Abstract
Oncology outcomes research could benefit from the use of an oncology-specific electronic medical record (EMR) network. The benefits and challenges of using EMR in general health research have been investigated; however, the utility of EMR for oncology outcomes research has not been explored. Compared to current available oncology databases and registries, an oncology-specific EMR could provide comprehensive and accurate information on clinical diagnoses, personal and medical histories, planned and actual treatment regimens, and post-treatment outcomes, to address research questions from patients, policy makers, the pharmaceutical industry, and clinicians/researchers. Specific challenges related to structural (eg, interoperability, data format/entry), clinical (eg, maintenance and continuity of records, variety of coding schemes), and research-related (eg, missing data, generalizability, privacy) issues must be addressed when building an oncology-specific EMR system. Researchers should engage with medical professional groups to guide development of EMR systems that would ultimately help improve the quality of cancer care through oncology outcomes research.
Introduction
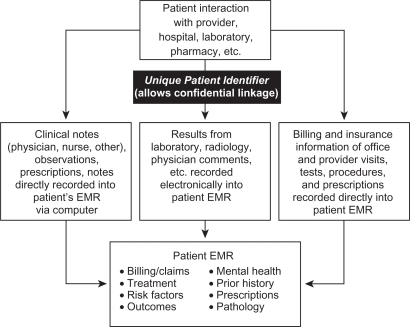
The term “EMR” generally refers to an electronic medical record and can indicate the establishment and use of standardized electronic databases for health care, with a digital record as its basis. Current EMR systems contain a record of all clinical, administrative, and laboratory encounters between a patient and a provider, including medical notes, results, billing claims, and insurance information, typically linked with a unique patient identifier (). The most comprehensive EMR databases would be those that have a stable population (eg, low rate of patients moving out of the medical system) and include records from all in- and out-patient care, laboratory and radiological results, and all prescribed and over-the-counter (OTC) medications, with a unique identifier for each patient to link them to different medical care providers and services, and to maintain confidentiality.
Figure 1 Schematic of current electronic medical record (EMR) components.
Current EMR systems in the United States (US) that fit this description exist at a few large, integrated health providers, such as Kaiser Permanente, Harvard Pilgrim Health System, and the Department of Veterans Affairs (VA), but are generally lacking. With only 25% of Americans belonging to any type of health maintenance organization (HMO),Citation1 this type of health care structure is not typical. While European and socialized countries may have existing platforms (eg, registries, health care systems) that are more readily suitable to EMR, with some exploring EMRs in oncology,Citation2 the primary focus of the current article is on the US.
The potential utility of EMR to enhance clinical medicine was recognized in the 1990s, primarily due to the increasing use of the Internet. The widespread use of the Internet fostered more cooperative relationships among doctors, patients, and other care providers, allowing for merging of data across different treatment settings. Several government initiatives and programs have been developed over the past several years to increase the use and development of EMR systems in the US ().
Table 1 Brief history of government initiatives to develop and use EMR
The use of an EMR in clinical medicine offers numerous potential benefits, including an improvement in the quality of patient care, a reduction in the cost of health care, and improvement in the ease of transferring patient information among providers.Citation3 In the US, maintenance of electronic records of continuous care is often hindered by frequent changes in providers and plan members, due to job changes or changes in coverage, but EMR adoption across a wide range of health systems could potentially provide a seamless record even across such changes and patient migration. The adoption of EMR, however, has generally been slow due to the cost of system implementation and user training. While the US government has been promoting the adoption of a national EMR system, little guidance has been provided on how it should look or function.Citation4 To date, less than 20% of group physician practices in the US have adopted EMRs.Citation5 In particular, small practices, which make up approximately 80% of all physician practices, have been slower to adopt EMR than physician groups associated with larger hospitals and health systems.Citation6 The general challenges of adopting and using EMR have been discussed elsewhere.Citation3,Citation7
While the benefits and challenges for adoption and use of EMR in clinical medicine and general health research have been investigated, the utility of EMR for oncology outcomes research has not been explored. In this paper, we describe how oncology outcomes research can benefit from the use of a hypothetical oncology-specific EMR network that incorporates widespread coverage, both across provider types and networks, as well as geographically. Although this level of coverage may not currently exist, even in best practice, among existing EMR systems, the purpose of this paper is to demonstrate the breadth of research questions and beneficial parties who will be affected when and if such a system is implemented. In addition, we describe the specific challenges that must be addressed when building such a system.
