Abstract
The development of a dynamic leadership coalition between practitioners and researchers/scientists – which is known in Canada as integrated knowledge translation (KT) – can play a major role in bridging the know-do gap in the health care and public health sectors. In public health, and especially in globally oriented public health, integrated KT is a dynamic, interactive (collaborative), and nonlinear phenomenon that goes beyond a reductionist vision of knowledge translation, to attain inter-, multi-, and even transdisciplinary status. Intimately embedded in its socioenvironmental context and closely connected with the complex interventions of multiple actors, the nonlinear process of integrated KT is based on a double principle: (1) the principle of transcendence of frontiers (sectorial, disciplinary, geographic, cultural, and cognitive), and (2) the principle of integration of knowledge beyond these frontiers. However, even though many authors agree on the overriding importance of integrated KT, there is as yet little understanding of the causal framework of integrated KT. Here, one can ask two general questions. Firstly, what “determines” integrated KT? Secondly, even if one wanted to apply a “transfrontier knowledge translation” vision, how should one go about doing so? For example, what would be the nature and qualities of a representative research program that applied a “transfrontier collaboration” approach? This paper focuses on the determinants of integrated KT within the burgeoning field of knowledge translation research (KT research). The paper is based on the results of a concurrent mixed method design which dealt with the complexity of building and sustaining effective coalitions and partnerships in the health care and public health sectors. The aims of this paper are: (1) to present an “integrated KT” conceptual framework which is global-context-sensitive, and (2) to promote the incorporation of a new “transfrontier knowledge translation” approach/vision designed primary for globally oriented public health researchers and health scientists.
Introduction
In today’s globalized learning economy,Citation1,Citation2 the ability to integrate, share, and disseminate knowledge across functional silos in health care organizations constitutes a major challenge, referred to as a knowledge-sharing (KS) challenge in the knowledge management parlanceCitation3–Citation8 or as a knowledge translation (KT) challenge by public health practitioners and scientists.Citation9–Citation14 In the context of contemporary globalization, the difficulty of this dual KS–KT health-related challenge is augmented by the need for social sustainability and eco–socio–efficiency.Citation15–Citation17
Improvements in the intertwined KS–KT aspect of the public health practice and health care are based on the ability to generate and integrate new knowledge into clinical/managerial practice while maintaining sound clinical/managerial processes. However, the acquisition and integration of knowledge is mostly “bit by bit”, fragmented, and unbalanced. Subsequently, and along with many authors,Citation18–Citation25 I believe that an active collaboration or coalition for sustainable KS–KT practices is the cornerstone to establishing effective knowledge-based health care institutions.Citation16 The development of a dynamic leadership coalition between practitioners and researchers/scientists – which is known in Canada as integrated KT – can play a major role in bridging the know-do gap in the health care and public health sectors. The term “integrated KT” refers to both a process and its result. In public health, and especially in globally oriented public health, integrated KT is a dynamic (nonstatic), interactive (collaborative), and nonlinear phenomenon that goes beyond a reductionist vision of knowledge translation (sometimes seen in clinical epidemiology), to attain inter-, multi-, and even transdisciplinary status. The process of integrated KT is based upon: (i) the collaboration of individual and institutional actors and the integration of their respective knowledge bases, (ii) the development of a sustained synergy among knowledge users and knowledge producers, and (iii) the emancipation of postpositivist biomedical paradigms, removal of interdisciplinary barriers, and the development of sectors favoring a collective approach to shared problems and questions concerning health.
Intimately embedded in its socioenvironmental context and closely connected with the complex actions and interventions of multiple actors, the nonlinear process of integrated KT is based on a double principle: (1) the principle of transcendence of frontiers (sectorial, disciplinary, geographic, cultural, and cognitive), and (2) the principle of integration of knowledge beyond these frontiers. Integrated KT thus becomes, according to Lapaige et al a double-process of transfrontier integration that permits: (i) optimization of evidence-based practice, evidence-based health care management, and evidence-informed policy, (ii) the development of ecolearning health care institutions, and (iii) the promotion of evidence-based, equitable, and sustainable public health in response to collective and individual vulnerabilities in a context of globalization.Citation26 However, even though many authorsCitation18–Citation26 agree on the overriding importance of integrated KT – the development of sustained partnerships between producers and consumers of knowledge – there is as yet little understanding of the causal framework of integrated KT. Here, one can ask two general questions. Firstly, what “determines” integrated KT? In other words, what are the success factors of coalitions and partnerships in KS and KT that actually (i) improved patient care, and (ii) developed ecolearning health care institutions? Secondly, even if one wanted to apply a “transfrontier knowledge translation” vision, how should one go about doing so? For example, what would be the nature and qualities of a representative research program that applied a “transfrontier collaboration” approach?
