Abstract
Obesity and hypertension are major public health concerns in the US. We examined the relationship between body mass index (BMI) and blood pressure in older Mexican Americans using data from the Hispanic Established Population for the Epidemiological Study of the Elderly (EPESE), a longitudinal study of Mexican Americans aged 65 and over residing in the southwestern US. The study sample was 2404 older Mexican American adults with a mean age of 72.6 years of age at baseline (1993–4). Both systolic and diastolic blood pressures were higher in subjects with high BMI categories. The rate of change in systolic blood pressure and diastolic blood pressure were −0.11 mm Hg and −0.32 mm Hg per year over a 7-year period, respectively. The rate of decline in systolic and diastolic blood pressure over a 7-year period was greater in subjects with BMI categories of 25–<30 kg/m2 and 30–<35 kg/m2 as compared with those subjects with in the lowest and in the highest BMI categories. Hypertension is one of the most prevalent medical conditions affecting older adults. Understanding possible modifiable risk factors that may play a role in the management of hypertension will be beneficial.
Keywords:
Introduction
Obesity has become a major health concern in the US (CitationKuczmarski et al 1994). The prevalence of obesity has continued to rise since the early 1990s and is now estimated to be the second leading cause of preventable death after cigarette smoking in the US (CitationMokdad et al 1999; CitationBrown et al 2000). Obesity has been associated with a worse quality of life, numerous other medical problems, and higher mortality (CitationMokdad et al 1999; CitationYan et al 2004). Obesity has been associated with medical problems such as cardiovascular diseases, type 2 diabetes, gallbladder disease, cancers of several sites, osteoarthritis, hypertension, and hyperlipidemia (CitationHubert et al 1983; CitationVan Itallie 1985; CitationPi-Sunyer 1991; CitationFeskens et al 1992). Even though the association between obesity and mortality seems to decline with advancing age, excess weight is still a risk factor for morbidity and mortality in the elderly (CitationSjostrom 1992; CitationStevens et al 1998).
An association between obesity and hypertension has been found in both younger and older individuals (CitationVan Itallie 1985). Ischemic heart disease mortality has been related to systolic and diastolic blood pressure (CitationHubert et al 1983; CitationBots et al 1991; CitationBenfante et al 1992; CitationGlynn et al 1995). Data from the Framingham study indicate that hypertension and obesity are both risk factors for the development of congestive heart failure, one of the major causes of mortality and morbidity in the older adult (CitationLevy et al 1996; CitationKenchaiah et al 2002). Even in very old age, blood pressure levels have been associated with cardiovascular diseases (CitationLewington et al 2002).
One practical indicator of excess weight is the body mass index (BMI). A high BMI has been associated with higher blood pressure (CitationAlpert and Hashimi 1993; CitationMasaki et al 1997; CitationBrown et al 2000). In a cross–sectional study CitationColin Bell and colleagues (2002) found that higher BMI was associated with a higher prevalence of hypertension in Chinese, non-Hispanic Whites, non-Hispanic Blacks, and Mexican Americans. Further, another study found that even when the BMI is within the normal range of 21 kg/m2 to 24.9 kg/m2, an individual with a high normal BMI is at an increased risk of type 2 diabetes, hypertension, coronary heart disease, and cholelithiasis (CitationWillett et al 1999).
Hypertension in older Mexican Americans is a common problem that is frequently under-treated (CitationSatish et al 1998). Indeed, large numbers of older Mexican Americans are unaware that they have high blood pressure (CitationSatish et al 1997). A high BMI could be a potential modifiable risk factor for hypertension. This study examines the association between BMI and systolic and diastolic blood pressures in older Mexican Americans over a 7-year period.
