Abstract
The humanized antibody efalizumab is currently the only T-cell directed biologic approved for the treatment of moderate-to-severe psoriasis by both American and European authorities. Binding to and blocking the function of the adhesion molecule leukocyte function associated antigen 1 (LFA-1), it is believed to interfere with T-cell activation in the lymph node, migration through the circulation into the skin, and re-activation in-loco, all of these representing central steps in the pathogenesis of psoriasis. A comprehensive clinical development program provided large and consistent evidence that efalizumab induces a major clinical benefit in psoriasis. Efalizumab rapidly and substantially improves psoriatic skin symptoms and leads to profound gain in quality of life. It allows safe and effective long-term control of psoriasis. Therefore, evidence-based treatment guidelines recommend its use in moderate to severe plaque-type psoriasis.
Clinical aspects of psoriasis
Psoriasis is one of the most common dermatological diseases. Although there is a great variation in the prevalence of psoriasis in different countries due to environmental and genetic factors, it can be said that it affects roughly 2%–3% of the world’s Caucasian population. About 20%–25% of these people suffer from joint involvement (psoriatic arthritis).
The disease usually occurs as so-called plaque-type psoriasis, accounting for more than 80% of the cases. Clinical features include sharply demarginated, erythematous plaques with non-adherent, silvery scales. Pain, itching, and cracking of the skin may be prominent as well. These lesions most typically affect elbows, knees, scalp, lumbar, and umbilical areas. Guttate psoriasis is often a form that begins in childhood or early adulthood; it appears as eruption of scattered 1.0–10 mm “drop” shaped, erythematous, scaly papules. Inverse psoriasis is typically localized to the axilla, submammary folds, genitocrural area, and neck. These lesions usually have no scale and appear as well-demarcated, salmon red plaques that can fissure. Palmoplantar psoriasis affects the palms and soles, presenting as discrete, erythematous, scaling patches and plaques. These lesions are usually bilateral, and involvement of the palms typically stops at the wrist-palm junction. The potential of psoriasis to principally affect every site of the body is reflected by the so-called erythrodermic psoriasis, presenting as generalized indurated erythema with diffuse exfoliation of fine scales. The patients may also present with fever, chills, rigors, arthralgias, and trouble maintaining core body temperature. More rarely, pustular types of psoriasis may occur. Additionally, scalp and nails may also be affected. Finally, some 20%–30% of patients develop joint involvement.
Unmet needs in the treatment of psoriasis
Although a wide spectrum of anti-psoriatic therapies is currently available, their application is often limited by numerous factors, including insufficient practicability (topical and phototherapies) and lack of long-term safety (photo- and systemic therapies); some are either not sufficiently effective as a monotherapy (retinoids) or are frequently not tolerated (fumarates). These shortcomings of established anti-psoriatic therapies are reflected in part by poor satisfaction among patients: In a recent survey, only some 25% stated they were satisfied with the treatment successes encountered (CitationStern et al 2004). Besides, non-compliance is high among psoriatic patients (CitationRichards et al 1999). Reasons for dissatisfaction and/or non-compliance comprise poor tolerability and/or efficacy, impracticability, and lack of information on adverse drug reactions.
The impact of psoriasis on physical and mental aspects of life is still widely underestimated, even though numerous studies have documented a high burden of disease comparable to major other entities such as cancer or rheumatoid arthritis (CitationRapp et al 1999). Consequently, improvement of health-related quality of life is an integral part of managing psoriasis.
Biologics, defined as molecular species generated in cell-based systems, have the potential to meet some of the above-mentioned needs (CitationSterry et al 2004). Major trials evaluating biologics in psoriasis have focused on moderate-to-severe plaque-type psoriasis. Measures currently used to document therapeutic efficacy include determination of the affected body surface area (BSA), Psoriasis Area and Severity Index (PASI), and the Dermatology Life Quality Index (DLQI) (CitationStrober et al 2006). In the absence of a precise definition, moderate to severe psoriasis is considered to be characterised by scores >10 in any of these instruments (CitationBoehncke et al 2006a). Treatment success is defined by reduction of the respective scores. Typically, the percentage of patients achieving at least a 75% reduction in the PASI (PASI-75) is considered a good clinical response.
Currently, four biologics are approved for the treatment of plaque-type psoriasis (CitationBoehncke et al 2006b). Whereas alefacept (approved only by the FDA) and efalizumab both interfere with T-cell function, infliximab and etanercept block the pro-inflammatory cytokine TNF-α; the latter three are approved by the US Food and Drug Administration (FDA) as well as the European Medicines Agency (EMEA). Both agencies are expected to approve the use of adalimumab, another TNF-α blocker, in the near future. All biologics mentioned have proven safety and efficacy as well as practicability and improvement of quality of life in double-blind, placebo-controlled, randomized trials.