This paper focuses on the determinants of integrated KT within the burgeoning field of knowledge translation research. The paper is based on the results of a concurrent mixed method design which dealt with the complexity of building and sustaining effective coalitions and partnerships in the health care and public health sectors. The aims of this paper are: (1) to present an “integrated KT” conceptual framework which is global-context-sensitive, and subsequently (2) to promote the incorporation of a new “transfrontier knowledge translation” approach in health care and (global) public health research.
The paper is divided into four parts: (1) terminological clarifications, and particularly the similarities and differences between KT, KT research, and integrated KT, (2) presentation of the QUAN-qual mixed model design used in my KT research study; based on preliminary results of this study, (3) a conceptual framework of integrated KT, which highlights the growing need for a global-context-sensitive vision in KT and evidence-based decision-making in health care institutions; and (4) in conclusion, presentation of an example of a currently active Canadian research program which has embraced an innovative vision in KT research. This new globally oriented KT approach transcends six types of borders in bridging the know-do gap in health care and public health: it has been called “transfrontier KT approach”.
Knowledge translation, knowledge translation research, and integrated knowledge translation: Terminologies, similarities, and differences
In today’s information age, the importance of health-related knowledge as a key source of competitive advantage is well established worldwide, as suggested by the increasing literature focusing on health care knowledge creation (generation, production), (re)use, application, exchange, dissemination, and transfer, and the rapid growth of the KT research field in Canada.Citation1,Citation6–Citation8,Citation10–Citation15,Citation17,Citation27–Citation50
Over recent years, there has been a major shift in the world economy from an industrial economy to a knowledge economy.Citation2,Citation51,Citation52 Canada, like other Western societies, has found itself in a context characterized by increasing globalization of production and exchange of goods, services, and capital, as this “new economy” spreads. The importance of knowledge as a source of sustainable competitive advantage has been discussed by a myriad of authors, and managing knowledge has become a major concern for many organizations, including health care institutions.Citation4,Citation5
At the dawn of the 21st Century, knowledge is a crucial resource in the provision of health care, guiding improvements to clinical/managerial decision-making, patient care, health outcomes, workforce quality, and organizational behavior and structure.
In this paper, evidence-based decision-making is discussed not only at the micro level of individuals (clinicians, public health practitioners), but also at the meso level of groups (teamwork) and sectors (health sector, public health field). According to Shortell et al the notions of KT (individual level) and KS (meso level) have been intertwined.Citation46 This paper considers sustainable KS–KT practices – artifact-mediated, experience-mediated, and resource-mediated KS–KT practices () – and the determining forces of their success in order to (i) develop ecolearning health care institutions, and (ii) improve patient care, population health, and the working lives of both (public) health practitioners and scientists at a time of changing roles and expectations.
Table 1 A note about terminology
While there is an overlap between these two notions, KT and KS are conceptually distinct (). They are nevertheless complementary. KT is emerging worldwide as a paradigm to learn and act toward closing the know–do gap in the domain of health care and the field of public health. In this paper, I am focusing on integrated knowledge translation with public health practitioners and health care researchers () at the micro (clinical level) and meso (managerial/organizational level) levels. The term “integrated KT” describes a different way of doing research in which researchers and research users work together to shape the research process, starting with collaboration on setting the research questions, deciding the methodology, being involved in data collection and methodological development, interpreting the findings, and helping to disseminate the research results ().Citation53 This approach, described in terms such as practice-oriented translational research (T2 research), collaborative research, action-oriented research, and co-production of knowledge, should produce findings which are more likely be relevant to, and for, end users.Citation54 Furthermore, in this paper, I consider KS, which is essentially used in the knowledge management parlanceCitation3,Citation4 and better tailored for a meso level, as a part of integrated KT ().
Figure 1 Integrated knowledge translation in a changing global context.
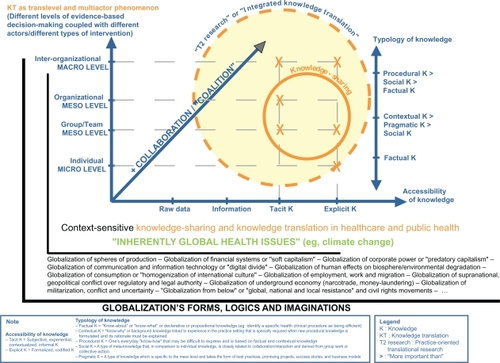
Table 2 The similarities and differences between KT, KT research, and integrated KT
In this paper, the basic premise is that KT is a multiactor and translevel phenomenon involving different levels of evidence-based decision-making and, correspondingly, different types of knowledge (). Health care knowledge is a social construct and the processes of KS, KT, and integrated KT (acquiring knowledge; [re]using knowledge; developing new knowledge) are social processes and entail organizational changes. Linking integrated KT with organizational learning can usefully interconnect different levels within a health care organization: individual, group/team/community, and organization (). This link also constitutes a fruitful way of approaching the complexity of managing KS/KT/integrated KT among health care professionals/public health practitioners, and mapping out future directions toward a “transfrontier KT approach” that institutionalized health care KS and KT might take.