Methods
Sample and procedures
Data used are from the Hispanic Established Population for the Epidemiological Study of the Elderly (H-EPESE), a longitudinal study of Mexican Americans aged 65 and over, residing in Texas, New Mexico, Colorado, Arizona, and California. The Hispanic EPESE was modeled after previous EPESE conducted in New Haven, East Boston, rural Iowa, and North Carolina (CitationMarkides et al 1996, Citation1999). Subjects were selected from five southwestern states (Texas, California, Arizona, Colorado, and New Mexico) using area probability sampling procedures. The sample and its characteristics have been described elsewhere (CitationMarkides et al 1996, Citation1999). The sampling procedure assured a sample that is generalizable to approximately 500 000 older Mexican Americans living in the southwest (CitationMarkides et al 1996, Citation1999). In-home interviews were conducted in Spanish or English depending on the respondent’s preference. The response rate was 83%, which was comparable with the other EPESE studies (CitationMarkides et al 1996, Citation1999). At the time of the baseline assessment during 1993–1994, 2873 subjects (94.2%) were interviewed in person and 177 (5.8%) were interviewed by proxy. The present study used baseline data (1993–94), data from a 2-year follow-up (1995–96), from a 5-year follow-up (1998–99), and from a 7-year follow-up assessment (2000–2001).
Of the 3050 subjects interviewed at baseline, 313 subjects were excluded due incomplete data on systolic and diastolic blood pressure measures (197 were interviewed by proxy and 116 were refusals), 281 subjects had no weight and height data, and 52 subjects had incomplete data on covariates. Subjects excluded were significantly more likely to be older, to have ever had a heart attack, a stroke, higher number of physician visits, and to have been hospitalized compared with those included in the study. Thus, the analysis sample consisted of 2404 subjects with complete data on weight, height, blood pressure at baseline, and complete data on all covariates. At end of the 7-year follow-up (2000–2001), 1403 subjects were re-interviewed, 105 subjects refused to be re-interviewed, 242 subjects were lost to follow-up, and 654 subjects were confirmed dead through the National Death Index (NDI) and reports from relatives.
Measures
Body mass index
Anthropometric measurements were collected in the home using the methods and instructions employed in other EPESE studies (CitationMarkides et al 1996, Citation1999). Height was measured using a tape placed against the wall. Weight was measured using a calibrated Metro 9800 measuring scale. The BMI was computed by dividing weight in kilograms by height in meters squared (kg/m2). BMI was grouped according to the National Institutes of Health (NIH) obesity standards (<18.5 kg/m2 = underweight; 18.5–24.9 kg/m2 = normal weight; 25.0–29.9 kg/m2 = overweight; 30.0–34.9 kg/m2 = obesity category I; 35.0–39.9 kg/m2 = obesity category II; and ≥40.0 kg/m2 = extreme obesity (NIH 1998).
Blood pressure
Blood pressures were measured by standard mercury sphygmomanometer after the subject was comfortably seated using an appropriate cuff size. Two sitting blood measures were taken for each subject with a 60-sec interval between the two according to the standard protocol used in the third National Health and Nutrition Examination (CitationBurt et al 1995). All of the interviewers underwent a 3-day special training in the use of a standardized protocol for measurement of blood pressure. Satisfactory performance on both a standardized videotape test and a live performance on volunteer subjects was a requirement for completion of the training. Interviewers were required to review the training videotape monthly and to undergo retraining at each follow-up. An average systolic and diastolic blood pressure was calculated for each subject.
Covariates
Baseline sociodemographic variables included age, gender, marital status, and years of formal education. We assessed the presence of medical conditions by asking if respondents had ever been told by a doctor that they had hypertension, diabetes, heart attack, or stroke. Subjects with self-reported hypertension were also asked if they were currently taking any medication for high blood pressure. Self-reported hypertension was categorized as no hypertension, hypertension with current treatment, and hypertension without current treatment. Waist circumference was measured at the level of the umbilicus with the subject standing. The measurement, taken with a non-stretchable measuring tape, was done over no more than one layer of outer clothing and recorded in centimeters to the nearest millimeter. A waist circumference in women >88 cm and >102 cm in men was considered high (CitationNIH 1998). Smoking status was assessed by asking subjects whether they were a current smoker or not. Physician utilization was assessed by the following question: “How many times in the past 12 months have you visited with a medical doctor?” Hospital utilization was assessed by the following question: “Did you experience an illness or injury that required staying overnight or longer in a hospital in the last year?”