Subsequently, the rationale for developing efalizumab, its chemistry and pharmacology as well as efficacy and safety will be discussed in detail.
The role of T-cells in the pathogenesis of psoriasis
There is agreement today that immunological mechanisms play an important role in the pathogenesis of many chronic relapsing inflammatory skin diseases, such as psoriasis (CitationKrueger 2002; CitationSchön and Boehncke 2005). Evidence of the pivotal role played by T-cells in the pathology of psoriasis is accumulating, such as
presence of activated T-cells in psoriatic lesions (CitationBjerke et al 1978)
the ability of activated T-cells to induce the altered keratinocyte growth and differentiation pattern typical of psoriasis, as demonstrated in the so-called psoriasis SCID mouse model: Injection of autologous immunoctyes into non-lesional skin grafts from psoriatic donors onto mice with a severe combined immune deficiency results in the phenotype of lesional psoriatic skin (CitationNickoloff and Wrone-Smith 1999)
efficacy of T-cell-targeted immune suppressive drugs, such as cyclosporine, and antibodies against the CD25 receptor and CD4 (CitationSchön and Boehncke 2005)
transfer of psoriasis in the process of bone marrow transplantation from a donor suffering from the disease to a healthy recipient (CitationGardembas-Pain et al 1991). Also, psoriasis can be “cured” when bone marrow is transplanted from a healthy donor to a person with psoriasis (CitationEedy et al 1990).
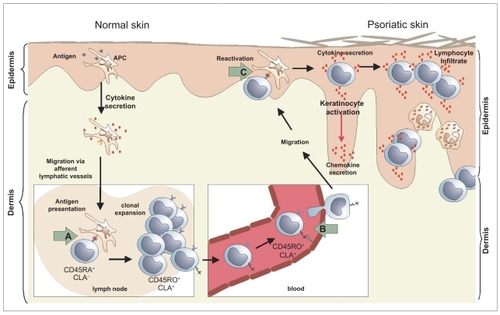
According to a widely accepted working hypothesis on the pathogenesis of psoriasis, antigen-presenting dendritic cells of the epidermis transport yet unknown antigens to regional lymph nodes and present them to naïve T-cells. These respond by activation, proliferation, and maturation into effector T-cells, which patrol the body and leave circulation at the site of antigen contact. Subsequently, these cells migrate toward the epidermis and upon re-activation, release effector molecules, namely pro-inflammatory cytokines, which in turn contribute substantially to the development of the clinically apparent erythemato-squamous plaques ().
Figure 1 Mode of action of efalizumab in psoriasis: According to a widely accepted working hypothesis, antigen-presenting dendritic cells of the epidermis transport yet unknown antigens to regional lymph nodes and present them to naïve T-cells. These respond by activation, proliferation, and maturation into effector T-cells, which patrol the body and leave circulation at the site of antigen contact. Subsequently, these cells migrate toward the epidermis and upon re-activation, release effector molecules, namely pro-inflammatory cytokines. Efalizumab interferes with this process at the LFA-1 dependent stages, namely activation of T-cells in lymph nodes (A), extravazation of circulating T-cells in inflammatory skin (B), and T-cell re-activation in the skin (C).
The role of leukocyte function associated antigen 1 (LFA-1) in the pathogenesis of psoriasis
LFA-1, Mac-1, and p159,95, members of the β2 integrin family, are heterodimeric molecules consisting of a β-subunit (CD18), common to all three molecules, which is non-covalently linked to the respective a-chain CD11a (LFA-1), CD11b (Mac-1), and CD11c (p159,95). T-cells mainly express LFA-1 (CD11a/CD18), which is essential for every step in the process of immune surveillance and mounting an immune response (CitationDustin et al 2004), namely firm adherence to the wall of blood vessels under blood flow, scanning by T cells of other cells within tissues, and formation of the immunological synapse between T-cells and antigen-presenting cells. The ligands for LFA-1 are intercellular adhesion molecules (ICAM). They include ICAM-1, expressed on leucocytes, vascular endothelium cells and epithelial cells, including keratinocytes, ICAM-2 expressed on resting endothelium and lymphocytes and ICAM-3, expressed on monocytes and resting lymphocytes.
Thus, LFA-1 is likely to be involved in numerous crucial steps of the pathogenesis of psoriasis, namely activation of T-cells in lymph nodes upon encounter of antigen transported there by dendritic cells of the epidermis, extravazation of circulating T-cells in inflammatory skin, T-cell re-activation in the skin by antigen-presenting cells, and keratinocyte interaction with infiltrating activated T-cells. Therefore, a function-blocking anti LFA-1 antibody should exhibit anti-psoriatic efficacy based on interference at these points ().
