Abstract
Iatrogenic ureteric injuries in gynecologic surgery are quite common. The laparoscopic spectra of treatment gives a wide range of application. We present the case of a 40-year-old female who underwent total abdominal hysterectomy with bilateral salpingo-oopherectomy for dysfunctional uterine bleeding. Postoperatively, she had oliguria with raised creatinine and was found to have ureteric narrowing on magnetic resonance urogram. The patient was successfully managed by laparoscopic (Boari flap) ureteroneocystostomy.
Iatrogenic ureteric injuries in gynecologic surgery are quite common. The laparoscopic spectra of treatment gives a wide range of application. We present the case of a 40-year-old female who underwent total abdominal hysterectomy with bilateral salpingo-oopherectomy for dysfunctional uterine bleeding (DUB). Postoperatively, she had oliguria with raised creatinine and was found to have ureteric obstruction on magnetic resonance urogram. The patient was successfully managed by laparoscopic (Boari flap) ureteroneocystostomy. Saline was released on the right and left side urinary Boari flap.
Figure 1 Magnetic resonance urogram (MRU) showing bilateral ureteric obstruction.
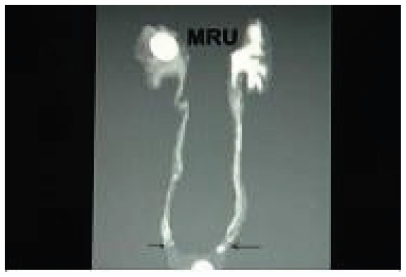
Figure 2 Creation of Boari flap.
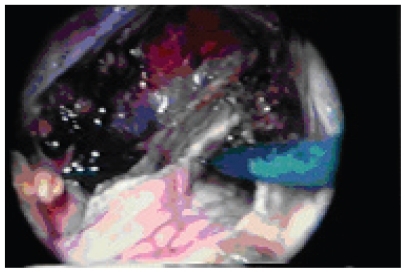
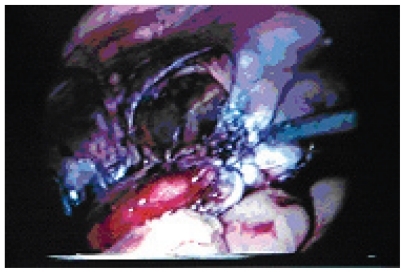
Figure 3 Tubularized Boari flap being anastomosed to the ureter.
Case report
A 40-year-old female patient underwent total abdominal hysterectomy with bilateral salphingo-oopherectomy for DUB with right-side broad ligament fibroid. Serum creatinine was 0.9 mg% prior to surgery. Following surgery, 500 ml of urine was drained from the bladder. No urine output was noted for the next 48 hrs. Abdominal ultrasonography revealed bilateral minimal hydronephroureterosis. Serum creatinine rose to 7 mg%. An attempted retrograde bilateral Dl stenting failed. Magnetic resonance (MR) urogram revealed an urinary column up to the lower ureters. The patient was preoperatively dialyzed and biochemical parameters came down to near normal. Patient was taken up for diagnostic laparoscopy under general anesthesia. The patient was placed in a supine position four days after abdominal hysterectomy. A 10 mm infraumbical port was placed along with two 5 mm ports, 4 cm below and lateral to the umbilicus. The lower ureters were identified at the level of crossing over iliac vessels. The ureters were traced downwards towards the bladder. The right lower ureter was found to be ligated with 2/0 vicryl. The ligature was cut and the ureter released. There was a 5 mm rent in the right ureter. A 6-Fr DJ stent (Bard, Karlsruhe, Germany) was introduced through cystoscopy and guided into the right renal pelvis under laparoscopic guidance. The rent in the ureter was sutured. The left lower ureter was found to be ligated and transected 5 cm above the vesicoureteric junction. The ligatures were cut and the proximal ureter was released. Approximation with the bladder was not possible in this situation. Boari flap was raised from the anterior surface of the bladder. The flap was converted into a tube and the lower end of the ureter was anastomosed to the end of the Boari flap tube. No attempt was made to create a submucosal tunnel antireflux technique. A 6-Fr DJ stent was placed and the bladder closed. Total operating time was 160 minutes. Urine output rose to 3400 cc in the first 24 hrs, serum creatinine came down to 0.9 mg% within 48 hrs, and ultrasound revealed no more hydrouretheronephrosis. No intra- or postoperative complications were noted. Postoperative paralytic ileus was noted for 96 hrs and conservatively managed.
Discussion
In gynecologic surgery, there is always the possibility that ureteral injuries will occur intraoperatively. Traditionally, these injuries were treated by laparotomy and ureteroneocystostomy. When the ureter is too short to reach the bladder without tension, bladder flap (Boari) technique is useful for ureteroneocystostomy.
The possible application of laparoscopic technique to different operations appears limitless. Attempts at laparoscopic ureteral reimplantation have involved the extravesical Lich-Gregoir technique with variable success I. CitationEhrlich and colleagues (1994) and CitationReddy and Evans (1994) independently showed the safety and feasibility of this technique clinically. In a recent series, CitationLakshamanan and Fung (2000) reported 71 laparoscopic extravesical reimplantations, including 23 unilateral and 24 bilateral, with no persistent reflux or obstruction postoperatively. CitationFergany and colleagues (2001) reported their experience with laparoscopic bladder flap (Boari) ureteroneocystostomy in the porcine model. Six female farm pigs were used to perform a laparoscopic bladder flap ureteroneocystostomy. No intra- or postoperative complications were noted. We have successfully used bladder flap (Boari) ureteroneocystostomy to bridge the gap in lower ureter and maintain the continuity of the draining system. Laparoscopic ureteroneocystostomy using the bladder flap technique can be performed successfully. Robotics may make this procedure easier with better vision and dexterity during suturing.
References
- EhrlichRMGershmanAFuchsG1994Laparoscopic vesicoureteroplasty children: initial case reportsUrology43255618116127
- FerganyAFSameeAAKaoukJH2001Laparoscopic porcine bladder flap (Boari) ureteric reimplantationJ Urol1661920311586261
- LakshamananYFungLC2000Laparoscopic extravesicular ureteral reimplantation for vesicoureteral reflux: recent technical advancesJ Endourol145899311030542
- ReddyPKEvansRM1994Laparoscopic ureteroneocystostomyJ Urol152205797966672