Analysis
Analysis of variance and post hoc Tukey test was used to examine the distribution of systolic and diastolic blood pressure by age and BMI categories at baseline. General linear mixed model using the MIXED procedure in SAS program was used to test the relationship between repeated measures of BMI and blood pressure (systolic and diastolic) over a 7-year period while adjusting for age, gender, education, marital status, smoking status, waist circumference, medical conditions (hypertension with and without treatment, diabetes, heart attack, and stroke), and healthcare use (physician visits and hospitalization). Time was treated as a continuous variable. All the variables were analyzed as time-dependent covariates (potential to change as time progresses) except variables of age, gender, and education.
Three mixed models were constructed to test the relationship between BMI and blood pressure over a 7-year period. Model 1 included age, gender, years of formal education, marital status, BMI, and time. In model 2, an interaction term – BMI categories × time – were added to estimate the effect of BMI categories on the rate of change on blood pressure (slope) over time. The time interaction represents the estimated effect of BMI on the rate of the change in systolic and diastolic blood pressures. In model 3, smoking status, waist circumference, medical conditions, and health care use were added.
The mixed model was chosen for several reasons. First, the model best accounted for missing or incomplete observations and makes it possible to use all available information. Second, it allowed for modeling of time-dependent change in the variables (BMI, systolic and diastolic blood pressure, among others) as well as time-dependent change in the magnitude of association between variables. Finally, because the H-EPESE study contains repeated measures over seven years, mixed models allow more flexibility in modeling the effects of time on outcomes (CitationLiang and Zeger 1986; CitationZeger and Liang 1986). All analyses were performed using the SAS System for Windows, Version 9.1.3 (SAS Institute, Cary, NC).
Results
Table presents descriptive characteristics of the sample at baseline. The study sample of 2404 older Mexican American adults had a mean age of 72.6 years with 58.2% being female and 55.7% being married. The mean years of formal education was 4.9. The mean BMI was 27.8 kg/m2. Less than 2% of the subjects (42) had a BMI <18.5 kg/m2, 40% of the subjects (972) had a BMI of 25–<30 kg/m2, and 29.9% (718) had a BMI of ≤30 kg/m2. The mean of systolic and diastolic blood pressures were 134.6±Standard Deviation (SD) of 15.9 mm Hg and 80.4±10.5 mm Hg, respectively. Self-reported hypertension (41.1%), diabetes (23.8%), and stroke (10.4%) were the most prevalent medical conditions. More than 70% of females and 40% of males had a high abdominal circumference.
Table 1 Descriptive characteristic of the sample at baseline (N=2404)
Figure shows mean systolic and diastolic blood pressures by years of follow-up. The mean systolic and diastolic blood pressures at baseline were 135 mm Hg and 80.4 mm Hg, respectively, and 132 mm Hg and 77.1 mm Hg by the end of the 7-years of follow-up (p<0.0001 for both systolic and diastolic blood pressures).
Figure 1 Mean systolic and diastolic blood pressures by years of follow-up (N=2404).
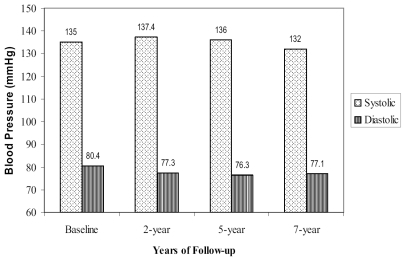
Figure shows average mean systolic and diastolic blood pressures over a 7-year period by age categories at baseline. Average mean systolic blood pressure by age categories at baseline were not statistically different during the follow-up period. The range of average mean systolic blood pressure was 135.3 mm Hg for those between the ages of 65 to 70 years of age to 134.1 mm Hg for those 80 years old and older. The range of average mean diastolic blood pressure was 79.7 mm Hg for the group 65 to 70 years of age to 76.4 mm Hg for those 80 year old and older (p<0.0001 for both systolic and diastolic blood pressures).
Figure 2 Average mean systolic and diastolic blood pressures over a 7-year period by age categories at baseline (N=2404).
