.Citation52 In fact, the combination of avastin with carboplatinum is currently under investigation as a potentially active regimen in women with brain metastases from breast cancer (NCT01004172).
Less common complications include osteonecrosis of the jaw and reversible posterior leukoencephalopathy syndrome (RPLS). RPLS may be associated with hypertension and symptoms include headache, seizure, lethargy, confusion, blindness, and other visual and neurologic disturbances.Citation53,Citation54 It usually resolves with discontinuation of bevacizumab and control of any associated hypertension. Osteonecrosis of the jaw is significantly increased in patients receiving bevacizumab in conjunction with bisphosphonates.Citation55,Citation56
Toxicities can be more frequent when bevacizumab is used in combination with chemotherapy or in the neo-adjuvant setting.Citation57 In a pre-operative study of cisplatin and bevacizumab, 37% of the patients with triple-negative breast cancer achieved a Miller-Payne 4 or 5 remission. However 11% of the patients could not complete the treatment due to toxicities, including hypertension, pulmonary embolus and tinnitus or hearing loss. Additionally, this treatment combination led to significant rates of surgical complications, including wound breakdown, implant loss, hematomas and persistent seromas.Citation58
Conclusions
A common theme in all combinations that included bevacizumab in breast cancer is that addition of the anti-VEGF antibody improves overall response rates and delays time to progression, but does not improve overall survival and does not seem to alter the course of the disease as dramatically as trastuzumab does in HER2-positive breast cancer. This points to the need to identify those patients who may benefit the most from this potentially toxic and costly treatment. Validated biomarkers for selecting cancer patients that should be considered for antiangiogenic therapy are needed.Citation59 Potential biomarkers such as VEGF polymorphisms or treatment responses such as hypertension, circulating angiogenic molecules or collagen IV all have some promise of helping to predict benefit and/or toxicity.
In the search for valid biomarkers, urine VEGF levels, tumor VEGF and thrombospondin 2 expressionCitation38 as well as mutations in p53 and Ras were not predictors of response to bevacizumab.Citation60,Citation61 However, in a retrospective analysis of ECOG2100, the presence of a germline single nucleotide polymorphism in the 5-prime untranslated region of VEGF-A, −2578AA and −1154AA showed a correlation with overall improved survival, as did the presence of greater than grade 2 hypertension.Citation62 Whether the differences in treatment outcomes are large enough to warrant stratification of patients according to these criteria, however, will need to be clarified in further studies.
Another unresolved, yet highly pressing issue is the emergence of resistance to antiangiogenic therapy, as almost all patients will eventually progress on bevacizumab, even if they achieved an initial response. In contrast to trastuzumab, which is continued even when chemotherapeutic agents are changed to address disease progression, there are no data to support the continued use of bevacizumab after disease progression. Indeed, a note of caution comes from recent laboratory observations about the prolonged use of angiogenesis inhibitors at a point of disease progression, and the use of PFS as an endpoint for the evaluation of angiogenesis inhibitors. While tumor-bearing mice treated with angiogenesis inhibitors experienced tumor shrinkage, their survival was reduced, and tumor invasiveness and metastasis were actually enhanced, leading to hypotheses that angiogenesis inhibition might facilitate the extravasation of tumor cells into a metastatic site or promote the creation of metastatic niches.Citation63,Citation64
The field of angiogenesis inhibitors for the treatment of breast cancer is young, and bevacizumab is currently under investigation internationally in over 100 clinical trials for all subtypes of stage II through IV breast cancer, mostly in combination with classical chemotherapy or newly developed targeted agents. Further validation of genetic biomarker profiles will likely aid in developing models to predict which patients will experience improved survival as a result of a bevacizumab-containing regimen.
Acknowledgments/disclosures
The authors report no conflicts of interest in this work.
