Abstract
A 51-year-old male patient with a past history of lung tuberculosis was referred to our clinic for routine control. The patient reported no complaints and chest X-ray was normal. Three-dimensional thoracic computed tomography revealed a balanced-type double aortic arch with no compression of trachea or esophagus.
Vascular rings, which constitute less than 1% of the congenital heart diseases, were first identified by Gross in 1945.Citation1 Double aortic arch (DAA) is the most frequent form of vascular rings. DAA may surround trachea and esophagus and, thus, may cause compression of these structures. If the compression is severe, symptoms such as dyspnea, recurrent pneumonia, stridor, dysphagia, and feeding difficulties may be observed at birth. However, when compression is minimal, DAA can remain undiagnosed until adulthood.Citation2 We report an asymptomatic case with a DAA in whom anatomical boundaries and branches of DAA were clearly demonstrated using three dimensional computed tomography (CT).
Case report
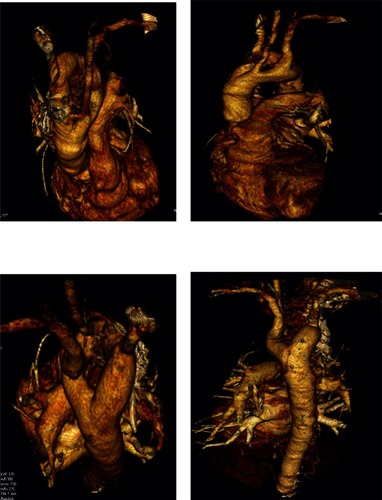
A 51-year-old male patient with a past history of lung tuberculosis presented for routine control. The patient reported no complaints. He smoked 40 packets of cigarettes per year and had suffered from tuberculosis 20 years ago and had been treated. Physical examination and laboratory findings were within normal limits; chest X-ray showed bilateral hyperlucency (). Chest CT revealed DAA surrounding the trachea on both sides. Left and right arches were equal in size although the right arch was located 5 mm higher than the left (). A three-dimensional CT scan was taken (1) to obtain better anatomic views and (2) to clearly identify its relation to neighboring structures (). These images show clearly that the DAA is a balanced type and there is no compression of either trachea or esophagus. Echocardiography was normal. Bronchoscopy was not performed due to lack of respiratory symptoms.
Figure 1 Bilateral hyperlucency is visible in this X-ray.
Figure 2 Left and right arches in the trachea are equal in size, but the right arch was 5 mm higher than the left.
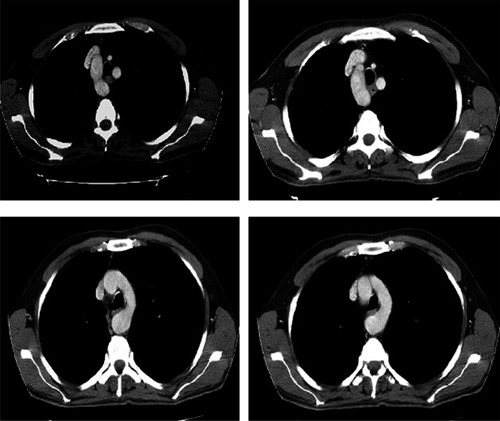
Figure 3 Computed tomography images of the patient’s trachea in relation to neighbouring tissues.
Discussion
The embryonic development of vascular ring has been explained in detail in literature.Citation3 There are six pairs of aortic arches that originate from the ventral aortic root in embryonic arch system. The first, second, and fifth primitive arches regress and form a double aortic arch. Normally, the left fourth arch regresses and forms the aortic arch. If the left fourth arch regresses and the right arch remains, this will result in a right-sided aortic arch.Citation3,Citation4 Classically, DAA has three types; right dominant aortic arch, left dominant aortic arch, and balanced-type aortic arch. In 75% of the cases, the right arch is dominant and in approximately 20% of the cases, the left arch is dominant. In 5% of the cases the dominance of both arches is equal.Citation5
Our case study patient had a balanced type of aortic arch. DAA can be accompanied by congenital cardiac defects, such as tetralogy of fallot and transposition of the great vessels.Citation6 Researchers recently reported that 20% of patients in their study with DAA had an intracardiac defect.Citation7 22q11 deletion was reported in 14% of the patients with normal intracardiac anatomy and DAA.Citation8 Symptoms are caused by compression of the trachea and the esophagus. At birth and in early infancy, symptoms such as respiratory distress, feeding difficulties, recurrent pneumonia, stridor, and dysphagia may occur as a result of tracheal and/or esophageal compression. But partial compression can lead to asymptomatic presentation, as shown in our patient. Adults with asymptomatic DAA are rare in literature. Presence of double cuts in right upper and left lower zones in tracheal air column is a significant finding. Barium esophagography may reveal esophageal compression but since the patient had no difficulty in swallowing we did not carry out this procedure. Chest X-ray may be normal and the diagnosis may be missed. Various imaging methods may be used to reveal DAA, such as magnetic resonance imaging (MRI), computed tomography scanning, and aortagraphy, in order to determine the best surgical approach for the patients who are surgical candidates.Citation9 We performed a three-dimensional CT for the purpose of gaining high quality three-dimensional images on a noninvasive basis. As far as we know this case is the first DAA case in which three dimensional CT scans. Echocardiography may be performed to reveal any intracardiac anomalies and may also be used for anatomical description of the vascular system. Bronchoscopy may be performed for the patients with compression of trachea to evaluate pulsalite tracheal compression. A surgical approach is the only choice for the patients with a symptomatic vascular ring anomaly. Surgical operations have a very high rate of success in infant patients with DAA.Citation2,Citation7 Some sporadic cases in which surgical treatments were performed in symptomatic adult patients have been reported.Citation2,Citation5,Citation9,Citation10 Surgical intervention with division of the minor arch is recommended for those adult patients who are symptomatic and can be approached via either left posterolateral thoracotomy or median sternotomy.