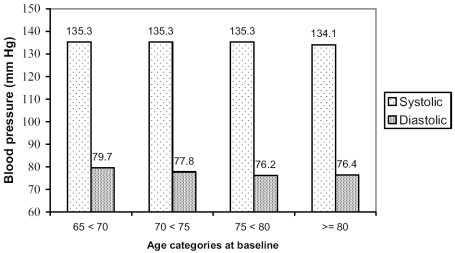
Figure shows average mean of systolic and diastolic blood pressures over a 7-year period by BMI categories at baseline. Both mean systolic and diastolic blood pressures were significantly higher as BMI category increases (p-value<0.0001). The average mean systolic blood pressure ranges from 127.6 mm Hg for subjects with a BMI <18.5 mm Hg to 136.3 mm Hg to 136.3 mm Hg for subjects with a BMI ≥40. The average mean diastolic blood pressure ranges from 73.5 mm Hg for subjects with a BMI <18.5 mm Hg to 79.9 mm Hg for subjects with a BMI ≥40.
Figure 3 Average mean systolic and diastolic blood pressures over a 7-year period by body mass index (BMI) categories at baseline (N=2404).
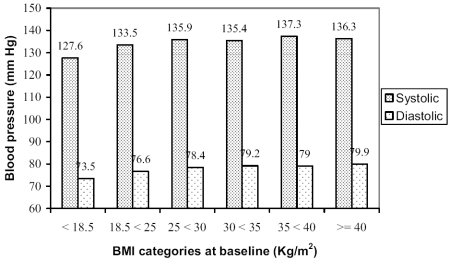
Table presents the general linear mixed model estimates for systolic blood pressure (mm Hg) as a function of BMI categories at baseline over a 7-year period. In model 1, the rate of change in systolic blood pressure was −0.26 mm Hg per year. There was a significant association at each time point of follow-up between BMI categories and systolic blood pressure, after controlling for age, time, gender, marital status, and years of formal education. We found that the higher the BMI, the greater the systolic blood pressure. Model 2 tests for the interaction between BMI and time of follow-up (slope of systolic blood pressure over time). The time-interaction represents the estimated effect of BMI on the rate of the change in systolic blood pressure. There were significant interactions in subjects with a BMI of 25 kg/m2 <30 kg/m2 and a BMI of 30 kg/m2 <35 kg/m2 indicating that subjects with these BMI categories had a significantly greater decline in systolic blood pressure over time compared with those in the lowest and in the highest BMI categories. In model 3, after controlling for all covariates, the interaction terms remained statistically significant (estimate=−0.36, SE=0.17, p<0.01 and estimate=−0.52, SE=0.20, p<0.01, respectively). Other factors such as being female, being married, higher levels of education, heart attack, and being hospitalized in the year prior to the interview were significantly associated with a decline in systolic blood pressure. A prior diagnosis of hypertension with or without treatment was significantly associated with increases in systolic blood pressure.
Table 2 General linear mixed models estimates for systolic blood pressure (mm Hg) as a function of BMI categories at baseline over 7-year period among older Mexican Americans (N=2404)
Table presents the general linear mixed model estimates for diastolic blood pressure (mm Hg) as a function of BMI categories at baseline over a 7-year period. In model 1, the rate of change in diastolic blood pressure was −0.55 mm Hg per year. There was a significant association at each time point of follow-up between BMI categories and diastolic blood pressure, after controlling for age, time, gender, marital status, and years of formal education. We found that the higher the BMI, the greater the diastolic blood pressure. Model 2 tests for the interaction between BMI and time of follow-up (slope of diastolic blood pressure over time). The time-interaction represents the estimated effect of BMI on the rate of the change in diastolic blood pressure. There were significant interactions for subjects with a BMI of 25 kg/m2 <30 kg/m2, BMI of 30 kg/m2 <35 kg/m2, and BMI of 35 kg/m2 <40 kg/m2 (estimate=−0.35, SE=0.12, p<0.001, estimate=−0.46, SE=0.13, p<0.001, and estimate=−0.46, SE=−0.21, p<0.01, respectively), indicating that subjects with these BMI categories had a significantly greater decline in diastolic blood pressure over time when compared with those in the lowest and in the highest BMI categories. In model 3, after controlling for all covariates, the interaction terms that remained statistically significant were for a BMI of 25 kg/m2 <30 kg/m2 and a BMI of 30 kg/m2 <35 kg/m2. Other factors such as older age, being female, being a current smoker, heart attack, diabetes, stroke, and being hospitalized in the past year were significantly associated with a decline in diastolic blood pressure. Self-reported hypertension with or without treatment and high abdominal circumference were significantly associated with increases in diastolic blood pressure.