“Integrated knowledge translation” in a changing global context: A concurrent mixed-method research design
Faced with the problem of an ever-mounting growth of information/knowledge, or in some cases “paradoxical information/knowledge”, both collective actors (health care institutions) and individual actors (public health practitioners and health scientists) need solutions. At the same time as the information/knowledge overload is increasing, health costs are expanding. Consequently actors at different levels – health care institutions workers, professionals, and researchers – are faced with the unattractive task of discovering approaches that are “better”, “faster”, and “cheaper”. With these imperatives in mind, new concepts, paradigms, or guiding principles reflective of the contemporary forces driving global change have become prominent in the past decade:
Evidence-based medicine and the drive for evidence-based approaches
The drive for a major leadership shift (from a traditionally top-down leadership to a transformational or coalition leadership) in health care
The drive for new models of KS in the knowledge management field, and the emergence of the KT paradigm in health care and public health
The drive for global collaboration and a renewed definition of globalization in public health
The drive for acknowledgement of the social nature of many determining factors, and consequently, the drive for new theories, perspectives, and/or identities in public health “[capturing] the idea that the physiological end-pathways leading to an individual’s ill health are inextricably linked to the social setting” (p. 14).Citation53
The drive for transdisciplinary teams and participatory research (integrated KT) in the health care and public health sectors.
Today’s health care organizations increasingly recognize the need to support the practice of KS and KT among their “employees”. As a consequence, researchers and professionals in clinical, managerial, and policy decision-making environments are collaboratively searching, testing, and using proactive interventions to facilitate KS and the application of knowledge. However, the success of active and efficient collaborations depends on a myriad of factors.
My two-part research study focused on active collaboration for sustainable KS–KT practices in globally oriented (public) health research. It drew on a nonlinear perspective that conceives KS and KT as accomplishing changes not only in technical, but also, and primarily, in cognitive, social and, organizational contexts.
This study was at the crossroads of three specific perspectives of research: (i) KT research,Citation53,Citation56 (ii) critical population health research,Citation57–Citation59 and (iii) the new field of equity in health.Citation60 My research goal was to elaborate an integrated KT conceptual framework designed for public health practitioners and researchers. The methodological design was a concurrentFootnotea mixed method design (QUAN + qual)Footnoteb: (i) the QUAN phase of the QUAN-qual design was a systematic review method,Citation64 and (ii) the qual phase of the QUAN-qual design was a Soft Systems Methodology.Citation65–Citation67 The qualitative strand/phase of this methodological approach enables this two-part study to be look upon as an integrated KT, responding to what is been referred as “Mode II of knowledge production”Citation68,Citation69 ( and ).
The qual strand was under the umbrella of a larger research program called “PROACTIVE” (Participatory and Evaluative Research Program to Optimize Workplace Management: Application of Knowledge, Transfer of Expertise, Innovative Interventions, Training Transformational Leaders).Footnotec The participants were health care managers (as “integrated KT users”; n = 199 [from 34 management teams originating from three Canadian provinces: Quebec, Ontario, and New Brunswick]) and academic partners (as knowledge producers [n = 13]).Citation70 Data collection included different Web-techniques (Web-based journal, Web-based interviews, peer-review Soft Systems Model validation through Web-conferencing), and data analysis was conducted by grounded theory.
The QUAN strand’s main objective was to identity the key elements of the dynamic process of integrated KT within health care institutions. The following research questions were considered in this systematic review: (1) What are: (i) the different definitions of “integrated KT” within health care institutions, (ii) the different types of knowledge and forms of evidence used by health care managers/public health practitioners, (iii) the different types of managerial KS, and/or (iv) the determinants of this KT?, (2) What are the integrated KT conceptual frameworks discussed in the literature?, and (3) What are the key indicators used to assess the KT evolution within health care institutions?