EMR for oncology research
With comprehensive and accurate information on clinical diagnoses, personal and medical histories, planned and actual treatment regimens, and post-treatment outcomes, EMR systems could provide a wealth of data for outcomes research. In a comprehensive literature review of the number and types of EMR systems used for outcomes research from 2000 through 2006, the number of EMR-based research studies conducted annually has increased 6-fold.Citation8 Although the use of computerized clinical information has been demonstrated to improve the efficiency of oncology clinical practice (eg, with computerized chemotherapy producing significantly fewer errors than manual prescriptions,Citation9 only 10% of 126 published studies of outcomes research using EMR from the US focus on oncology outcomes.Citation8 In addition, several limitations exist in using EMR data, which must be considered (discussed later).
Implementation of comprehensive EMR systems that focus specifically on the treatment of oncology patients could answer many questions that are unique to oncology clinical practice (eg, see ). The relevance of research from such a resource would be broad, with the potential to benefit parties at each level within the US health care structure from oncology patients, researchers, and clinicians; to policy makers, health economists, and administrators; to pharmaceutical and other health companies. These various perspectives are described in more detail below (see also ).
Figure 2 Utility of electronic medical record (EMR) to various groups for outcomes research.
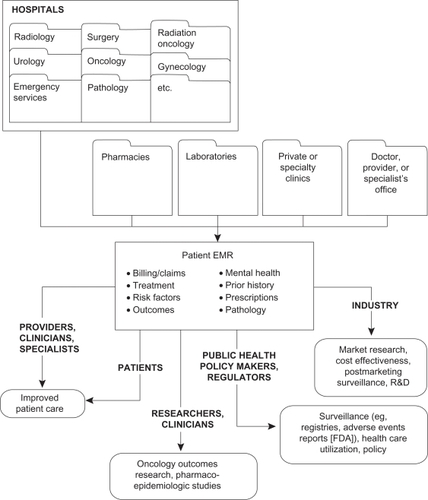
Table 2 Examples of outcomes research questions that may be addressed with an oncology-specific EMR
Utility of oncology EMR compared to other available data sources
Several clinical and research databases are currently being used to conduct clinical outcomes research in oncology. provides a summary of some of these data sources and their advantages and disadvantages when conducting outcome research, and how an “ideal” EMR could improve upon such databases. These data sets vary in breadth of coverage (national to regional), funding source (private to national government funded), mechanism of data collection (continuous, post hoc), and scope of data collected. While each contains unique elements that allow it to answer specific oncology research questions among certain populations, each is also limited by specific constraints that may be improved upon by a widespread, comprehensive, and provider/insurance-neutral EMR network of oncology practices.
Table 3 Summary of selected existing databases and improvements provided by oncology EMR
An ideal oncology EMR would provide several advantages over current research, observational studies, and claims databases. Clinical data gathered in the course of routine medical care, if systematically collected and routinely stored, would provide a data source less costly in labor and operational funding than current research databases; would be more accessible than integrative HMO data; would prospectively collect patient data and characteristics, permitting analyses of factors from many points during the course of disease both pre- and post-diagnosis (unlike most population-based case-control studies); and would follow the entire patient cancer experience from diagnosis onward, collecting information that may affect outcomes. Further, this information would be more suitable for real-world research than data obtained in clinical trials.