Table 3 General linear mixed models estimates for diastolic blood pressure (mm Hg) as a function of BMI categories at baseline over 7-year period among older Mexican Americans (N=2404)
The major findings of this study were first, the rate of change in systolic blood pressure was −0.11 mm Hg per year and the rate of change in diastolic blood pressure was −0.32 mm Hg per year after controlling for all covariates. Second, both systolic and diastolic blood pressures were higher in subjects with high BMI categories at each time of follow-up and the higher the BMI the greater systolic and diastolic blood pressures. Third, the rate of decline in systolic and diastolic blood pressure over a 7-year period was greater in subjects with BMI categories of 25 kg/m2–<30 kg/m2 and 30 kg/m2–<35 kg/m2 compared with those in the lowest and in the highest BMI categories.
Discussion
Our findings are consistent with previous studies on the relationship between BMI and blood pressure (CitationPi-Sunyer 1993; CitationMasaki et al 1997; CitationBrown et al 2000; CitationColin Bell et al 2002). High BMI in middle aged adults has been associated with increased blood pressure and coronary artery disease (CitationPi-Sunyer 1993; CitationMasaki et al 1997; CitationBrown et al 2000; CitationColin Bell et al 2002). A cross–sectional study by CitationColin Bell and colleagues (2002) examining ethnic differences in the strength of the association between BMI and hypertension found that higher BMI was associated with a higher prevalence of hypertension in four ethnic groups including Mexican Americans. A study by CitationMasaki and colleagues (1997) found in a cross-sectional analysis of 1348 elderly Japanese American men and women aged 60 to 82 that BMI was associated with systolic and diastolic blood pressure after adjusting for multiple variables. In the present study we found that systolic and diastolic blood pressures were significantly higher in subjects with higher BMI at each time point of follow-up.
One possible explanation for the higher systolic and diastolic blood pressures with higher BMI in older Mexican Americans may be metabolic changes caused by high body weight in this population. The association between obesity and high blood pressure has been recognized for decades, but the underlying mechanism is still poorly understood (CitationAntic et al 2003). Some of the possible pathways for obesity to induce hypertension are sympathetic activation with vasoconstriction, endothelial dysfunction, and positive sodium balance causing a rise in blood pressure (CitationAntic et al 2003).
We also found a significant yearly decrease of systolic and diastolic blood pressure in our study group. Previous studies have shown that diastolic blood pressure tends to decrease after ages 60–75 (CitationLandahl et al 1986; CitationFranklin et al 1997). CitationLandahl and colleagues (1986) found in a sample of 2550 subjects an increase in the mean systolic blood pressure for those 50 to 70 years of age and a moderate decrease in the mean systolic blood pressure after the early 70’s.
However, CitationFranklin and colleagues (1997) found that systolic blood pressure continues increasing at least into the early 80s’ in a sample of 2036 subjects. Our study group is much older with a mean age of 72 at the beginning of the study. This age difference could be one factor of why the findings from this study are different from those of CitationLandahl et al (1986). CitationFranklin et al (1997) excluded subjects with apparent coronary artery disease or those receiving antihypertensive therapy at baseline or before the study began. Their subjects in general have less risk factors for cardiovascular diseases and this may explain the different findings in systolic blood pressure. Also, other possible explanations for decline in systolic blood pressure in our study over time might be changes in dietary habits, changes in subject’s physician practices (blood pressure management), and changes in activity level. However, these possible explanatory factors were not available in our study.
Several longitudinal and cross-sectional studies have shown that systolic and/or diastolic blood pressures decline in older age (CitationLanger et al 1993; CitationTervahauta et al 1994; CitationHakala and Tilvis 1998; CitationSatish et al 2001). For example, CitationLanger and colleagues (1993) studying subjects aged 75 years and older in Rancho Bernardo, California found that 55% of the subjects had >−5 mm Hg diastolic blood pressure decrease over eleven years. Another study by CitationSatish and colleagues (2001) using a prospective cohort of 9696 community dwelling persons aged 65 years and older found that falling systolic and diastolic blood pressure was common among older adults and was a marker for declining health.
