Abstract
Osteoporosis in men is an increasingly recognized problem with associated fracture morbidity and mortality. Treatment is limited, with the bisphosphonates being the mainstay of therapy. Risedronate has demonstrated fracture efficacy in women and efficacy has been recently been investigated in men. In men, risedronate either maintains or increases bone mineral density. In placebo controlled trials it has been shown to be safe and effective in preventing fractures.
Osteoporosis in men
Osteoporosis is increasingly recognized in men as a condition that is associated with significant morbidity and mortality. Data from the third National Health and Nutrition Examination Survey (NHANES III) indicate that 3%–6% of men in the US have osteoporosis and 28%–47% have osteopenia when using male cut-offs for bone mineral density (BMD) (CitationLooker et al 1997). In a population-based sample Melton et al compared osteoporosis in men with women (CitationMelton et al 1998). By World Health Organization criteria, the age-adjusted prevalence of osteoporosis at the hip, spine, or wrist was 35% among women 50 years of age or older. A similar approach produced an osteoporosis prevalence rate in men 50 years of age and older of 19%. They showed that bone density predicts fracture risk in men as it does in women, and the prevalence of osteoporosis in men, using sex-specific normal values, is substantial. They concluded that there was a need for better prevention and treatment strategies for men (CitationMelton et al 1998).
There are several differences in the clinical presentation of osteoporosis between men and women (CitationPoor et al 1995a; CitationVanderschueren et al 2000; CitationDiamond 2005). Men achieve approximately 1% greater peak bone mass than women at the spine and 5% at the femoral neck (CitationLooker et al 1997; CitationTenenhouse et al 2000). Although the incidence of osteoporosis-related fractures is much less in men, osteoporotic fractures are associated with greater morbidity and mortality in men compared with women (CitationJiang et al 2005). Among men and women >50 years of age, the incidence of spinal fractures was estimated at 5% and 16% and that of hip fractures at 6% and 18%, respectively (CitationDiamond 2005). Men with hip fractures have greater mortality (CitationPoor et al 1995b; CitationJiang et al 2005; CitationHawkes et al 2006) and at least in one study were twice likely to die compared with women with hip fractures (CitationPoor et al 1995a). Among men with hip fractures who survive, 80% will not regain their prefracture functional status and up to 50% will be institutionalized (CitationPoor et al 1995b).
Observational data showed that men referred to tertiary care osteoporosis centers had higher mean baseline femoral neck and lumbar spine bone mineral densities than women, yet they had double the rate of prevalent vertebral fractures compared with women and triple the rate of multiple prevalent vertebral fractures compared with women (CitationSawka et al 2004). Furthermore, men were twice as likely as women to sustain a fracture within 2 years of starting treatment during the observation period. It was suggested that osteoporosis may be under-recognized in men until the condition is at an advanced stage and that a form of gender bias may exist in the recognition and treatment or referral for treatment of osteoporosis in men.
In male patients presenting with osteoporotic fractures, major causes of skeletal fragility, such as hypogonadism, glucocorticoid excess, primary hyperparathyroidism and alcohol abuse, can often be identified (CitationVanderschueren et al 2000). In as many as 50% of osteoporotic men, however, no etiology can be found (CitationVanderschueren et al 2000). The loss of skeletal integrity in aging men may be partially related to endocrine deficiencies, including vitamin D, androgen, and/or estrogen deficiency. While the consequences of vitamin D or estrogen deficiency in women have been well established, the skeletal impact of these (partial) age-related deficiencies in men remains to be clarified. As knowledge about the prevalence and etiology of osteoporosis in men increases, it will be recognized and treated in more men, in hopes of preventing fracture.
Risedronate
Risedronate [1-hydroxy-2-(3-pyridinyl)ethylidene bisphosphonic acid monosodium salt], (Cincinnati), is a potent pyridinyl bisphosphonate that has been shown to decreases the risk of vertebral and nonvertebral fractures in postmenopausal women with osteoporosis (CitationHarris et al 1999; CitationReginster et al 2000; CitationMcClung et al 2001). Recently it has been studied in men under a variety of clinical circumstances ().