Development and characterization of efalizumab
Efalizumab (Raptiva®, rhuMAb CD11a, hu1124, Genentech, Inc., South San Francisco, CA, USA) is a full-length, IgG1 kappa isotype antibody composed of two identical kappa light chains consisting of 214 amino acid residues, and two gamma heavy chains consisting of 451 residues. Each light chain is covalently coupled through a disulfide link to a heavy chain. The two heavy chains are covalently coupled to each other via inter-chain disulfide bonds consistent with the structure of human IgG1. The molecular weight of intact efalizumab is 148,841 Da.
Originally developed as a murine anti-CD11a monoclonal antibody (MHM24; CitationHildreth and August 1985), efalizumab has been prepared by substituting human DNA sequences using genetic engineering methods to reduce immunogenicity. In detail, complementarity determining regions (CDR) from the murine antibody MHM24 were grafted into consensus human IgG1χ heavy and light chain sequences. This results in a “humanized” mAb (HuIgG1) in which the complementarity-determining regions (CDRs) of the murine antibody – important for specific antigen recognition – are preserved.
Previous studies on murine MHM24 have shown that, similar to other anti-CD11a antibodies, it is able to inhibit T-cell function.
The consensus sequences for the human heavy chain subgroup III (VH-CH1) and the light chain subgroup k 1 were used as the framework for the humanization. Several humanized variants were made and screened for binding as Fabs. To construct the first Fab variant of humanized MHM24, all six CDR residues were transferred from the murine antibody to the human framework.
Further variants were constructed by targeted exchange of either framework residues, or residues within CDRs using the first variant (Fab-1), as a template. For that purpose, both light and heavy chains were completely sequenced for each variant. Plasmids containing the sequences were then transformed to Escherichia coli for protein expression.
All variants were tested for CD11a binding in the Jurkat domains of the variant with optimal cell assay. VL and VH binding characteristics were then transferred to human IgG1 constant domains, giving the full-length intact humanized antibody (CitationWerther et al 1996).
Several in vitro assays were performed to compare efalizumab with its parent murine antibody MHM24, including the keratinocyte cell-adhesion assay and the mixed lymphocyte response assay (MLR).
The results showed that, in these assays, efalizumab worked as well as MHM24. In addition, the apparent Kd values, as determined by saturation binding using peripheral blood mononuclear cells (PBMCs) of two human donors, were similar for both MHM24 and efalizumab (0.16 ± 0.01 nM and 0.13 ± 0.02 nM vs 0.11 ± 0.08 nM and 0.18 ± 0.03 nM, respectively).
Pharmacodynamics
The pharmacodynamic properties of efalizumab were investigated in several phase I and phase II studies following intravenous and subcutaneous administration, either as a single dose or repeated weekly administration.
In the single-dose intravenous study, doses of 0.03–10 mg/kg were given (CitationGottlieb et al 2000). Within 24 hours, treatment with efalizumab reduced the level of CD11a expression on T-cells to 25% of pretreatment levels. This suppression persisted as long as efalizumab was present in the circulation. In the above mentioned study (iv, single dose), CD11a expression returned to baseline within 7–10 days following clearance of efalizumab, without showing any signs of lymphocyte depletion. Total white blood cell (WBC) count was slightly increased within about 8 hours of efalizumab administration; circulating lymphocyte counts were increased by day 7. Following multiple weekly dosing, lymphocytes remained elevated but returned to baseline after efalizumab clearance. This elevation of lymphocyte count is probably due to demargination – blocked entry of efalizumab-bound cells to tissues.
To achieve the full pharmacodynamic effect, intravenous doses of above 0.3 mg/kg were necessary. Complete saturation and maintenance of CD11a binding site down-regulation on lymphocytes required weekly intravenous doses of 0.6 mg/kg, which corresponds to an efalizumab plasma concentration of 5 μg/mL.
Several histological changes were observed in psoriatic plaques following efalizumab administration. A marked reduction of keratin-16, corresponding to decreased disease activity, was noted. Keratinocyte ICAM-1 levels were also reduced, indicating reduced cytokine-mediated inflammation. Furthermore, a significant thinning of the epidermis and restoration of normal skin was observed after 28 days of treatment, in concordance with reductions of over 50% in cutaneous T-cell infiltration and reduced CD11a availability (CitationGottlieb et al 2002). These data demonstrate that by reducing CD11a on the surface of circulating and cutaneous T-cells, efalizumab is able to reverse both the histological signs of inflammation and the pathological hyperplasia characteristic of plaque psoriasis.