References
- BRIDGE: Bridging Gaps, Expanding Outreach For Metastatic Breast Cancer PatientsBreast200918527327519616435
- JangGLeeSAhnJClinical features and course of brain metastases in triple-negative breast cancer: Comparison with HER2+ and other typeJ Clin Oncol20092715s Suppl
- ScruggsKPradhanSMMfalilaCDifferential timing and patterns of recurrence among breast cancer subtypesJ Clin Oncol20092715s Suppl
- KoblerJThe reluctant surgeon A biography of John HunterGarden City, New YorkDoubleday & Company, Inc.1960
- HertigAAngiogenesis in the early human chorion and in the primary placenta of the macaque monkeyContr Embryol Carnegie Inst1935253781
- AlgireGHC HWLegallaisFYParkHDVascular reactions of normal and malignant tumors in vivo. I. Vascular reactions of mice to wounds and to normal and neoplastic transplantsJ Natl Cancer Inst194567385
- FolkmanJTumor angiogenesis: therapeutic implicationsN Engl J Med197128521118211864938153
- BremHFolkmanJInhibition of tumor angiogenesis mediated by cartilageJ Exp Med197514124274391113064
- FerraraNHenzelWJPituitary follicular cells secrete a novel heparin-binding growth factor specific for vascular endothelial cellsBiochem Biophys Res Commun198916128518582735925
- SengerDRGalliSJDvorakAMTumor cells secrete a vascular permeability factor that promotes accumulation of ascites fluidScience198321945879839856823562
- CulyCBevacizumab: antiangiogenic cancer therapyDrugs Today (Barc)2005411233615753967
- FerraraNGerberHPLeCouterJThe biology of VEGF and its receptorsNat Med20039666967612778165
- DvorakHFVascular permeability factor/vascular endothelial growth factor: a critical cytokine in tumor angiogenesis and a potential target for diagnosis and therapyJ Clin Oncol200220214368438012409337
- SaifMWMerrittJRobbinsJPhase III multicenter randomized clinical trial to evaluate the safety and efficacy of CoFactor/5-fluorouracil/bevacizumab versus leucovorin/5-fluorouracil/bevacizumab as initial treatment for metastatic colorectal carcinomaClin Colorectal Cancer20066322923417026795
- JohnsonDHFehrenbacherLNovotnyWFRandomized phase II trial comparing bevacizumab plus carboplatin and paclitaxel with carboplatin and paclitaxel alone in previously untreated locally advanced or metastatic non-small-cell lung cancerJ Clin Oncol200422112184219115169807
- TyagiPBevacizumab, when added to paclitaxel/carboplatin, prolongs survival in previously untreated patients with advanced non-small-cell lung cancer: preliminary results from the ECOG 4599 trialClin Lung Cancer20056527627815845177
- AghajanianCThe role of bevacizumab in ovarian cancer – an evolving storyGynecol Oncol2006102213113316846774
- MonkBJChoiDCPugmireGBurgerRAActivity of bevacizumab (rhuMAB VEGF) in advanced refractory epithelial ovarian cancerGynecol Oncol200596390290515721449
- GrayRBhattacharyaSBowdenCIndependent review of E2100: a phase III trial of bevacizumab plus paclitaxel versus paclitaxel in women with metastatic breast cancerJ Clin Oncol200927304966497219720913
- HurwitzHFehrenbacherLNovotnyWBevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancerN Engl J Med2004350232335234215175435
- EscudierBPluzanskaAKoralewskiPBevacizumab plus interferon alfa-2a for treatment of metastatic renal cell carcinoma: a randomised, double-blind phase III trialLancet200737096052103211118156031
- FriedmanHSPradosMDWenPYBevacizumab alone and in combination with irinotecan in recurrent glioblastomaJ Clin Oncol200927284733474019720927
- KreislTNKimLMooreKDuicPRoyceCStroudIPhase II trial of single-agent bevacizumab followed by bevacizumab plus irinotecan at tumor progression in recurrent glioblastomaJ Clin Oncol200927574074519114704