Relevance to the patient, clinician, and medical researcher
For patients, providers, and researchers, the most relevant questions focus on improving health and quality of life (QOL), providing better quality of care, and advancing disease knowledge. For example, an oncology patient would be interested in their chances of surviving existing disease and preventing future tumor recurrence. While many population-based observational studies have examined the relation of pre-diagnosis lifestyle factors – such as weight, diet, exercise, nonsteroidal anti-inflammatory drug (NSAID) use, alcohol consumption, and smoking – with cancer risk, the effect of risk factors on survival after diagnosis has been more difficult to study. In particular, studies that attempt to elicit self-reported risk factors occurring after diagnosis are susceptible to lead-time bias and recall bias,Citation10 particularly if the time between diagnosis and interview is protracted, and only certain individuals survive long enough to be interviewed. Further, because the experience of cancer treatment, as well as the presence of disease itself, can affect behaviors, pre-diagnosis risk-factor information may not accurately reflect behaviors after diagnosis. An EMR system that collects information on some common health-related behaviors both pre- and post-diagnosis, medications and treatments, and response to treatment in a standardized fashion could aid in elucidating the complex inter-relationships among these factors. In addition, patient choice – such as the type of therapy or the decision to treat their disease at all – is a primary predictor of treatment patterns in several cancers,Citation11–Citation15 and information collected by EMR on treatment efficacy and side effects may directly influence the decision-making process.
A practicing oncologist might be interested in studies of various chemotherapeutic agents, dosages, and regimens to prolong patient survival with the least risk of toxicity, side effects, and other detriments to QOL. Although clinical trial data provide some evidence of efficacy, they are conducted within a controlled treatment structure and among patients that are highly selected by health status, tumor type, and previous response to treatment. Thus, the data from these trials may not provide a realistic view of treatment response within a “real-world” administration. In addition to wide variation among cancer patients with respect to personal and tumor characteristics, differences in psychological factors and lifestyle choices may influence their course of disease and response to treatment. Even among patients with similar prescribed regimens and dosages, individual adherence to recommended treatment, and differences in patient choices of treatment type, may further influence response.
In an EMR-based oncology practice, the adherence to prescribed regimen, reported treatment side effects, psychological concerns, and possibly other modifiers of treatment efficacy would be recorded with each clinic visit. In combination with quantifiable outcomes data (eg, disease progression or survival), an oncology EMR can provide clinicians with a more representative data source by which to develop their medical recommendations. These data from an EMR could also help researchers investigate ways to improve guideline adherence and implementation of evidence-based medicine for follow up and treatment that may improve the care received by the oncology patient.
Advances in biotechnology and bioinformatics have permitted the examination of etiologic and outcomes research in oncology with increasing detail, with molecular, cellular, and other biological measurement often incorporated to characterize cancer and disease progression (see ). EMR systems that record such biomarker data, when available, over the course of clinical practice could provide a potentially cost-effectiveCitation16 and efficient means for conducting this research, and are a valuable tool in pharmacoepidemiologic studies.
Relevance to the policy maker
From the policy makers’ perspective, outcomes research in oncology can provide clues to identify deficits in outreach and programmatic spending and current health care resource utilization and accessibility. The recent Institute of Medicine (IOM) report on optimizing the effectiveness of health care servicesCitation17 recommends conducting systematic reviews of current published research on the effectiveness of health services to create a link between scientific evidence and clinical decision-making. New research studies using comparative effectiveness study methods (eg, comparing new drugs, devices, and procedures to current treatment options)Citation18,Citation19 can also provide answers on what treatments are most effective from both the cost and clinical standpoints for specific populations, such as addressing whether health care resources are being spent on the most effective treatments for oncology patients. EMR systems could be a valuable resource for conducting these research studies in oncology, because they contain more comprehensive health histories and outcome information than claims databases or other disease registries for researchers to address a variety of treatments and outcomes.
Research and public health measures aimed at identifying deficits and disparities in medically underserved groups, and mitigating these differences, have become high priorities of government health care program policies.Citation20–Citation23 Rates of cancer incidence, mortality, and survival may differ by age, race/ethnicity, socioeconomic status (SES), educational attainment level, and geographic location,Citation24 and it is thought that access to health care, screening, and treatment resources, and the quality of treatment given, may underlie a large proportion of these differences.Citation25 For example, analyses of a population-based cancer registry of patients aged 66 to 85 years with a primary diagnosis of colorectal, breast, lung, or prostate cancer during 1992 to 2002, researchers found that black patients were significantly less likely than white patients to receive therapy for their cancer, and there was no evidence that the magnitude of racial disparities had lessened during the study period.Citation26 Disparities in cancer treatment can vary across cancer types, with differential impacts on access to care, ability to absorb costs, and cultural and personal biases, all of which are factors not currently captured in most available data. EMR systems that contain detailed insurance, personal, and clinical information may form a more complete picture of the many factors that influence treatment patterns, providing policy makers with better direction when directing health care policies.