In general, the effects of subcutaneous efalizumab on lymphocytes were comparable to those observed after intravenous dosing. Subcutaneous doses of 1 mg/kg/week or above produced the required efalizumab plasma concentrations of 5 μg/mL for binding site down-regulation and saturation. No additional clinical benefits of higher doses (eg, doses of 2 mg/kg/week and 4 mg/kg/week) were observed (CitationGottlieb et al 2002).
In addition to reduced CD11a expression on the surface of CD3+ T-cells, binding of efalizumab also causes a reduced expression of other adhesion molecules, such as CD11b, L-selectin or β7-integrin. The down-modulation of these adhesion molecules likely contributes to the anti-adhesive effects of efalizumab. There is also a decrease of αβ + T-cell receptors and of TCR-associated co-receptors, such as CD4, CD8 or CD2. Inhibition of TCR-mediated activation therefore seems to also play a role in efalizumab mode of action.
Pharmacokinetics
The pharmacokinetic properties of subcutaneous efalizumab were determined in an open, multicenter, phase I study of 70 patients suffering from moderate-to-severe plaque psoriasis. Patients received weekly doses of either 1 mg/kg (n = 33) or 2 mg/kg (n = 37) efalizumab for 12 weeks subcutaneously (CitationMortensen et al 2005).
After subcutaneous administration of efalizumab, peak plasma concentrations are reached after 2–3 days. The average estimated bioavailability was about 50% at the recommended dose level of subcutaneous efalizumab, 1.0 mg/kg/week.
Steady-state serum concentrations of efalizumab were achieved after 4 doses of weekly efalizumab, 1 mg/kg, and after 8 weeks in patients receiving 2 mg/kg. At this dose level (with an initial dose of 0.7 mg/kg in the first week), the mean efalizumab plasma trough values were 9.1 ± 6.7 μg/mL in the 1 mg/kg group and 23.5 ± 12.2 μg/mL in the 2 mg/kg group. The volume of distribution of the central compartment after single intravenous doses was 110 mL/kg at dose 0.03 mg/kg and 58 ml/kg at dose 10 mg/kg.
The metabolism of efalizumab is through internalization followed by intracellular degradation as a consequence of either binding to cell surface CD11a or through endocytosis. The expected degradation products are small peptides and individual amino acids which are eliminated by glomerular filtration. Cytochrome P450 enzymes, as well as conjugation reactions, are not involved in the metabolism of efalizumab.
Efalizumab is cleared by dose-dependent nonlinear saturable elimination (CitationGottlieb et al 2000). Mean steady-state clearance is 24.3 ± 18.5 and 15.7 ± 12.6 mL/kg/day for the 1 mg/kg/week and 2 mg/kg/week groups, respectively. The elimination half-life was about 6.21 ± 3.11 days for the 1 mg/kg/week group and 7.4 ± 2.5 days in the 2 mg/kg/week at steady-state is 25.5 ± 1.6 days at 1 mg/kg/week group. Tend and 44 ± 10 days at 2 mg/kg/week.
Efalizumab shows dose-dependent nonlinear pharmacokinetics which can be explained by its saturable specific binding to cell surface receptors CD11a. Clearance was more rapid at lower doses, suggesting a receptor-mediated mechanism at drug levels below 10 μg/mL.
In a population pharmacokinetic analysis of 1088 patients, body weight was found to be the most significant covariate affecting efalizumab clearance. Other covariates such as baseline PASI, baseline lymphocyte count and age had modest effects on clearance; gender and ethnic origin had no effect.
Additional pharmacokinetic data are available from an open-label extended treatment trial in which patients who responded to an initial treatment of efalizumab, 2 mg/kg, for 12 weeks, received the drug in a maintenance phase for up to 33 months at a dose of 1 mg/kg. Pharmacokinetic analysis of each 12-week treatment period for up to 15 months showed that steady-state trough levels remained constant during continuous efalizumab dosing. There was no evidence of efalizumab accumulation or alteration of the pharmacokinetic profile of efalizumab during long-term continuous dosing.