- HanahanDFolkmanJPatterns and emerging mechanisms of the angiogenic switch during tumorigenesisCell19968633533648756718
- FerraraNVascular endothelial growth factor as a target for anticancer therapyOncologist20049Suppl 121015178810
- AchenMGJeltschMKukkEVascular endothelial growth factor D (VEGF-D) is a ligand for the tyrosine kinases VEGF receptor 2 (Flk1) and VEGF receptor 3 (Flt4)Proc Natl Acad Sci U S A19989525485539435229
- WeidnerNFolkmanJPozzaFTumor angiogenesis: a new significant and independent prognostic indicator in early-stage breast carcinomaJ Natl Cancer Inst19928424187518871281237
- WeidnerNSempleJPWelchWRFolkmanJTumor angiogenesis and metastasis – correlation in invasive breast carcinomaN Engl J Med19913241181701519
- ShweikiDItinANeufeldGGitay-GorenHKeshetEPatterns of expression of vascular endothelial growth factor (VEGF) and VEGF receptors in mice suggest a role in hormonally regulated angiogenesisJ Clin Invest1993915223522437683699
- RakJYuJLKlementGKerbelRSOncogenes and angiogenesis: signaling three-dimensional tumor growthJ Investig Dermatol Symp Proc2000512433
- LaughnerETaghaviPChilesKMahonPCSemenzaGLHER2 (neu) signaling increases the rate of hypoxia-inducible factor 1alpha (HIF-1alpha) synthesis: novel mechanism for HIF-1-mediated vascular endothelial growth factor expressionMol Cell Biol200121123995400411359907
- HerbstRSTherapeutic options to target angiogenesis in human malignanciesExpert Opin Emerg Drugs200611463565017064223
- LinYSNguyenCMendozaJLPreclinical pharmacokinetics, interspecies scaling, and tissue distribution of a humanized monoclonal antibody against vascular endothelial growth factorJ Pharmacol Exp Ther199928813713789862791
- MargolinKGordonMSHolmgrenEPhase Ib trial of intravenous recombinant humanized monoclonal antibody to vascular endothelial growth factor in combination with chemotherapy in patients with advanced cancer: pharmacologic and long-term safety dataJ Clin Oncol200119385185611157039
- HseiVDeguzmanGGNixonAGaudreaultJComplexation of VEGF with bevaczumab decreases VEGF clearance in ratsPharm Res200219111753175612458683
- CobleighMALangmuirVKSledgeGWA phase I/II dose-escalation trial of bevacizumab in previously treated metastatic breast cancerSemin Oncol2003305 Suppl 1611712414613032
- MillerKDChapLIHolmesFARandomized phase III trial of capecitabine compared with bevacizumab plus capecitabine in patients with previously treated metastatic breast cancerJ Clin Oncol200523479279915681523
- MillerKWangMGralowJPaclitaxel plus bevacizumab versus paclitaxel alone for metastatic breast cancerN Engl J Med2007357262666267618160686
- MilesDChanARomieuGRandomized, double-blind, placebo-controlled, phase III study of bevacizumab with docetaxel or docetaxel with placebo as first-line therapy for patients with locally recurrent or metastatic breast cancer (mBC): AVADOJ Clin Oncol200826520 Suppl abstr LBA1011
- MilesDChanARomieuGFinal overall survival (OS) results from the randomized, double-blind, placebo-controlled, phase 3 AVADO study of bevacizumab (B) plus docetaxel (D) complared with placebo (PL) plus D for the first-line treatment of locally recurrent (LR) or metastatic breast cancer (mBC)Cancer Research2010
- O’ShaughnessyJABrufskyAMRiBBON 1 and RiBBON 2: phase III trials of bevacizumab with standard chemotherapy for metastatic breast cancerClin Breast Cancer20088437037318757267
- RobertNDierasVGlaspyJRIBBON-1: Randomized, double-blind, placebo-controlled, phase III trial of chemotherapy with or without bevacizumab (B) for first-line treatment of HER2-negative locally recurrent or metastatic breast cancer (MBC)Journal of Clinical Oncology20092715S (May 20 Suppl), ASCO Annual Meeting Proceedings (Post-Meeting Edition)