Relevance to the pharmaceutical industry/manufacturer
EMR systems could provide answers to research questions relevant to several groups within the pharmaceutical and biotechnology industries. With comprehensive and accurate information on various aspects of patient-care information, EMR could potentially provide a set of clinical data to answer questions related to marketing, outcomes research, research and development, and phase IV post-marketing surveillance (eg, adverse events identification, targeted evaluation of treatment groups, observational studies), among others. For example, information in EMR (received by the pharmaceutical industry data de-identified of personal information) could be mined to determine the size of therapeutic markets for rare cancers or conditions, or in populations that are resistant to or cannot take conventional medication. EMR could also aid industry in evaluating the prevalence or incidence of certain conditions and associated co-morbidities, in various subpopulations, in certain types of hospitals, or in different areas, to aid in marketing drugs and supporting new drug applications and other regulatory documentation.
Economic analyses and health care resource use evaluations would also be possible with EMR systems. Cost-effectiveness strategies of pharmacologic therapy could be evaluated, including for example, population of predictive health economics models for forecasting costs and market share. Forecasting models could also be developed from these data, with particular focus on specific drugs, disease stage, line of therapy, or clinic type, provided that issues of generalizability were accounted for (see later section). From a marketing point of view, EMRs could also be used to develop differentiation strategies among competing firms by evaluating patient profiles and drug use.
Because EMRs represent a “real-world” patient cohort, these data could also be used to aid in preparation of regulatory applications using actual population-based data, as well as in identification of possible safety issues, and could therefore also be of use in pharmacovigilance studies. A clear EMR record of all medications prescribed and taken, whether for medications, biological products, or herbal supplements could aid in understanding and preventing adverse events with certain therapeutics. EMRs may be beneficial for process-of-care studies, where insight into patient care, disease endpoints, and therapies could be evaluated in tandem in a single EMR and could aid in beneficial results for patients (eg, shorter lengths of stay in hospital, preventive or palliative care). Detailed clinical and laboratory history of patients undergoing treatment contained in EMR may reveal new indications or contraindications of existing therapeutics. Effectiveness of therapeutics could also be tracked in certain situations through clinical practice and reporting of patient outcomes.
Challenges of using EMR for oncology research
Despite the promise that EMR can provide for oncology outcomes research, several challenges must be considered to develop a comprehensive, valid, and useful data resource. While many of these challenges of EMR are general, some are oncology specific. Challenges can include structural,Citation27,Citation28 clinical,Citation29,Citation30 and public health research-related issues,Citation31,Citation32 all of which should be considered in building a useful EMR system.
Structure
At present, a variety of options are available in EMR systems, and physician groups and health systems are free to choose the system best suited to their needs.Citation3 For example, the American Society of Clinical Oncology (ASCO) has developed a set of recommendations for oncologists to use in choosing an EMR.Citation33 ASCO identified several important elements that should be included in any EMR used by an oncologist: ability to enter staging information, work flow, chemotherapy doses and administration, toxicity assessment, clinical trial management, drug inventory management, and survivor care.
Interoperability
Regardless of the type of EMR system chosen, it will need to be interoperable, that is, having the ability to interact and exchange data across departments and clinics (eg, laboratory, pathology, clinic).Citation34 Without interoperable interfaces, information cannot be exchanged easily, which can affect the work flow for the clinic and could lead to missing information within the medical record and major problems with data quality and completeness.
Incorporation of different data formats
Information available in an EMR may include a variety of data formats, ranging from text for office visits to images from radiology visits. In addition, results can include text reports, numerical data such as laboratory values, graphs, and images such as CT scans or MRIs. As such, the results can be entered using a wide variety of methods, including direct data uploads from the processing laboratory, scanning of text using optical character recognition, or simply capturing the electronic readout as an image. Physician orders can be recorded in several ways, with varying degrees of automation, including selecting individual chemotherapy drugs with pre-populated fields or customizing automated orders with free-text entry. However, treatment offered outside the institutions that contribute to the EMR (eg, radiation therapy) may be available only from information scanned into the EMR system, which may not be readily searchable by computer algorithms if they contain non-text fields such as images.