Efficacy
The efficacy of efalizumab for the treatment of adults with moderate to severe psoriasis () was evaluated in 3 large phase III studies (CitationGordon et al 2003; CitationLebwohl et al 2003; CitationLeonardi et al 2005). Of these studies, 2 also had extension phases lasting an additional 12 weeks (CitationLeonardi et al 2005; CitationMenter et al 2005). In addition, an open-label study investigating the long-term efficacy was initiated (Gottlieb et al 2004). The phase III study by Lebwohl and colleagues (CitationLebwohl et al 2003) was divided into three phases: a treatment phase from weeks 0 to 12, an extended treatment phase from weeks 13 to 24, and lastly a follow-up phase from weeks 25 to 36. Two of these studies, one by CitationLebwohl et al (2003), the other by CitationLeonardi and colleagues (2005), subjects received efalizumab 1 or 2 mg/kg or placebo subcutaneously, after a first dose of 0.7 mg/kg to reduce first dose adverse events. In the other phase III study by CitationGordon et al (2003), subjects received efalizumab 1.0 mg/kg subcutaneously or placebo. In the 3-year long-term study, patients were randomized to receive 12 weeks of open-label efalizumab 2.0 mg/kg once weekly with or without topical fluocinolone ointment (0.025%) during weeks 9 through 12. After these 12 weeks, patients with a PASI score reduction of 50% (PASI-50) were then scheduled to receive efalizumab 1.0 mg/kg once weekly for up to 33 months. Patients that relapsed during the maintenance phase were switched to once-weekly dosing of 2.0 mg/kg for 12 weeks or 4.0 mg/kg for 4 weeks. In the extension study by CitationMenter et al (2006), all the patients that finished the initial 12-week double-blind phase received efalizumab 1.0 mg/kg/week for a further 12 weeks. Another extension phase by CitationLeonardi et al (2005), patients who received efalizumab previously with PASI score reductions less than 75% were then re-randomized to receive placebo or continue on their previously administered dose of efalizumab at 1.0 or 2.0 mg/kg/week.
Table 1 Efficacy of efalizumab in the treatment of psoriasis (adapted from CitationBoehncke et al 2006b)
All of the phase III, double-blind studies used PASI score reductions of 75% (PASI-75) after 12 weeks of treatment as the primary efficacy endpoint. In the long-term study by CitationGottlieb et al (2006), in addition to PASI-75, PASI-50 and PASI-90 scores were examined.
The study by CitationGordon and colleagues (2003) found that all efalizumab-treated patients experienced statistically significant improvement on all end points than those patients receiving placebo. Twenty-seven percent of patients receiving efalizumab achieved PASI-75 versus 4% of the placebo group. In addition, 95% of efalizumab-treated patients achieved PASI-50 compared with 14% of those receiving placebo. With regard to patient reported outcomes, at week 12, patients treated with efalizumab had a greater mean percentage improvement in DLQI with 47% compared with 14% in the placebo group. Efalizumab treatment also produced a 38% improvement in Itching Visual Analog Score (VAS) compared with placebo. Lastly, efalizumab-treated patients had statistically significant improvement in Psoriasis Symptom Assessment (PSA), both frequency and severity subscales (48% vs 18% and 46% vs 17%, respectively), compared with placebo.
In the extension study published by Menter and colleagues (CitationMenter et al 2005), of the 342 subjects who received and completed the 12-week course of efalizumab treatment, 342 enter an open-label treatment period for an additional 12 weeks, receiving 1 mg/kg/week. In addition, 174 subjects who completed a 12-week course of placebo were schedules to receive 12 weeks of efalizumab at the same dose. As the duration of treatment continued, PASI indexes continued to improve. At week 24, 66.6% of the previously efalizumab-treated patients achieved a PASI-50 response, and 43.8% achieved a PASI-75 response. The percentage of patients who achieved a static Physician’s Global Assessment (sPGA) of minimal or clear increased from 25.7% to 35.9% from week 12 to 24. For those subjects who received placebo followed by efalizumab, 28.7% achieved a sPGA rating of minimal or clear after 12 weeks. In addition to physician-assessed parameters, there was a statistically significant improvement after 12 weeks of efalizumab treatment in DLQI, Itching scale, and PSA frequency and severity.
In a study by CitationLebwohl and colleagues (2003), patients receiving 1 mg/kg/week of efalizumab achieved PASI-75 in 22% of the subjects and in 28% of those subjects receiving 2 mg/kg/week, compared with 5% of those subjects receiving placebo. In the extended treatment phase, those subjects achieving PASI-75 or PASI-50 were randomly assigned to continue receiving 2 mg/kg of efalizumab weekly or every other week or placebo. Those subjects not attaining at least PASI-50 were randomly assigned to either an increased dose of 4 mg/kg of efalizumab weekly or placebo. It was found in the extended treatment phase that the efalizumab-treated subjects who initially achieved a PASI-75, a greater proportion of the subjects who received further treatment with efalizumab maintained a PASI-75 compared with those receiving placebo (p < 0.001). Of those subjects who did not achieve a PASI-50 on initial efalizumab treatment, an improvement of 75% or more was achieved in 40% of those subjects receiving efalizumab 4 mg/kg/week, compared with 15% in the placebo group (p = 0.02).
At the 36-week follow-up, 12 weeks after the discontinuation of study treatment, it was found that in subjects who received at least 50% improvement in their PASI index at week 24, the time to relapse (loss of at least 50% of the improvement in the PASI index that had been achieved between base line and week 24) was approximately 84 days.