Table 1 Summary of randomized controlled trials of risedronate for the treatment of male osteoporosis
Primary osteoporosis
Boonen et al recently reported in abstract from, a 2-year, double-blind, randomized, placebo-controlled, parallel group, multicenter study to determine the efficacy and safety of risedronate 35 mg once a week (CitationBoonen et al 2006), compared with placebo in men with osteoporosis. Men between the ages of 36 and 84 years, inclusive, who had osteoporosis defined as either a lumbar spine T-score ≤–2.5 and femoral neck T-score ≤–1 SD or a lumbar spine T-score ≤–1 and femoral neck T-score ≤–2 SD were randomized (2:1) to either risedronate 35 mg once a week (n = 191) or placebo (n = 93). All received daily supplementation of calcium (1000 mg) and vitamin D (400–500 IU) for 2 years. Efficacy was assessed by percentage change from baseline in lumbar spine and total proximal femur, femoral neck, and femoral trochanter bone mineral density (BMD) and bone turnover markers (BTMs) including type I collagen C- telopeptide (Ctx), type I collagen N-telopeptide/creatinine (Ntx/cr), and bone specific alkaline phosphatase (BSAP). BMD was measured at months 6, 12, 24, and end point.
The primary endpoint showed a statistically significant difference between risedronate and placebo groups in mean percent change from baseline to endpoint in lumbar spine BMD 4.53% (95% CI: 3.46%, 5.60%). The risedronate group had statistically significant increases compared with placebo in mean percentage change from baseline for lumbar spine BMD at months 6, 12, and 24, total proximal femur and femoral trochanter BMD at months 12, 24, and endpoint, and femoral neck BMD at month 24 and endpoint. The mean percentage change values for all BTMs were statistically significantly reduced in the risedronate group compared with baseline and with placebo at all time points measured.
The two treatment groups were comparable in overall percentages of patients with adverse events (AEs) (73%, placebo, 70% risedronate), serious AEs (16% placebo, 15%, risedronate), moderate to severe upper GI AEs (4% placebo, 3% risedronate) and overall musculoskeletal AEs (11% placebo, 12% risedronate). In this 2-year study, risedronate 35 mg once a week was safe and effective for the treatment of osteoporosis in men.
CitationRinge et al (2006) assessed the efficacy and safety of risedronate in the treatment of men with primary and secondary osteoporosis. They conducted a single-center, open label, randomized, prospective 1-year study where patients were randomized to risedronate (risedronate 5 mg/day plus calcium 1000 mg/day and vitamin D 800 IU/day) or control groups (alfacalcidol 1 μg/day plus calcium 500 mg/day or vitamin D 1000 IU/day plus calcium 800 mg/day). The mean age in the risedronate-treated group was 55.8 years and in the control group 58.0 years. Prevalent vertebral fractures were present in 53.2% of the risedronate group and 51.3% of the control group. BMD measurements, x-rays of the spine, and patient self-assessments of back pain were performed at baseline and 12 months. Blinded semi-quantitative fracture assessment was conducted by a radiologist. A total of 316 men with osteoporosis were enrolled in the trial (risedronate, n = 158; control, n = 158). At 1 year, lumbar spine BMD increased by 4.7% in the risedronate group versus an increase of 1.0% in the control group (p < 0.001). Significant increases in BMD at the total hip and femoral neck were also observed with risedronate compared with the control group. Over 1 year, 8 patients suffered new vertebral fractures (5.1%) in the risedronate-treated group, compared with 20 patients with new vertebral fractures (12.7%) in the control group, representing a 60% (p = 0.028) reduction in fractures. Nonvertebral fractures occurred in 10 patients (6.3%) in the risedronate-treated group compared with 17 patients (10.8%) in the control group. They concluded that daily treatment with risedronate for 12 months significantly increased BMD at the lumbar spine, femoral neck, and total hip and significantly reduced the incidence of new vertebral fractures.
Corticosteroid-induced bone loss
Limited information is available on the effect of bisphosphonates in men receiving corticosteroid therapy. CitationReid et al (2001) studied 184 men among the patients enrolled in two double-blind, placebo-controlled, 1-year studies with similar protocols. The studies evaluated the effects of risedronate in patients beginning corticosteroid treatment (prevention study) at a dose of at least 7.5 mg per day of prednisone or equivalent or continuing long-term treatment of corticosteroid (treatment study) at that dose. The men received either placebo or risedronate (2.5 mg or 5 mg) daily, along with calcium supplementation (500–1000 mg). Endpoints included differences in BMD at the lumbar spine, femoral neck, and femoral trochanter, assessment of vertebral fractures, changes in biochemical markers of bone turnover, and overall safety. The underlying diseases requiring corticosteroid treatment included rheumatoid arthritis, lung disease, polymyositis, polymyalgia rheumatica, temporal arteritis, and vasculitis. A total of 184 male patients received at least one dose of study drug (ITT population). The baseline characteristics of the 184 enrolled patients were similar between treatment groups. At baseline, the mean lumbar spine BMD was similar in the risedronate and placebo groups. The mean daily corticosteroid dose prior to enrollment was 19.4 mg (SD, 16.4) and the mean corticosteroid dose during the 1-year study was 14.2 mg (SD, 15.7); the corticosteroid doses were similar among the three treatment groups. Forty percent of men had prevalent (baseline) vertebral fractures; the prevalence was slightly higher in the risedronate 5 mg group (46%) than in the other groups.