A therapeutic dilemma exists when asymptomatic patients undergo surgery for another cardiac condition. To date, there have been five patients with asymptomatic DAA diagnosed in their 6th and 7th decades of life.Citation2,Citation11–Citation14 Four of these patients were treated conservatively; only one patient underwent surgical intervention.Citation2 Division of the vascular ring at the time of coronary revascularization due to moderate esophageal compression was performed in this patient.Citation2 Because our patient was asymptomatic with no compression of trachea or esophagus we did not perform any surgical intervention; however, we informed the patient about potential complications of DAA and encouraged him the patient to make follow-up appointments.
Due to the sporadic nature of this anomaly, there are not enough data on either the long-term prognosis or the standard care of untreated DAA in adulthood. The long-term complications experienced by untreated DAA in patients undergoing surgery are unknown. Recent reports documenting nonoperative management have had good results.Citation12–Citation14
In summary, DAA (1) is a very rare congenital anomaly in adulthood, (2) may cause symptoms due to compression of the esophagus and trachea, (3) three dimensional CT for DAA detection is invaluable due to its noninvasive nature and high quality images, and (4) surgical intervention may be performed in symptomatic cases, otherwise nonoperative follow-up would be suitable.
Disclosure
The authors report no conflicts of interest in this work.
References
- GrossRESurgical relief for tracheal obstruction from a vascular ringN Engl J Med194523358659021003928
- KypsonAPAndersonCARodriguezEKoutlasTCDouble aortic arch in an adult undergoing coronary bypass surgery: a therapeutic dilemma?Eur Cardiothorac Surg200834920921
- EdwardsJAnomalies of derivatives of the aortic arch systemMed Clin North Am19483292594918877614
- EdwardsJEMalformation of the aortic arch system manifested as vascular ringsLab Invest19532567513036024
- RitaBSimoneSStefanoBPaoloMVascular ring due to double aortic arch: a rare cause of dysphagiaEur J Radiol2004522124
- EmmelMSchmidtBSchickendantzSDouble aortic arch in a patient with Fallot’s tetralogyCardiol Young200515525315831162
- KhalfanARebeccaGTaraKWilliamsWGCrindleBWManagement and outcomes of double aortic arch in 81 patientsPediatrics2006118e1336e134117000782
- McElhinneyDBClarkBJWeinbergPMAssociation of chromosome 22q11 deletion with isolated anomalies of aortic arch laterality and branchingJ Am Coll Cardiol2001372114211911419896
- ChiakiKShinTYoichiroMKojiOHidetoSIsaoYSuccessful surgical treatment for an adult case of double aortic archJpn J Thorac Cardiovasc Surg20055322322615875561
- StoicaSCLockowandtUCouldenRWardRBiltonDDunningJDouble aortic arch masquerading as asthma for thirty yearsRespiration200269929511844971
- IkenochiHTabelFItohNNozakiASilent double aortic arch found in an elderly manCirculation2006114e360e36116923763
- YilmazMTokMCengizMAsymptomatic balanced-type double aortic arch in an elderly patient: a case reportHeart Surg Forum200710e297e29817599878
- KajikawaYTakemotoSSuganamiYInoueMAsymptomatic double aortic archIntern Med20054435635715897653
- KindlerHBaggerJPTaitPCamiciPGA vascular ring without compression: double aortic arch presenting as a coincidental finding during cardiac catheterizationHeart20059177315894773