CitationLeonardi and colleagues (2005) assessed short-term and extended-treatment efficacy and safety of efalizumab in another phase III study. The study was divided into 3 12-week treatment periods, the first from weeks 1 to 12, and retreatment or extended treatment periods during weeks 13 to 24, with 2 observation periods, with subjects receiving an initial treatment of efalizumab 1 mg/kg/week, 2 mg/kg/week, or placebo. During the first treatment week after 12 weeks, significantly more patients receiving 1 mg/kg and 2 mg/kg achieved a PASI-75 (39% and 27%, respectively) compared with those subjects receiving placebo (2%). Those efalizumab-treated subjects who did not achieve PASI-75 were re-randomized at week 12 to receive efalizumab or placebo for an extended 12-week period. At week 24, 20.3% of subjects who received an additional 12 weeks of efalizumab achieved a PASI-75 compared with 6.7% of those receiving placebo.
Gottlieb and colleagues assessed long-term, continuous therapy with efalizumab in a multicenter, open-label, phase III study in patients with moderate to severe chronic plaque psoriasis. Results for the first 27 months of this 36-month continuous therapy trial are available (CitationGottlieb et al 2006). These data document that once-weekly subcutaneous efalizumab maintains sustained efficacy without toxicity. Patients were randomized to receive 12 weeks open-label subcutaneous efalizumab 2.0 mg/kg/week with or without topical fluocinolone during weeks 9 to 12. After the 12th week, patients were then scheduled to receive efalizumab, 1.0 mg/kg/week for up to 33 weeks, if they received at least a PASI-50 during the first 12 weeks of treatment. If a patient relapsed, therapy was increased to 2.0 mg/kg/week for 12 weeks or 4.0 mg/kg/week for 4 weeks. Concomitant topical corticosteroids and UVB phototherapy were also permitted. PASI improvement was maintained throughout the 27-month period.
Safety
Once-weekly injections of efalizumab, 1 mg/kg, was generally well tolerated for 12 weeks to 15 months (CitationGordon et al 2003; CitationLebwohl et al 2003; Gottlieb et al 2004; CitationLeonardi et al 2005; CitationMenter et al 2005). In published clinical trials, 3%–6% of subjects withdrew due to adverse events of efalizumab compared with 1%–3% in the placebo groups. The most common adverse events seen in clinical trials included a first dose complex consisting of headache, nausea, myalgia, fever, and chills that typically developed within 2 days after the first two injections (). After the third dose, these reactions diminished, with similar incidence in both efalizumab and placebo groups (CitationGordon et al 2003; CitationLebwohl et al 2003; Gottlieb et al 2004; CitationLeonardi et al 2005; CitationMenter et al 2005). These reactions were typically well managed with acetaminophen or nonsteroidal anti-inflammatory drugs. Serious adverse events were uncommon. In the three 12-week studies, 2% of efalizumab-treated patients (1 mg/kg/week) had a serious adverse event during treatment. Withdraw from the studies due to these adverse events were rare as well, with a total of 3.5% of efalizumab (1 mg/kg/week) treated patients withdrew from treatment due to adverse events in these same studies, whereas 2.1% of placebo-treated patients withdrew because of adverse events.
Table 2 Safety of efalizumab
Long-term treatment with efalizumab, examined in the study by CitationGottlieb and colleagues (2006), was not associated with an overall increased incidence of adverse events. Those events noted were similar in nature to those documented in short-term trials. There was no evidence of cumulative noted. Two serious adverse events that were determined by the investigator to be drug related included arthritis and gastrointestinal carcinoma.
In the phase III study by CitationGordon and colleagues (2003), infections were present in 27% of efalizumab-treated patients compared with 23% of those receiving placebo. Among these subjects, there was no increased susceptibility to any certain pathogen appreciated upon analysis. In all three phase III studies by CitationGordon et al (2003), CitationLebwohl et al (2003), and CitationLeonardi et al (2005), no statistically significant increased risk of infection was appreciated in the efalizumab treated patients compared with those subjects receiving placebo.
There were 2 cases of malignancy in one clinical trial by CitationGordon and colleagues (2003), which was determined to not be related to efalizumab secondary to the time line of drug initiation and identification of malignancy. According to company generated information, of the 2762 patients who received efalizumab for a mean duration of 8 months, the incidence of malignancies of any kind was 1.8 per 100 patient-years with efalizumab and 1.6 per 100 patient-years with placebo (Raptiva package insert 2005).