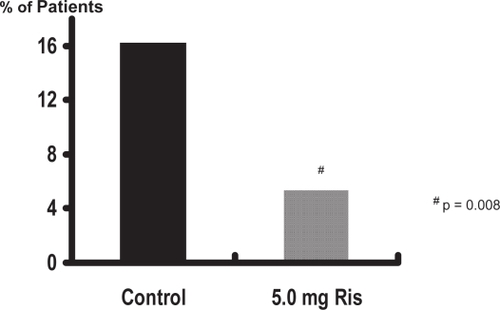
In the treatment study, risedronate 5 mg significantly (p < 0.01) increased lumbar spine BMD by 4.8% at the lumbar spine, 2.1% at the femoral neck, and 2.6% at the femoral trochanter compared with baseline values (). In the prevention study, bone loss was prevented with risedronate 5 mg; in the placebo group, BMD decreased significantly (p < 0.01) by 3.4%, 3.3%, and 3.4% in the lumbar spine, femoral neck, and trochanter, respectively, at 1 year (). The differences between risedronate 5 mg and placebo groups were significant at all skeletal sites in the prevention study (p < 0.01) and at the lumbar spine in the treatment study (p < 0.001). The 2.5 mg dose also had a positive effect on BMD, although of a lesser magnitude than the 5 mg dose. When the data from the two studies were combined, the incidence of vertebral fractures decreased 82.4% (95% CI: 36.6%, 95.1%) in the pooled risedronate groups compared with placebo (p = 0.008). Risedronate was well tolerated in men, with a similar incidence of upper gastrointestinal adverse events in the placebo and treatment groups. They concluded that daily treatment with risedronate increases bone density and decreases vertebral fracture risk within 1 year in men receiving corticosteroid therapy.
Figure 1 Risedronate in the treatment of corticosteroid-induced osteoporosis.
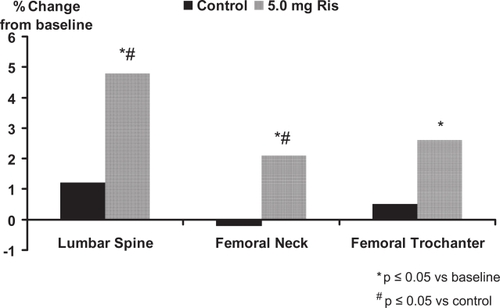
Figure 2 Risedronate in the prevention of corticosteroid-induced osteoporosis.
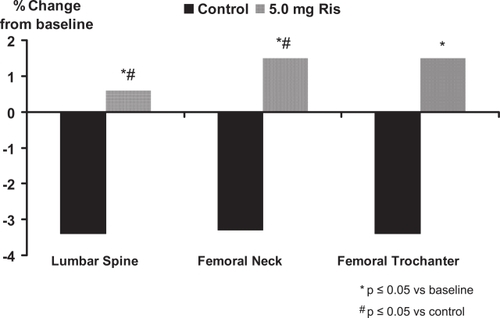
Figure 3 Vertebral fracture incidence.
Other conditions
Risedronate has been studied in a number of other conditions including post-stroke (CitationSato et al 2005), hyperthyroidism (CitationMajima et al 2006), inflammatory bowel disease (CitationHenderson et al 2006), transplantation (CitationTauchmanova et al 2003), leprosy (CitationKanaji et al 2006), and stress fractures in infantry recruits (CitationMilgrom et al 2004).