Some of the proven benefits of weight loss for obese individuals are decreased blood pressure in hypertensive patients (CitationStevens et al 1993), improvements in the lipid profile, and decreased insulin resistance, among others (CitationWeinstock et al 1998). A review of the major hypertension treatment trials in the elderly demonstrated a statistically significant decrease in the occurrence of congestive heart failure as a result of treatment for three to five years (CitationMoser and Hebert 1996). Despite these positive advances, the benefits of hypertension treatment and the ideal blood pressure in the very old are not clear at this time.
Our study has some limitations. First, blood pressure was measured two times, 1 minute apart, on a single occasion. This might have reduced the precision on an individual’s blood pressure. However, findings from the Framingham study and a meta-analysis of nine prospective epidemiological studies have shown that blood pressure measurement on a single occasion will predict future stroke and coronary heart disease as well as a series of blood pressure measurements does (CitationKannel et al 1970; CitationGordon et al 1991; CitationCollins and MacMahon 1994). Second, we were limited to self-reports of medical conditions. Third is the potential bias inherent in using follow-up survivor subjects. Thus, our study sample may represent the healthier subjects. Our study has several strengths including its large community-based sample, its prospective design, and its exploration of potential factors affecting blood pressure in older Mexican Americans, a rapidly growing segment of the older population in the US. Another important strength of our study is the use of mixed models, an analytic approach that allowed the use of all available data and evaluation of time-dependent effects.
In conclusion, we found a significant higher systolic and diastolic blood pressure in subjects with higher BMI categories and a significant decrease in both systolic and diastolic blood pressure after controlling for multiple variables. Hypertension is one of the most prevalent medical conditions affecting older adults. Understanding possible modifiable risk factors that may play a role in the management of hypertension will be beneficial. Further, studies addressing the benefits of weight reduction in hypertensive older adults need to be conducted.
Acknowledgements
This study was supported by grants, AG10939 and AG17638, from the National Institute on Aging, USA, and in part by the UTMB Center for Population Health and Health Disparities –5P50CA105631. The Bureau of Health Professions’ Geriatric Academic Career Award 1 K01 HP 00056-01 supports Dr Amador’s work.
Reference
- AlpertMAHashimiMW1993Obesity and the heartAm J Med Sci306117238362892
- AnticVDullooAMontaniJP2003Multiple mechanisms Involved in obesity-induced hypertensionHeart Lung Circ12849316352114
- BenfanteRReedDFrankJ1992Do coronary heart disease risk factors measured in the elderly have the same predictive roles as in the middle aged? Comparisons of relative and attributable risksAnn Epidemiol2273821342278
- BotsMLGrobbeeDEHofmanA1991High blood pressure in the elderlyEpidemiol Rev132943141765115
- BrownCDHigginsMDonatoKA2000Body mass index and the prevalence of hypertension and dyslipidemiaObes Res86051911225709
- BurtVLWheltonPRoccellaEJ1995Prevalence of hypertension in the US adult population: Results from the Third National Interview and Nutrition Examination Survey, 1988–1991Hypertension25305137875754
- Colin BellAAdairLSPopkinBM2002Ethnic differences in the association between body mass index and hypertensionAm J Epidemiol1553465311836199
- CollinsRMacMahonS1994Blood pressure, antihypertensive drug treatment and the risks of stroke and coronary heart diseaseBr Med Bull50272988205459
- FeskensEJBowlesCHKromhoutD1992A longitudinal study on glucose tolerance and other cardiovascular risk factors: associations within an elderly populationJ Clin Epidemiol452933001569427
- FranklinSSGustinW4thWongND1997Hemodynamic patterns of age-related changes in blood pressure. The Framingham Heart StudyCirculation96308159236450