Two search chains (English and French keywords search chains) were used as follows:
– (“evidence-based health care management” OR “evidence-based healthcare management” OR “evidence-based health management”) OR ((“knowledge manage*” OR “evidence-based management” OR evidence OR “knowledge transfer” OR “knowledge translation” OR “knowledge sharing” OR “knowledge utilization” OR “research utilization” OR “knowledge application”) AND (health OR healthcare OR “health care” OR hospital* OR “health W/2 organization*” OR “health W/2 administrat*” OR “public health W/2 institute*”))
– (((gestion OR administrat* OR cadre* OR organis* OR institut*) W/3 (soins OR service* OR sante)) AND (preuve* OR “donnee* probante*” OR “savoir* probant*” OR “donnee* factuelle*” OR” fait*” OR evidence*)) OR ((gestion OR manage* OR transfert OR utilization OR application) W/3 (savoir* OR connaissance* OR resultat*) AND (soins OR service* OR sante))
The inclusion criteria were: (1) English and French sources, (2) published and unpublished documents or reports, (3) manual searching used as well as electronic databases, and (4) publication period: from 1990 to 2009. The exclusion criteria were: (1) master or PhD thesis, (2) editorials, and (3) success stories. The databases consulted were: ISI Web of Knowledge, EBSCO, Cochrane Library, Current Contents: All EBM Reviews: MEDLINE/Pubmed, EMBASE, CABI, CINHAL, ASSIA, AHA Hospital and Health Administration Index, and BDSP. The references were entered into Reference Manager v.11.0 (Thomson ResearchSoft, New York, NY) and after removal of duplicates, a total of 11,207 references remained. These were further reduced through review of abstracts. Results reported here are based on preliminary analysis of 308 articles.
The development of my conceptual framework was based on the secondary results of the qual strand and the preliminary results of the QUAN strand (systematic review). At the end of each strand/phase of the design, qualitative inferences (predominantly inductive inferences) were made. These inferences were combined/contracted to achieve a fuller picture of the integrated KT process.Citation71 Strategies for integrating these inferences and the role of each (eg, exploratory, triangulation) were more crucial than the priority/dominance of one approach over another (QUAN-qual).Citation72,Citation73
What determines “integrated knowledge translation”? A global-context-sensitive conceptual framework
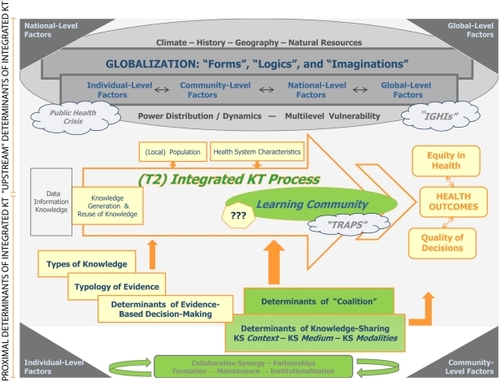
Integrated KT is influenced by many factors/determinants and groups of factors/determinants that are interrelated at many levels, but can be divided into two supra-categories: (i) “upstream” determinants, and (ii) proximal determinants. Each of these supra-categories can be subdivided in the following way:
“Upstream” determinants of integrated KT (context of contemporary globalization)
Ia. Globalization: forms, logics, and imaginations
Ib. Multilevel factors of life-worlds
Ic. Multilevel vulnerability and “inherently global health issues”
II. Proximal determinants of integrated KT
IIa. Health systems characteristics
IIb. Determinants of evidence-based decision-making
IIb-1. Types of knowledge
IIb-2. Typologies of evidence
IIb-3. Determinants of coalition
IIb-4. Determinants of knowledge-sharing
IIc. Traps and questions.
The usefulness of this framework () is firstly to show the importance of multilevel relationships between: (i) contemporary globalization, (ii) the evidence-based decision-making movement, and (iii) the development of effective and sustainable collaboration between knowledge users and producers.Citation16 Secondly, illustrates that: (i) integrated KT is a nonlinear phenomenon with multiple and complexly intertwined determinants, (ii) integrated KT is a global-context-sensitive phenomenon which is influenced by multilevel factors of life-world and vulnerability (global-level factors, national-level factors, community-level factors, individual-level factors).
Figure 2 Integrated knowledge translation conceptual framework.