Post-stroke
There is a high incidence of hip fractures in patients after hemiplegic stroke. Bone mineral density is decreased on the hemiplegic side in patients after stroke, correlating with the immobilization-induced bone resorption, the degree of paralysis, and hypovitaminosis D. CitationSato et al (2005) evaluated the effectiveness of risedronate on osteoporosis and the risk of hip fractures in men 65 years or older after stroke. They conducted an 18-month, randomized, double-blind trial of 280 male patients 65 years or older who were post-stroke, with 140 receiving a daily dose of 2.5 mg risedronate and the other 140 receiving placebo. The mean age in both groups was 76.3 years. There were no significant differences between the placebo group and risedronate group in Barthel Index, degree of hemiplegia, number of fallers, type of stroke, BMD, or biochemical indices of bone metabolism. Although the values of BMD on both hemiplegic and nonhemiplegic sides were within the reference range compared with the elderly general Japanese population, BMD on the hemiplegic side was significantly reduced compared with that of the nonhemiplegic side. Compared with the reference range of the elderly general Japanese population, both groups of patients had high levels of serum ionized calcium and urinary D-Pyr and low serum concentrations of PTH, 25-OHD, and 1,25-(OH)2D at baseline. Serum 25-OHD was outside of the reference range in both groups: 114.6 ± 21.7 ng/mL (45.9 ± 8.7 nmol/L) in the placebo group and 114.6 ± 16.7 ng/mL (45.9 ± 6.7 nmol/L) in the risedronate group.
During the study, a total of 269 falls occurred in the former group and 278 in the latter group, or 4.2 falls per patient per year for both groups. In the risedronate group, 28 (20%) of 140 patients fell at least once, and 15 (80%) fell twice or more; in the placebo group, 29 (21%) of 140 patients fell at least once, and 15 (79%) fell twice or more. The number of falls among fallers ranged from 1 to 12 in both groups.
Ten patients sustained hip fractures in the placebo group, and 2 hip fractures occurred in the risedronate group. The relative risk of a hip fracture was reduced with risedronate to 0.19 (95% CI: 0.04–0.89). Bone mineral density increased by 2.5% in the risedronate group and decreased by 3.5% in the placebo group (p < 0.001). Urinary deoxypyridinoline, a bone resorption marker, decreased by 58.7% in the risedronate group and by 37.2% in the placebo group. They concluded that treatment with risedronate increases bone mineral density and reduces hip fractures in elderly men who are post-stroke (CitationSato et al 2005).
Hyperthyroidism
It has been well established that hyperthyroidism leads to diminished BMD, and that a previous history of hyperthyroidism remains a risk factor for fractures. However, little is known about how to manage the reduction in BMD caused by hyperthyroidism. This study evaluated the efficacy of risedronate for the treatment of osteoporosis/osteopenia in patients with Graves’ disease (CitationMajima et al 2006). Of 34 Japanese male patients with newly diagnosed Graves’ disease, 27 with osteoporosis/osteopenia were included in this study. They were randomly divided into two groups by therapeutic regimen. Fourteen patients were treated with an antithyroid drug and risedronate and the control group consisted of 13 patients treated with the same antithyroid drug only. The mean age and BMI was 43.6 years and 22.86 in the risedronate group and 45.5 years and 22.34 respectively in the control group. BMD at the lumber spine, femoral neck, and distal radius were measured at baseline, and at 6 and 12 months after the trial. Bone-specific alkaline phosphatase and urinary N-terminal telopeptide of type I collagen normalized by creatinine were significantly more reduced in the risedronate treated group than in the control group after both 6 and 12 months. The percentage increases in BMD at the lumbar spine femoral neck and distal radius at 1 year were 6.6%, 4.2%, and 2.4% respectively for risedronate and were greater than in the control group. These beneficial effects of risedronate for patients with osteoporosis/osteopenia caused by Graves’disease may reduce risk of future fractures. They concluded that risedronate should be considered for the treatment of decreased bone mass associated with Graves’ disease.