Due to the variety of sources, data collection may be time intensive, requiring manpower and database management.Citation35 Because some of the information in the EMR may be text based,Citation27 rather than consisting of a data set or collection of raw values, natural language algorithms may be necessary to extract the information of interest. Studies using natural language algorithms have been able to identify a majority of potential study participants by disease type. For example, a study designed to identify cases of heart failure from an EMR found 100% sensitivity and 97.8% specificity when using this method.Citation36 Other limitations may include not being able to extract information from reports that have been scanned into the medical record using these algorithms, and not having access to previous paper records that have not been incorporated into the EMR.Citation3
Clinical
Variety of diagnostic coding vocabulary
The coding vocabulary used to identify and define cancer cases within the medical record varies by physician type. Standard codes include the American Joint Committee on Cancer (AJCC) codes for tumor staging, Systematized Nomenclature of Medicine (SNOMED) used primarily by pathologists, and various International Classification of Diseases (ICD) codes (ICD-9-CM, ICD-10, and ICD-O), and Current Procedural Terminology (CPT) for coding of diagnoses and procedures performed during diagnosis and treatment. In some cases, the clinicians are not the ones directly recording the codes, but they provide a narrative of the disease history or clinic visit that is subsequently coded by medical record coders at a later time, strictly for billing purposes. Disease progression of cancer, in particular metastasis or recurrence, may follow a variety of pathways, and there is no standard for recording progression in the medical record, nor are cancer-specific codes available for identifying cancers that have progressed. Because several standardized codes are used over the course of an oncology patient’s care by different departments and treating physicians, with some used primarily for billing purposes, the researcher will need to consider all sources of codes, and possibly lack of codes, to identify cancer cases or they may miss identifying all cases of a particular cancer.
Linking of departments and continuity of care
Cancer, as a diagnosis, encompasses a variety of tumor types that are treated by physicians in a variety of specialties, including general surgery, hematology, oncology, urology, and endocrinology. Within a comprehensive health care system, these specialties may be handled with an interconnected EMR; however, outside these health systems, the specialties may not be linked in a standardized fashion, or some specialty department may not use EMR. In addition, practices are often challenged in the amount of retrospective information that they receive from prior health care providers and institutions, and are also constrained by costs and logistics in the amount of data they can enter into the EMR due to inadequate time and staffing. Longitudinal observations of study subjects may be difficult if data prior to the adoption of the EMR have not been added to the database. The concerns of not incorporating records from all specialties providing care are 2-fold.
First, patients with some cancers, such as prostate cancer or early-stage breast cancer, may be diagnosed and treated primarily within one or two departments (eg, urology, surgery) or, as is the case for the majority of patients, different outpatient clinics entirely. If the EMR does not link these departments, these patients and essential elements of their clinical history may be missed. This may also make the construction of the oncology patient’s cancer experience incomplete. Similarly, for childhood cancers, specialized hospitals and clinics that deal primarily with pediatric cancers may or may not be connected with the EMR where the children receive their primary care. For researchers interested in other subpopulations, such as those investigating rare cancers or conditions that are difficult to diagnose in some cases (eg, Ewing’s sarcoma), the low adoption rates of EMR may present a barrier to identifying these small groups, because the number of cases may be too small from available EMR data, thereby preventing a study from being adequately powered for research.
Second, outcomes of procedures that are not considered clinically relevant to a particular department may not be captured in their EMR system. For example, persisting post-surgery incision pain that affects QOL may not be recorded within a surgical department EMR as an outcome of surgery, particularly if there is a long lag time after the procedure or if the patient seeks care from their primary care physician.
Research-specific
The most obvious problem with using EMR systems for research is that they collect information and are designed for the care of each individual patient; the data are not collected specifically for research. For example, demographic data collected for patient care, rather than research purposes, may not be collected systematically with standardized definitions. Thus, the rigors of data collection for research, including validation, quality checking, and reproducibility, are not inherent in the EMR-collected data. Issues related to the reliability and validity of a study, such as dealing with missing data and generalizability to the source population, as well as ethics and privacy concerns and general accessibility when using an EMR, must be considered.