I. “Upstream” determinants of integrated KT (context of contemporary globalization)
Although globalization () can be described as a socio-historical process evolving along with human societies, it is necessary to distinguish “globalization” from other terms such as “internationalization” (political internationalization is the growth of cross-border economic and political activity), “liberalization” (economic liberalization refers to “free-market” strategies), “westernization” (the global spread of companies such as McDonald’s), and “universalization” (global convergence around cultural and institutional forms), terms that are often used interchangeably. The work of Scholte is helpful in this respect.Citation74 This author reserves the term “globalization” to describe social interactions that not only cross national boundaries, but also transcend them, and he sees the emergence of transplanetary relations and the rise of supra-territoriality as genuinely novel features of globalization.Citation74 Satellite communications, the Internet, transplanetary TV, intercontinental production chains, anthropogenic ecological changes (eg, global warming), illicit drug trafficking, transworld migrants, and economic remittances are examples of globalization in this strict sense. It is very important to be aware of how the term globalization is defined, for a looser definition suggests that at least some aspects of what people call globalization are not novel to the late 20th century. A strict definition of globalization as the transcendence of territorial boundaries is distinctive of the transition facing human societies worldwide in recent decades.
A second important question is why globalization is occurring. What are the “forms” and “logics” of globalization? And what are some globalization-related conceptual schemes or “imaginations”?
Ia. Globalization: Forms, logics and imaginations
The forms ( and ) it takes can be differentiated as follows:
Globalization of capital or of the finance sector (globalization of financial systems: “soft capitalism”)
Globalization of markets and globalization of spheres of production, commerce, and logistical systems
Globalization of technology, R&D, and knowledge
Globalization of lifestyles, consumerism, and culture (or globalization of consumption, “homogenization” of international culture, cultural challenges)
Globalization of standards (this particular form has major stakes in global governance, which for its part constitutes an integral part of globalization) and globalization as a worldwide policy instrument (globalization of supranational and geopolitical conflict over regulatory and legal authority)
Globalization of perceptions of human conditions or of a “global conscience”, “globalization from below” (global, national, and local resistance, and human rights movements)
Globalization of communication and information technology (“digital divide”) and communication-media globalization
Globalization of corporate power or “predatory globalization” (mega-mergers, oligopolies)
Globalization of human effects on biosphere, and of environmental degradation
Globalization of militarization, conflict, and “fear and risk” (post-cold War continuity, post-9/11 tensions)
Globalization of employment, work, and migration.
Furthermore, globalization subscribes to six different “logics”,Citation16 that can be defined as abstract and schematic orders of reasoning that allows an understanding of the complexity of reality. First, there are market logics and productive logics, which are closely related and make up the core of the new globalizing world. Productive logic is the root of the organizational changes in globalization on which production, re-engineering, and “total quality” are based. Market logic extols the marketability of everything and anything. Secondly, at the very core of the capitalist system is velocicratic logic. In the context of globalization, new forms of expression of the human connection to time are effectively emerging: these are urgency, immediacy, instantaneousness, and speed, with acceleration being the common denominator that unites the other forms. The arrival of urgency and instantaneousness in economic life falls right in line with the emergence of a new global space-time. Velocicratic logic therefore joins another type of logic – cyber logic – which, for its part, is related to the ICT revolution. Technoscientific logic, which represents the alliance between science and technology, comes third. Technoscientific logic is inseparable from the performance culture which, when allied with the cult of speed and subjected to the law of market, gives it real meaning. Coming fourth is epidemic logic, which relates to the breakdown of boundaries. Whether we are dealing with a computer virus, the disappearance of borders, the deregulation of the foreign exchange market, a rise in political extremism, or the mad cow crisis, a similar “epidemic” logic seems to guide these apparently social facts.
Moreover, the new globalizing world is shown through various conceptual schemes, or “imaginations”:
The comprehensivist imagination, as in “similar throughout the world”
The “worldwide everyday life” imagination (“global happenings”, catastrophes, etc)
The “collective cohabitation” imagination
The “everything is for sale and everything can be bought” imagination, as in freedom of choice
The discursive imagination (that is, words specific to our times: governance, accountability, effectiveness, quality improvement, and assessment).
These different forms, logics, and imaginations of contemporary globalization influence multiple “levels” of determination of variegated life-worlds. Generally speaking, they cause a profound crisis in public health. More specifically, they can be tied to the development of integrated KT as well as the development of a multilevel vulnerability and the emergence of “inherently global health issues” (IGHIs).
Ib. Multilevel factors of life-worlds
– Global-level factors include: global trade, global public goods, emerging global governance, ICT, migration, income distribution.
– National-level factors refer to: infrastructural resources, population density, employment, income growth, political institutions, policies and programs which enhance capabilities and build social capital (eg, education, income transfers, public investments in infrastructure, disease prevention measures), social inclusion, and social support networks.
– Community-level factors correspond to: resource allocation, population heterogeneity, social environment, and physical environment (eg, clean water and air, safe and warm housing, safe working conditions, adequate fuel supplies, fertile soil).
– Individual-level factors include: biology and genetics endowment, healthy child development, gender, personal health practices, and coping skills.