Inflammatory bowel disease
Low bone density and fractures are common in patients with inflammatory bowel disease (IBD). CitationHenderson et al (2006) conducted a study to determine whether risedronate is safe and effective in preserving bone mass compared with calcium alone in IBD patients with low bone mass. They enrolled 61 ambulatory patients, 25 of whom were males, with Crohn’s disease (n = 31) or ulcerative colitis (n = 30) and low bone density in a double-blind placebo-controlled trial. Patients were randomized to 12 months of therapy with risedronate 5 mg or placebo. All received a 600 mg calcium supplement. Bone density using dual energy x-ray absorptiometry was performed at baseline and at 12 months. Disease activity, use of corticosteroid, and adverse events were noted. Forty-eight patients completed the trial. Compared with the placebo group, risedronate resulted in a 2.0% (95% CI: 0.02–3.97) and 1.9% (95% CI: 0.21–3.62) improvement in bone density at the spine and hip, respectively. IBD diagnosis, gender, therapy, and disease status had no effect on the results. There were no significant differences in the adverse events. They concluded that risedronate improved bone density at the spine and hip in patients with either Crohn’s disease or ulcerative colitis and low bone mass. These data suggest that risedronate is a safe and effective therapy to improve bone mass in these patients (CitationHenderson et al 2006).
Transplantation
In this prospective randomized study risedronate was evaluated in patients who had undergone allogeneic stem cell transplant (SCT) for hematological malignancies (CitationTauchmanova et al 2003). Thirty-four patients (18 females, 16 males, age 32 ± 10 years) with BMD T-score ≤–1.5 SD at least 6 months after SCT were treated with calcium 1 g/day and vitamin D 800 IU/day and randomized to receive (n = 17) or not receive (n = 17) oral risedronate 5 mg/day. The duration of treatment was 12 months. After 12 months, lumbar BMD increased (5.9 ± 1.7%, p < 0.05), compared with baseline in risedronate-treated patients and increased slightly (+1.1 ± 1.4%) in the placebo group. They concluded that treatment with risedronate for 12 months increased BMD significantly at the lumbar spine and prevented further bone loss at the femoral neck in long-term survivors after allogeneic stem cell transplantation.
Leprosy
CitationKanaji et al (2006) evaluated the therapeutic effect of risedronate in male osteoporotic patients with leprosy. Twenty-three male patients with leprosy, 63–87 years of age, were randomly divided into two groups, risedronate, 2.5 mg/day or placebo. The BMD of the lumbar spine (L2–L4) was measured by dual-energy X-ray absorptiometry (DXA), and urinary N-telopeptide cross-links (NTX) were assessed at baseline, 6 months, and 12 months after treatment. There were no significant differences in age, body mass index, BMD, or urinary NTX levels at baseline between the two groups. They showed that oral administration of risedronate prevented vertebral fractures. There were a mean of 0.82 new vertebral fractures per patient during the 12 months’ treatment in the risedronate group and 1.88 per patient in the placebo group. The number of incident vertebral fractures per patient in the risedronate group was significantly lower than those in the placebo group (p < 0.05), suggesting that risedronate treatment prevented incident vertebral fractures. Increased lumbar BMD and significant reductions of bone turnover as measured by urinary NTX levels were seen with risedronate compared with placebo. These findings suggest that oral administration of risedronate contributes to the prevention of vertebral fractures by suppressing bone resorption and increasing in lumbar BMD in the elderly male patients with leprosy.
Stress fractures
A randomized, double-blind, placebo controlled trial of 324 new infantry recruits known to be at high risk for stress fracture was conducted (CitationMilgrom et al 2004). Recruits were given a loading dose of 30 mg of risedronate or placebo daily for 10 doses during the first 2 weeks of basic training and then a once a week maintenance dose for the following 12 weeks. Recruits were monitored by biweekly orthopedic examinations during 15 weeks of basic training for stress fractures. Bone scans for suspected tibial and femoral stress fractures and radiographs for suspected metatarsal stress fractures were used to verify stress fracture occurrence. No statistically significant difference in the tibial, femoral, metatarsal, or total stress fracture incidence between the treatment group and the placebo group was seen and it was concluded that prophylactic treatment with risedronate in a training population at high risk for stress fracture using a maintenance dosage for the treatment of osteoporosis does not lower stress fracture risk.
Summary
Osteoporosis in men is a significant cause of morbidity and mortality. Risedronate is effective in increasing BMD in primary and corticosteroid-induced osteoporosis in men and more importantly the prevention of vertebral fractures within the first year of therapy in corticosteroid-treated men. Risedronate is also effective in the prevention of hip fractures post stroke and vertebral fractures in those with leprosy. Risedronate maintained BMD in those with Graves’ disease, inflammatory bowel disease, cystic fbrosis and transplantation. Risedronate was ineffective in the prevention of stress fractures in infantry recruits.