- GlynnRJFieldTSRosnerB1995Evidence for a positive linear relation between blood pressure and mortality in elderly peopleLancet34582597898229
- GordonTSorliePKannelWB1991Problems in the assessment of blood pressure: The Framingham StudyInt J Epidemiol5327341010660
- HakalaSMTilvisRS1998Determinants and significance of declining blood pressure in old age. A prospective birth cohort studyEur Heart J19187289886731
- HubertHBFeinleibMMcNamaraPM1983Obesity as an independent risk factor of cardiovascular disease: a 26-year follow-up of participants in the Framingham Heart StudyCirculation67968776219830
- KannelWBWolfPAVerterJ1970Epidemiologic assessment of the role of blood pressure in stroke. The Framingham studyJAMA214301105469068
- KenchaiahSEvansJCLevyD2002Obesity and the risk of heart failureN Engl J Med3473051312151467
- KuczmarskiRJFlegalKMCampbellSM1994Increasing prevalence of overweight among US adults. The National Health and Nutrition Examination Surveys, 1960 to 1991JAMA272205118022039
- LandahlSBengtssonCSigurdssonJA1986Age-related changes in blood pressureHypertension8104493770866
- LangerRDCriquiMHBarrett-ConnorEL1993Blood pressure change and survival after age 75Hypertension2255198406660
- LevyDLarsonMGVasanRS1996The progression from hypertension to congestive heart failureJAMA2751557628622246
- LiangKYZegerSL1986Longitudinal data analysis using generalized linear modelsBiometrika731322
- LewingtonSClarkeRQizilbashN2002Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studiesLancet36019031312493255
- MarkidesKSStroup-BenhamCAGoodwinJS1996The effect of medical conditions on the functional limitations of Mexican-American elderlyAnn Epidemiol6386918915469
- MarkidesKSStroup-BenhamCABlackS1999The health Mexican American elderly: selected findings from the Hispanic EPESEWykleMLFordABServing minority elders in the 21st CenturyNew YorkSpringer Pub Co, Inc7290
- MasakiKHCurbJDChiuD1997Association of body mass index with blood pressure in elderly Japanese American men: the Honolulu Heart ProgramHypertension2967379040455
- MokdadAHSerdulaMKDietzWH1999The spread of the obesity epidemic in the United States, 1991–1998JAMA28215192210546690
- MoserMHebertPR1996Prevention of disease progression, left ventricular hypertrophy and congestive heart failure in hypertension treatment trialsJ Am Coll Cardiol271214188609345
- [NIH] National Institutes of Health1998Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults –the evidence reportObes Res6Suppl 251S209S9813653
- Pi-SunyerFX1991Health implications of obesityAm J Clin Nutr531595S1603S2031492
- Pi-SunyerFX1993Medical Hazard of ObesityAnn Intern Med119655608363192
- SatishSMarkidesKSZhangD1997Factors influencing unawareness of hypertension among older Mexican AmericansPrev Med26(5 Pt 1)645509327472
- SatishSStroup-BenhamCAEspinoDV1998Undertreatment of hypertension in older Mexican AmericansJ Am Geriatr Soc46405109560060
- SatishSZhangDDGoodwinJS2001Clinical significance of falling blood pressure among older adultsClin Epidemiol549617
- StevensVJCorriganSAObarzanekE1993Weight loss intervention in phase 1 of the Trials of Hypertension Prevention. The TOHP Collaborative Research GroupArch Intern Med153849588466377
- StevensJCaiJPamukER1998The effect of age on the association between body-mass index and mortalityN Engl J Med338179414324
- SjostromLV1992Mortality of severely obese subjectsAm J Clin Nutr55516S523S1531097
- TervahautaMPekkanenJEnlundH1994Change in blood pressure and 5-year risk of coronary heart disease among elderly men: the Finnish cohorts of the seven countries studyJ Hypertens12118397836735
- Van ItallieT1985Health implications of overweight and obesity in the United StatesAnn Intern Med10398384062130
- WeinstockRSDaiHWaddenTA1998Diet and exercise in the treatment of obesity. Effects of 3 interventions on insulin resistanceArch Intern Med15824779855386
- WillettWCDietzWHColditzGA1999Guidelines for healthy weightN Engl J Med3414273410432328
- YanLLDaviglusMLLiuK2004BMI and health-related quality of life in adults 65 years and olderObes Res12697614742844
- ZegerSLLiangKY1968Longitudinal data analysis for discrete and continuous outcomesBiometrics42121303719049