Ic. Multilevel vulnerability and “inherently global health issues”
A new category of vulnerability has appeared in the context of contemporary globalization that can be termed a “globo-agentive” vulnerability, referring to the impact of globalization upon agents at various levels of their life-world. This multilevel vulnerability is itself in interaction with the appearance of IGHIs and the public health crisis (see the upper part of ).
– Globo-agentive vulnerability is manifested in: income disparities, educational disparities, geospatial disparities (eg, regional inequalities, economic segregation), gender disparities and discrimination, and ethnic disparities.
– Globo-agentive vulnerability results from factors such as: living conditions (eg, housing, neighborhood characteristics), employment and working conditions (economic insecurity, occupational exposures), food quality and security, water quality, and air quality (eg, urban, agricultural and industrial pollution exposures, access to safe water, sanitation).
– Globo-agentive vulnerability is linked to the emergence of IGHIs. Labonte et al proposed the term “inherently global health issues” to describe health-determining phenomena that transcend national borders and political jurisdictions and urge greater research and policy attention to the linkages between these issues.Citation75 IGHIs are related to the crisis of public health; they can be structured around three themes:Citation76
The first theme concerns collective resources and comprises climate change, the disappearance of ecosystems, the diminution of marine resources, deforestation, water shortage, and maritime pollution.
The second theme involves action by individual citizens, with respect to the intensification of the struggle against poverty, the struggle against terrorism, education for every person, infectious disease, the digital divide, and the prevention and management of natural catastrophes.
The third theme relates to burgeoning global governance. With respect to codes, norms, and regulations, it will be necessary to: (i) re-invent income tax for the 21st century, (ii) reflect on the establishment of rules concerning bio-technology, a worldwide financial structure, commerce, investment, and competition, (iii) reflect on laws concerning intellectual property, and (iv) reflect on the establishment of rules of commerce, as well as international rules concerning work and migration.
II. Proximal determinants of integrated knowledge translation
The components of an integrated KT process include both health care characteristics and the determinants of evidence-based decision making which can be characterized as (i) types of knowledge, (ii) evidence typology, (iii) coalition determinants, and (iv) KS determinants (see the lower part of ). Collectively, in a nonlinear fashion, all of these factors decisively impact the integrated KT process, which in turn influences health outcomes, decision quality, and health equity. Finally, in the case of an integrated KT process involving the development of a learning community, there are traps to be avoided and questions that must be asked to assure the success of the integrated KT.
IIa. Health system characteristics
These characteristics include: the availability of care, the affordability of care (eg, effects of cost recovery, user charges), and the availability of care (eg, adequate health human resources, rural/urban equity).
IIb. Determinants of evidence-based decision-making
IIb-1. Types of knowledge
Five types of knowledge can be distinguished in the health and public health sectors: (i) factual knowledge (propositional knowledge or “Know-About”), (ii) contextual knowledge (“Know-Why”), (iii) procedural knowledge (“Know-How”), (iv) social knowledge, and (v) pragmatic knowledge.Citation77
Types of knowledge can further be distinguished with respect to relative accessibility: (i) easily-accessible explicit knowledge (formalized, codified knowledge), (ii) less-accessible tacit knowledge (subjective, experiential, contextualized, informal knowledge), and (iii) implicit knowledge considered as having “intermediate” accessibility.
IIb-2. Typologies of evidence
With respect to the various types of evidence, the following three aspects should be considered:
The sources of evidence: published literature and grey literature; “absolute scientific data”, “contextual scientific data”, and “informal data”
The nature of evidence: qualitative research, survey, case-control studies, cohort studies, randomized control trials, quasiexperimental studies, nonexperimental interventions, and systematic reviews
The characteristics of scientific evidence: availability, accessibility, validity, timing, and communicability.
IIb-3. Determinants of coalition
Within an integrated KT process, the determinants of coalition have to be taken into account. Empowering people to develop a collective vision and creating systems to capture and share learning (in case of the development of a learning community) is not an easy undertaking. The determinants of coalition are: the structural and functional characteristics of coalition such as formalization, communication, conflict resolution, as well as the commitment to collaborative efforts, the perceived benefits, and the institutionalization of the community.
IIb-4. Determinants of knowledge-sharing
The determinants of KS include: (i) the KS context, (ii) the KS medium, and (iii) the KS modalities.
KS takes place within a context which epitomizes: (i) the issue or the subject of the shared knowledge, (ii) the motivation for KS, (iii) the temporal relevance of the shared knowledge, (iv) the orientation of the decision-makers engaged in the KS exercise (eg, terminology used, brevity and formality of knowledge, language constructs, expected outcomes, trust in sources), and (v) the decision-makers’ needs, interests, operational capacity, and degree of trust towards the knowledge.