References
- BoonenSDelmasPDWenderothDH2006Risedronate shown to be safe and effective in men with osteoporosis in a 2-year, double-blind, randomized, placebo-controlled, multicentre studyOsteoporos Int17S23031
- CohenSLevyRMKellerM1999Risedronate therapy prevents corticosteroid-induced bone loss: a twelve-month, multicenter, randomized, double-blind, placebo-controlled, parallel-group studyArthritis Rheum4223091810555025
- DiamondTH2005Pharmacotherapy of osteoporosis in menExpert Opin Pharmacother6455815709882
- HarrisSTWattsNBGenantHK1999Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis: a randomized controlled trial. Vertebral Efficacy With Risedronate Therapy (VERT) Study GroupJAMA28213445210527181
- HawkesWGWehrenLOrwigD2006Gender differences in functioning after hip fractureJ Gerontol A Biol Sci Med Sci614959916720747
- HendersonSHoffmanNPrinceR2006A double-blind placebo-controlled study of the effects of the bisphosphonate risedronate on bone mass in patients with inflammatory bowel diseaseAm J Gastroenterol1011192316405543
- JiangHXMajumdarSRDickDA2005Development and initial validation of a risk score for predicting in-hospital and 1-year mortality in patients with hip fracturesJ Bone Miner Res2049450015746995
- KanajiAHigashiMNamisatoM2006Effects of risedronate on lumbar bone mineral density, bone resorption, and incidence of vertebral fracture in elderly male patients with leprosyLepr Rev771475316895071
- LookerACOrwollESJohnstonCCJr1997Prevalence of low femoral bone density in older U.S. adults from NHANES IIIJ Bone Miner Res121761689383679
- McClungMRGeusensPMillerPDEffect of risedronate on the risk of hip fracture in elderly women. Hip intervention program study groupN Engl J Med3443334011172164
- MajimaTKomatsuYDoiK2006Clinical significance of risedronate for osteoporosis in the initial treatment of male patients with Graves’ diseaseJ Bone Miner Metab241051316502116
- MeltonLJIIIAtkinsonEJO’ConnorMK1998Bone density and fracture risk in menJ Bone Miner Res131915239844110
- MilgromCFinestoneANovackV2004The effect of prophylactic treatment with risedronate on stress fracture incidence among infantry recruitsBone354182415268892
- PoorGAtkinsonEJLewallenDG1995aAge-related hip fractures in men: clinical spectrum and short-term outcomesOsteoporos Int5419268695962
- PoorGAtkinsonEJO’FallonWM1995bDeterminants of reduced survival following hip fractures in menClin Orthop Relat Res26065
- ReginsterJMinneHWSorensenOH2000Randomized trial of the effects of risedronate on vertebral fractures in women with established postmenopausal osteoporosis. Vertebral efficacy with risedronate therapy (VERT) Study GroupOsteoporos Int11839110663363
- ReidDMAdamiSDevogelaerJP2001Risedronate increases bone density and reduces vertebral fracture risk within one year in men on corticosteroid therapyCalcif Tissue Int692424711730260
- ReidDMHughesRALaanRF2000Efficacy and safety of daily risedronate in the treatment of corticosteroid-induced osteoporosis in men and women: a randomized trial. European corticosteroid-induced osteoporosis treatment studyJ Bone Miner Res1510061310841169
- RingeJD2003[Osteoporosis in men]Dtsch Med Wochenschr1289252812715292
- RingeJDFaberHFarahmandP2006Efficacy of risedronate in men with primary and secondary osteoporosis: results of a 1-year studyRheumatol Int264273116001181
- SatoYIwamotoJKanokoT2005Risedronate sodium therapy for prevention of hip fracture in men 65 years or older after strokeArch Intern Med16517434816087822
- SawkaAMAdachiJDPapaioannouA2004Are there differences between men and women prescribed bisphosphonate therapy in canadian subspecialty osteoporosis practices?J Rheumatol3119939515468365
- TauchmanovaLSelleriCEspositoM2003Beneficial treatment with risedronate in long-term survivors after allogeneic stem cell transplantation for hematological malignanciesOsteoporos Int1410131914517597
- TenenhouseAJosephLKreigerN2000Estimation of the prevalence of low bone density in canadian women and men using a population-specific DXA reference standard: the canadian multicentre osteoporosis study (CaMos)Osteoporos Int1189790411199195
- VanderschuerenDBoonenSBouillonR2000Osteoporosis and osteoporotic fractures in men: a clinical perspectiveBaillieres Best Pract Res Clin Endocrinol Metab1429931511035908