Missing data
Missing information in the EMR may lead to misclassification of exposure and/or outcome in epidemiologic and other research.Citation31 Another consideration is the extent of the data collected within the EMR (eg, personal/medical histories, planned versus actual treatment regimens, psychosocial parameters, follow-up on treatment outcomes). Because various physicians or practices may record information differently, the researcher will have to make decisions on whether the collected data set is complete. A study performed in a network of primary-care clinics determined that clinicians reported missing clinical information in almost 14% of visits.Citation37 In addition, there may be a lag time between the clinic visit and data entry into the EMR. The researcher will also need to distinguish whether information is missing or was just never followed through or recorded. For example, the researcher may need to determine whether a record is requesting a treatment or recording that treatment was given. Insurance claims data sets capture treatments that are given; thus, an EMR linked to an insurance claims database could help ascertain the difference. If paper records are available, they could also be used to identify missing data. Researchers will need to account for missing data in their analyses to ensure robustness and accuracy.
Generalizability
The population covered within an EMR may not be representative of the underlying population in the region, thus limiting the generalizability of potential research studies to larger populations or to the US in general.Citation31 Due to the low adoption rates of EMR mentioned previously, there may be few clinics or hospitals in a geographic area that collect medical records electronically. Clinics and hospitals that have adopted EMR may be different in terms of the patient population that uses the facilities compared to those clinics and hospitals that have not adopted EMR. Even within clinics, there may be differences in patient participation and enrollment, depending on physician and patient preference, thereby possibly skewing the population characteristics. Researchers should keep generalizability in mind when interpreting the results of studies conducted with EMR data.
Ethical and privacy concerns
Any large database of identifiable personal health information (PHI), such as that from an EMR, is subject to the Common RuleCitation38 and the Health Insurance Portability and Accountability Act (HIPAA), which also has a privacy rule embedded within it.Citation39 The researcher must work with the Institutional Review Board (IRB) associated with the EMR to ensure that the research activity protects the privacy and confidentiality of the patients included. Additional safeguards to protect the privacy and confidentiality of subject data can include de-identification of PHI, password protection, data encryption, and use of firewalls if there is potential for Internet access to the information.Citation40
Conclusions and future directions
Cancer continues to be a leading cause of morbidity and mortality, and there is an increasing need for new data sources to address questions regarding oncology outcomes, particularly when current data systems used in research are limited. The drive to achieve a nationwide system of electronic medical records, and the recommendation by the IOM to optimize health services through systematic reviews is a call for researchers to engage with medical professional groups to help guide development of EMRs and EMR-based systems that have utility for several groups, including patients and policy makers. This interaction will ensure that secondary uses of the data are secure and protect patient privacy, are useful to researchers and others, and will help improve the quality of cancer care through oncology outcomes research.
Acknowledgments/disclosures
Funding for this manuscript provided by Amgen, Inc. At the time of writing Drs O’Malley, Fryzek and Nordyke were employees and stockholders of Amgen, Inc.; they have no relevant conflicts of interest. Drs Kanas, Morimoto, and Mowat are employees of Exponent, Inc. and have no relevant conflicts of interest.