KS is practiced via a medium. The sophistication of this medium may range from face-to-face environments (eg, person-person conversations, speaker-audience interactions) to Internet-based mediums (eg, online discussion forum, Web-CT, peer-to-peer networks).
KS modalities are determined by the nature of the knowledge to be shared (explicit versus implicit, factual versus contextual, pragmatic versus social) as well as the character of the relevant evidence (availability, accessibility, validity, timing, and communicability). The KS modalities can be characterized in the following ways: (i) asynchronous versus synchronous versus multisynchronous, (ii) anonymous versus disclosed identity of the decision-makers, (iii) individual-based interactions versus group interactions, (iv) push versus pull versus deliberative mode of knowledge delivery, (v) open participation versus members-only participation, (vi) supporting-dynamic versus static knowledge content, and (vii) short-term versus long-term relationships between decision-makers.
IIc. Traps and questions
In the case of an integrated KT associated with the constitution of a learning community, the integrated KT process can be analyzed by answering to the following questions:
Why is knowledge shared?
When is knowledge shared?
Where is knowledge shared?
Who shares knowledge?
What type of knowledge is shared?
How is knowledge shared? (these questions are represented with question marks in the center of ).
One must also be watchful for the various “traps” that can complicate the successful development of a learning community’s integrated KT:
The “individual learning trap” (this trap refers to the danger of treating integrated KT as a learning process for the individual [at the micro level] while disregarding its contribution to the health care institution/health sector [at the meso/macro level])
The “ICT trap” (this trap revolves around placing too much faith in information and communication technologies’ ability to improve integrated KT)
The “management trap” (this trap relates to the tendency to approach the need for supporting integrated KT with too much empathy for the management perspective)
The “inequity trap” (this trap related to the tendency to forget the context of contemporary globalization and IGHIs).
Conclusion: The need for a transfrontier approach in knowledge translation research
Success-determining factors of an integrated KT with respect to a given IGHI are numerous, varied, and interrelated in complex ways: their effective application is no easy task. In Quebec, a recently-developed approach that takes into account a maximum number of these factors is being applied to the specific IGHI of climate change. The KT research chair, Climat, santé, écoapprentissages, provides an illustration of an equitable, sustainable, and transborder vision in KT research.Citation78
In the face of the planetary challenge of global warming, all of us must act, as citizens and public health workers, if we hope to see humanity develop in a harmonious, just, and environmentally-friendly way. As public health professionals, we can and must do more than simply echo a general appeal for global ecocitizenship: we can promote, develop, and transfer ecoknowledge conducive to healthy climatic conditions: (1) in prioritizing research on the applications of ecoknowledge (KT research), and (2) by orienting this research so that it focuses on the adaptation of public health to climate change, and on the attenuation of climate change (mitigation).
The research program of this Chair respects the global priorities mentioned in Article 6 of the Climate Convention (United Nations Framework Convention on Climate Change), and the Plan d’action 2006–2012 sur les changements climatiques – Volet santé of the Ministry of Health and Social Services of Quebec.Citation79,Citation80 The recent accumulation of research results flowing from studies on climate change poses the challenge of applying these results to achieve attenuation of climate change as well as adapting public health to the impacts of those climate changes.
The Chair promotes values of social justice, enduring change, and shared responsibility, and the explicit intention is to extend application of research results beyond several frontiers (sectorial, disciplinary, geographic, cognitive, and cultural), and is thus in many senses of the term “transfrontier”. The Chair is also committed to an overarching vision of: (1) an engaged citizenry with leadership shared among individual and organizational members, and (2) a transfrontier application of knowledge that seeks to reinforce the adaptive capacities of health systems, enabling them to promote climatic health that is just, enduring, “transfrontier”, and that entails shared responsibility. The “transfrontier” aspect of this visionCitation78 refers to an application of knowledge that would ideally be:
Trans-sectorial, in that the program seeks to transcend hermetic sectorial compartmentalization of knowledge among key actors for adaptation
Transdisciplinary, in that the program seeks to break down disciplinary barriers (climate sciences, public health sciences, social sciences) and exclusionary schools of thought between key actors
Transnational (and transinstitutional), in that the program seeks to transcend spatial boundaries between agents as well as spatiotemporal boundaries between their knowledge bases
Transcognitive, in that the program seeks to transcend the cognitive forms that characterize various disciplines, that may facilitate work and communication within a discipline but render it less accessible to other specialists, as well as to transcend the various supports, medias, and practices related to these disciplines
Transknowledge level, in that the program seeks to integrate the various levels of knowledge (micro, meso, macro)
Transcultural, in that the program seeks to transcend cultural and ethnic boundaries, by promoting local cultures of contributing agents (eg, traditional knowledge and practices), mobilizing and integrating them without excluding their particularities.