During clinical trials, 19 of 2589 patients experience worsening (past baseline) of their psoriasis during or after treatment with efalizumab. The worsening involved new plaques, as well as different forms of their psoriasis, including pustular and erythrodermic psoriasis. Some pateints required hospitalization and alternate psoriasis treatments were administered (Raptiva package insert 2005). Retrospective analysis of pooled data from different studies, however, show that 14% of patients encounter a so-called rebound (worsening of psoriasis to ≥125% of the initial PASI) after abrupt termination of efalizumab treatment (CitationGordon et al 2002) (). The likelihood to encounter a rebound is particularly high among patients who did not encounter a sufficiently profound clinical response, and is seemingly rare after good clinical improvement.
Clinical and post-marketing data have included reports of arthritis, including new onset as well as recurrent, severe arthritis (). Joint pain was noted during treatment as well following discontinuation of efalizumab, and typically resolved after discontinuation of efalizumab and without other therapies (Raptiva package insert 2005).
Platelet counts at or below 52,000 cells/μL were observed in 8 subjects during clinical trials (). Seven (1 patient lost to follow-up) were treated with systemic corticosteroids, with resolution. Post-marketing surveillance has reported cases of severe thrombocytopenia as well, and physicians should monitor platelets count closely. Patients experiencing thrombocytopenia while taking efalizumab should discontinue treatment (Raptiva package insert 2005). Hemolytic anemia, usually 4–6 once after initiation of therapy, was noted, and treatment with efalizumab should be stopped if this develops (Raptiva package insert 2005).
Efalizumab: clinical use and treatment guidelines
Based on the above-mentioned trials, both the FDA as well as the EMEA have approved efalizumab for the treatment of moderate-to-severe plaque psoriasis in adult patients. Whereas efalizumab can be considered alongside with other systemic or phototherapy in the US, the more restrictive European label demands that patients must have failed to respond to, have a contraindication to, or are intolerant to other systemic therapy. Two evidence-based European guidelines recommend the use of efalizumab in patients fulfilling the above-mentioned criteria defined by the European label (CitationSmith et al 2005; CitationNast et al 2006). Expert comments on these criteria have been recently summarized elsewhere (CitationBoehncke et al 2006a): In brief, measures currently used to document disease severity include determination of the affected BSA, PASI, and the DLQI. In the absence of a precise definition, moderate to severe psoriasis is considered to be characterised by scores >10 in any of these instruments, but other criteria such as involvement of the face or joints may also be used.
According to the above-mentioned guidelines, treatment should be initiated with an sc injection of 0.7 mg/kg body weight, followed by weekly sc injections of 1 mg/kg body weight for 12 weeks. The German guideline suggests consideration of continuation in patients with a good clinical response (≥PASI-50) at that time and monthly monitoring of hemoglobin, hematocrit, red/white blood cell and platelet counts as well as liver enzymes; this should be accompanied by a rigid physical examination to detect potential infections. In case of insufficient efficacy, the respective patient should be switched to another therapy. To prevent a possible rebound, the alternative therapy should either follow efalizumab treatment immediately or overlap sufficiently long to guarantee efficacy. Since contraindications to conventional therapies may limit alterantive options, a potential rescue strategy should be defined for each patient individually.
Conclusion
Efalizumab has reproducibly proven its ability to rapidly and effectively control symptoms of moderate-to-severe plaque psoriasis in several randomized, double-blind, placebo-controlled clinical studies. This was associated with substantial improvement of health-related quality of life. Simple self-administration and minimal monitoring requirements add to the practicability of efalizumab from the patients’ and physicians’ perspectives.
Efalizumab was generally well tolerated, with similar rates and types of adverse events in the active and placebo groups. Injection site reactions were the most frequently seen adverse event, presenting mainly as flu-like symptoms after the first and second injections, and could be controlled by decreasing the dose or with nonsteroidal antiphlogistics. Termination of therapy was observed to cause rebound in some 15% of patients with low initial responses, but occurred less frequently (approximately 1%) in patients with a good clinical response and could be prevented by adding other therapies. Leukocytosis was observed frequently, but stayed within physiologic limits and resolved after termination of treatment. Thrombocytopenia was observed occasionally, as were single cases of hemolytic anemia; thus, monitoring should include platelet counts. Dropout rates were approximately 10%, but usually were not due to adverse effects. The risk for adverse events did not increase throughout a 15-month observation period.
Two evidence-based European guidelines recommend the use of efalizumab in adult patients with moderate-to-severe plaque psoriasis.
Acknowledgments
I am grateful to Drs. Karlheinz Schmitt-Rau and Sigbert Jahn for help and advice, particularly on aspects of pharmacokinetics and pharmacodynamics of efalizumab.