References
- National Center for Health StatisticsHealth, United States, 2007 with Chartbook on Trends in the Health of AmericansHyattsville, MD2007
- GalligioniEBerloffaFCaffoODevelopment and daily use of an electronic oncological patient record for the total management of cancer patients: 7 years’ experienceAnn Oncol200920234935218718889
- MehtaNBPartinMHElectronic health records: a primer for practicing physiciansCleve Clin J Med2007741182683018020002
- American Recovery and Reinvestment Act of 2009 http://www.gpo.gov/fdsys/pkg/PLAW-111publ5/content-detail.html. accessed Feb 23, 2009
- BurtCWSiskJEWhich physicians and practices are using electronic medical records?Health Aff (Millwood)20052451334134316162581
- ThakkarMDavisDCRisks, barriers, and benefits of EHR systems: a comparative study based on size of hospitalPerspect Health Inf Manag20063518066363
- BaronRJFabensELSchiffmanMWolfEElectronic health records: just around the corner? Or over the cliff?Ann Intern Med2005143322222616061920
- DeanBBLamJNatoliJLButlerQAguilarDNordykeRJUse of electronic medical records for health outcomes research: A literature reviewMed Care Res Rev200966661163819279318
- Huertas FernandezMJBaena-CanadaJMMartinez BautistaMJArriola ArellanoEGarcia PalaciosMVImpact of computerised chemotherapy prescriptions on the prevention of medication errorsClin Transl Oncol200681182182517134971
- SchmierJKHalpernMTPatient recall and recall bias of health state and health statusExpert Rev Pharmacoecon Outcomes Res20044215916319807519
- CardosoFDiLALohrischCBernardCFerreiraFPiccartMJSecond and subsequent lines of chemotherapy for metastatic breast cancer: what did we learn in the last two decades?Ann Oncol200213219720711885995
- DonovanKAGreenePGShusterJLPartridgeEETuckerDCTreatment preferences in recurrent ovarian cancerGynecol Oncol200286220021112144829
- PensonRTDignanFSeidenMVAttitudes to chemotherapy in patients with ovarian cancerGynecol Oncol200494242743515297184
- OsobaDLessons learned from measuring health-related quality of life in oncologyJ Clin Oncol19941236086168120561
- WeeksJCCookEFO’DaySJRelationship between cancer patients’ predictions of prognosis and their treatment preferencesJAMA199827921170917149624023
- SchmierJKKaneDWHalpernMTPractical applications of usability theory to electronic data collection for clinical trialsContemp Clin Trials200526337638515911471
- Institute of Medicine (IOM)Knowing What Works in Health Care: A Roadmap for the NationWashington, DCThe National Academies Press2008
- Agency for Healthcare Research and Quality Effective Health Care. URL: effectivehealthcare.ahrq.gov, accessed February 17, 2009.
- Congressional Budget Office Research on the Comparative Effectiveness of Medical Treatments: Issues and Options for an Expanded Federal Role; 2007 December. http://www.cbo.gov/doc.cfm?index=8891. accessed Feb 23, 2009.
- Health Disparities Collaboratives (HDC) URL: http://www.healthdisparities.net/hdc/html/collaborativesOverview.aspx. Accessed June 25, 2008.
- Healthy People 2010Understanding and Improving Health2nd edUS Department of Health and Human Services2382000US Government Printing Office2000
- Strategic research plan to reduce and ultimately eliminate health disparities, fiscal years 2002–2006. 2002. http://ncmhd.nih.gov/our_programs/strategic/pubs/VolumeI_031003EDrev.pdf. Accessed June 25, 2008
- LisoviczNWynnTFouadMPartridgeEECancer health disparities: what we have doneAm J Med Sci2008335425425918461726
- The NCI Strategic Plan for Leading the Nation to Eliminate the Suffereing and Death Due to Cancer. In: Institute NC, ed NIH Publication No. 06-5773. US Department of Health and Human Services, National Institutes of Health; 2006
- LiCIMaloneKEDalingJRDifferences in breast cancer stage, treatment, and survival by race and ethnicityArch Intern Med20031631495612523916
- GrossCPSmithBDWolfEAndersenMRacial disparities in cancer therapy: did the gap narrow between 1992 and 2002?Cancer2008112490090818181101
- HayrinenKSarantoKNykanenPDefinition, structure, content, use and impacts of electronic health records: a review of the research literatureInt J Med Inform200877529130417951106
- AmbinderEPA history of the shift toward full computerization of medicineJ Oncol Pract200512545620871680