- DicklerMNRugoHSEberleCAA phase II trial of erlotinib in combination with bevacizumab in patients with metastatic breast cancerClin Cancer Res200814237878788319047117
- Bagheri-YarmandRVadlamudiRKWangRAMendelsohnJKumarRVascular endothelial growth factor up-regulation via p21-activated kinase-1 signaling regulates heregulin-beta1-mediated angiogenesisJ Biol Chem200027550394513945710967114
- ArriagaYBecerraCRAdverse effects of bevacizumab and their management in solid tumorsSupport Cancer Ther20063424725018632501
- KabbinavarFHurwitzHIFehrenbacherLPhase II, randomized trial comparing bevacizumab plus fluorouracil (FU)/leucovorin (LV) with FU/LV alone in patients with metastatic colorectal cancerJ Clin Oncol2003211606512506171
- PandeALombardoJSpangenthalEJavleMHypertension secondary to anti-angiogenic therapy: experience with bevacizumabAnticancer Res2007275B3465347017972502
- GordonCRRojavinYPatelMA review on bevacizumab and surgical wound healing: an important warning to all surgeonsAnn Plast Surg200962670770919461291
- SaifMWElfikyASalemRRGastrointestinal perforation due to bevacizumab in colorectal cancerAnn Surg Oncol20071461860186917356952
- SaifMWMehraRIncidence and management of bevacizumab-related toxicities in colorectal cancerExpert Opin Drug Saf20065455356616774493
- ChengXMoroneyJWLevenbackCFFuSJaishuenAKavanaghJJWhat is the benefit of bevacizumab combined with chemotherapy in patients with recurrent ovarian, fallopian tube or primary peritoneal malignancies?J Chemother200921556657219933049
- BesseBLasserreSFComptonPHuangJAugustusSRohrUPBevacizumab safety in patients with central nervous system metastasesClin Cancer Res16126927820028762
- MarinellaMAMarkertRJReversible posterior leukoencephalopathy syndrome associated with anticancer drugsIntern Med J2008
- VaughnCZhangLSchiffDReversible posterior leukoencephalopathy syndrome in cancerCurr Oncol Rep2008101869118366965
- AyllonJLaunay-VacherVMedioniJCrosCSpanoJPOudardSOsteonecrosis of the jaw under bisphosphonate and antiangiogenic therapies: cumulative toxicity profile?Ann Oncol200920360060119188135
- ChristodoulouCPervenaAKlouvasGCombination of bisphosphonates and antiangiogenic factors induces osteonecrosis of the jaw more frequently than bisphosphonates aloneOncology200976320921119212145
- RyanPTungNMIsakoffSJNeoadjuvant cisplatin and bevacizumab in triple negative breast cancer (TNBC): Safety and efficacyJ Clin Oncol20092715s Suppl
- GolshanMGarberJGelmanRSurgical complications and the use of neoadjuvant bevacizumabCancer Rese200969Suppl 24496s
- JainRKDudaDGWillettCGBiomarkers of response and resistance to antiangiogenic therapyNat Rev Clin Oncol20096632733819483739
- InceWLJubbAMHoldenSNAssociation of k-ras, b-raf, and p53 status with the treatment effect of bevacizumabJ Natl Cancer Inst2005971398198915998951
- JubbAMHurwitzHIBaiWHolmgrenEBTobinPGuerreroASImpact of vascular endothelial growth factor-A expression, thrombospondin-2 expression, and microvessel density on the treatment effect of bevacizumab in metastatic colorectal cancerJ Clin Oncol200624221722716365183
- SchneiderBPRadovichMMillerKDThe role of vascular endothelial growth factor genetic variability in cancerClin Cancer Res200915175297530219706811
- Paez-RibesMAllenEHudockJTakedaTAntiangiogenic therapy elicits malignant progression of tumors to increased local invasion and distant metastasisCancer Cell200915322023119249680
- EbosJMLeeCRCruz-MunozWBjarnasonGAChristensenJGKerbelRSAccelerated metastasis after short-term treatment with a potent inhibitor of tumor angiogenesisCancer Cell200915323223919249681