References
- BjerkeJRKroghTKMatreJD1978Characterization of mononuclear cell infiltrates in psoriatic lesionsJ Invest Dermatol713403309493
- BoehnckeW-HBrasieJABarkerJ2006aTreatment of psoriasis in Europe using etanercept: thoughts and recommendations from a Dermatology Expert PanelJ Eur Acad Der Venerol2098898
- BoehnckeW-HPrinzJGottliebAB2006bBiologic therapies for psoriasis. A systematic reviewJ Rheumatol3314475116724367
- RichardsHLFortuneDGO’SullivanTM1999Patients with psoriasis and their complicance with medicationJ Am Acad Dermatol41581310495380
- DustinMLBivonaTGPhilipsMR2004Membranes as messengers in T cell adhesion signalingNature Immunol53637215052266
- EedyDJBurrowsDBridgesJM1990Clearance of severe psoriasis after allogeneic bone marrow transplantationBr Med J3009082337714
- Gardembas-PainMIfrahNFoussardC1991Psoriasis after allogeneic bone marrow transplantationArch Dermatol12615232241215
- GordonKBKooJYMFeldmanSR2002Definitions of measures of effect duration for psoriasis treatmentsPsoriasis Forum815
- GordonKBPappKAHamiltonTK2003Efalizumab for patients with moderate to severe plaque psoriasis: a randomized controlled trialJ Am Acad Dermatol290307380
- GottliebABHamiltonTCaroI2006Long-term continuous efalizumab therapy in patients with moderate to severe chronic plaque psoriasis: updated results from an ongoing trialJ Am Acad Dermatol544 Suppl 1S1546316488337
- GottliebABKruegerJBBrightR2000Effects of administration of a single dose of a humanized monoclonal antibody to CD11a on the immunobiology and clinical activity of psoriasisJ Am Acad Dermatol424283510688712
- GottliebABKruegerJBWittkowskiK2002Psoriasis as amodel for T-cell mediated disease: immunobiologic and clinical effects of treatment with multiple doses of afalizumab, an anti CD11a antibodyArch Dermatol13859160012020219
- HildrethJEKAugustJT1985The human lymphocyte function-associated (HLFA) antigen and a related macrophage differentiation antigen (HMac-1): functional effects of subunit-specific monoclonal antibodiesJ lmmunol134327280
- KruegerJG2002The immunologic basis for the treatment of psoriasis with new biologic agentsJ Am Acad Dermatol4612311756941
- LebwohlMTyringSKHamiltonTK2003A novel targeted T-cell modulator, efalizumab, for plaque psoriasisN Engl J Med34920041314627785
- LeonardiCLPappKAGordonKB2005Extended efalizumab therapy improves chronic plaque psoriasis: results from a randomized phase III trialJ Am Acad Dermatol524253315761420
- MenterAGordonKCareyW2005Efficacy and safety observed during 24 weeks of efalizumab therapy in patients with moderate to severe plaque psoriasisArch Dermatol14131815655139
- MenterALeonardiCLSterryW2006Long-term management of plaque psoriasis with continuouse efalizumab therapyJ Am Acad Dermatol544 Suppl 1S182816488340
- MortensenDLWalickePAWangX2005Pharmacokinetics and pharmacodynamics of multiple weekly subcutaneous efalizumab doses in patients with plaque psoriasisJ Clin Pharmacol452869815703364
- NastAKoppIBAugustinM2006S3-Leitlinie zur Therapie der Psoriasis vulgarisJDDG Supplement2S1126
- NickoloffBJWrone-SmithT1999Injection of pre-psoriatic skin with CD4+ T cells induces psoriasisAm J Pathol1551455810393847
- PappKBissonnetteRKruegerJG2001The treatment of moderate to severe psoriasis with a new anti-CD11a monoclonal antibodyJ Am Acad Dermatol456657411606914
- RappSRFeldmanSRExumML1999Psoriasis causes as much disability as other major medical diseasesJ Am Acad Dermatol41401710459113
- SchönMPBoehnckeWH2005PsoriasisN Engl J Med3521899191215872205
- SmithCHAnsteyAVBarkerJN2005British Association of Dermatology guidelines for the use of biological interventions in psoriasis 2005Br J Dermatol1534869716120132
- SternRSNijstenTFeldmanSR2004Psoriasis is common, carries a substantial burden even when not extensive, and is associated with widespread treating dissatisfactionJ Invest Dermatol Symp Proc91369
- SterryWBarkerJBoehnckeWH2004Biological therapies in the systemic management of psoriasis: International Consensus ConferenceBr J Dermatol151Suppl 6931715265063
- StroberBESiuKMenonK2006Systematic review of conventional systemic agents for psoriasisJ Rheumatol331442616724368
- WertherWAGonzalezTNO’ConnorSJ1996Humanization of an anti-lymphocyte function-associated antigen (LFA)-1 monoclonal antibody and reengineering of the humanized antibody for binding to rhesus LFA-1J Immunol1574986958943405