- AmbinderEelectronic health recordsJ Oncol Pract200512576320871681
- ASCO Electronic Health Record RoundtableEnsuring continuity of care through electronic health recordsJ Oncol Pract20073313714220859398
- AschengrauASeageGREssentials of Epidemiology in Public HealthBostonJones and Bartlett Pub2003
- GoldweinJUsing an electronic health record for researchJ Oncol Pract200735278279
- ASCO Develops Practical Guide for Selecting, Implementing Electronic Health RecordsASCO Daily News200824B
- DetmerDBloomrosenMRaymondBTangPIntegrated personal health records: transformative tools for consumer-centric careBMC Med Inform Decis Mak200884518837999
- WeinerMGLymanJAMurphySWeinerMElectronic health records: high-quality electronic data for higher-quality clinical researchInform Prim Care200715212112717877874
- PakhomovSWestonSAJacobsenSJChuteCGMeverdenRRogerVLElectronic medical records for clinical research: application to the identification of heart failureAm J Manag Care2007136 Part 128128817567225
- SmithPCAraya-GuerraRBublitzCMissing clinical information during primary care visitsJAMA2005293556557115687311
- Department of Health and Human Services Protection of Human Subjects. 45 CFR 462008128140 http://www.hhs.gov/ohrp/human-subjects/guidance/45cfr46.htm. accessed Feb 23, 2009
- Health Insurance Portability and Accountability Act of 1996 (HIPAA), PL 104-191-2003
- WolfLEWaldenJFLoBHuman subjects issues and IRB review in practice-based researchAnn Fam Med20053Suppl 1S30S3715928216
- BushGW Exec. Order No. 13335: Incentives for the Use of Health Information Technology and Establishing the Position of the National Health Information Technology Coordinator40. Weekly Compilation of Presidential Documents2004702704
- Food and Drug Administration FDA’s Critical Path Initiative. URL: http://www.fda.gov/oc/initiatives/criticalpath/. Accessed February 23, 2009.
- Food and Drug AdministrationThe Sentinel Initiative, National Strategy for Monitoring Medical Product SafetyDepartment of Health and Human Services52008
- US Department of Health and Human ServicesAchieving a Transformed and Modernized Health Care System for the 21st Century: CMS Strategic Action Plan 2006–200910162006
- GrodsteinFNewcombPAStampferMJPostmenopausal hormone therapy and the risk of colorectal cancer: a review and meta-analysisAm J Med1999106557458210335731
- Hebert-CroteauNA meta-analysis of hormone replacement therapy and colon cancer in womenCancer Epidemiol Biomarkers Prev1998786536599718216
- ChlebowskiRTWactawski-WendeJRitenbaughCEstrogen plus progestin and colorectal cancer in postmenopausal womenN Engl J Med200435010991100414999111
- ChanJAMeyerhardtJAChanATGiovannucciELColditzGAFuchsCSHormone replacement therapy and survival after colorectal cancer diagnosisJ Clin Oncol200624365680568617179103
- SlatteryMLAndersonKSamowitzWHormone replacement therapy and improved survival among postmenopausal women diagnosed with colon cancer (USA)Cancer Causes Control199910546747310530618
- RitenbaughCStanfordJLWuLConjugated equine estrogens and colorectal cancer incidence and survival: The Women’s Health Initiative Randomized Clinical TrialCancer Epidemiol Biomarkers Prev200817102609261818829444
- ChenYCHunterDJMolecular epidemiology of cancerCA Cancer J Clin20055514554 quiz 5715661686
- SorlieTPerouCMTibshiraniRGene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implicationsProc Natl Acad Sci U S A20019819108691087411553815
- BidardFCConfortiRBouletTMichielsSDelalogeSAndreFDoes triple-negative phenotype accurately identify basal-like tumour? An immunohistochemical analysis based on 143 ‘triple-negative’ breast cancersAnn Oncol20071871285128617675400
- CareyLAPerouCMLivasyCARace, breast cancer subtypes, and survival in the Carolina Breast Cancer StudyJAMA2006295212492250216757721
- KimMJRoJYAhnSHKimHHKimSBGongGClinicopathologic significance of the basal-like subtype of breast cancer: a comparison with hormone receptor and Her2/neu-overexpressing phenotypesHum Pathol20063791217122616938528
- CleatorSHellerWCoombesRCTriple-negative breast cancer: therapeutic optionsLancet Oncol20078323524417329194
- SorlieTPerouCMFanCGene expression profiles do not consistently predict the clinical treatment response in locally advanced breast cancerMol Cancer Ther20065112914291817121939