In conclusion, this transfrontier KT vision is aligned with Wallace’s definition of globalization as “[…] an awareness of how “what affects one affects all”, or a consciousness of our fundamental interdependence as a global community, as well as the resulting process of learning to work collaboratively and share and disperse resources within our global community to ensure social justice, equity, the protection of the human rights, and the sustainability of the planet” (p. 19).Citation81
Such a consciousness and KT approach can also guide the weeding out of the destructive forms, logics, and imaginations of contemporary globalization. Transfrontier collaboration is needed to fully actualize that which is constructive. The drive for globalization, as newly defined, and transfrontier collaboration research are the pillars of the newly emerging KT research field.
Acknowledgements
Funding has been provided by the Canadian Health Services Research Foundation (CHSRF) and the Canadian Institutes of Health Research (CIHR) (# PDA-1833-05). The views expressed in this paper are those of the author and do not necessarily reflect the position or policy of the Canadian Health Services Research Foundation, the Canadian Institutes of Health Research, or the Laval University. This paper was presented during the 137th APHA (American Public Health Association) Annual Meeting which took place in Philadelphia, PA from November 7–11, 2009. It received positive feedback from Dr. George Washington, the facilitator of Session 4036.0 “Translation of health administration theory and research to health administration practice”. The author equally thanks Dr. Nancy Borkowski, Director of the Chapman Graduate School of Business, from Florida International University, as well as Dr. Lea Ayers LaFave of the New Hampshire Public Health Institute.
When the study was conceptualized and designed, Veronique Lapaige was a CHSRF/CIHR knowledge translation research fellow in the PROACTIVE program (Participatory and Evaluative Research Program to Optimize Workplace Management: Application of Knowledge, Transfer of Expertise, Innovative Intervention, Training Transformational Leaders), a research program directed by Chantal Viens and Sylvie Hains. At the time of the study, the author was mentored by Dr. Chantal Viens (Laval University), Dr. Michel O’Neill (Laval University), Dr. Jean Rochon (Quebec National Institute of Public Health), and Sylvie Hains (Quebec Ministry of Health and Social Services). The author thanks all of them for their thoughtful feedback on the conception of this study.”
The author extends her sincere thanks to Christian Dagenais (Montreal University) and his KT research team (“Valorisation et transfert de connaissances” Team) as well as to Marie Désilet and the Louis-H Lafontaine Hospital’s librarians (Montreal) for their unconditional support during the systematic review.
Her thanks also go to the reviewers for their insights, helpful comments and precious suggestions.
Disclosure
The author reports no conflicts of interest in this work.
Notes
a A concurrent mixed method design is a multistrand design in which both qualitative and quantitative data are collected and analyzed to answer a single type of research question (either qualitative or quantitative). The final inferences are based on both data analysis results. The two types of data are collected independently at the same time or with a time lag.Citation61
b Morse, writing in the applied field of nursing, authored an important paper on approaches to quantitative-qualitative methodological triangulation in which she presented a basic terminology and notational system.Citation62,Citation63 Her notational system is the standard currently used in the mixed methods research area. Components of this system include the following: (i) use of the abbreviations QUAN for quantitative and QUAL for qualitative, (ii) use of the plus sign (+) to indicate that data are collected simultaneously (eg, QUAN + qual), and (iii) use of uppercase to denote more priority given to that orientation (eg, QUAN).Citation62,Citation63
c “PROACTIVE” was a sequential program of three research projects focusing on the reorganization of care, services, and work in Canada. This program was led by Chantal Viens and Sylvie Hains from Laval University and Ministry of Health and Social Services, respectively.Citation70 The PROACTIVE program’s main objectives were to support Canadian health care institutions’ managers in carrying out evidence-based decisions on the reorganization of care, services, and work, to promote transformational leadership, and to mentor these managers and their partners.Citation70 Only the secondary results of the PROACTIVE program were considered here.
References
- ForayDOptimizing the use of knowledgeKahinBForayDAdvancing Knowledge and the Knowledge EconomyBoston, MAMIT Press2006918
- DolfsmaWKnowledge Economies: Organization, Location and InnovationNew York, NYRoutledge2008
- AbidiSSRHealthcare knowledge sharing: purpose, practices, and prospectsBaliRKDwivediANHealthcare Knowledge Management. Issues, Advances, and SuccessesNew York, NYSpringer20076786
- BaliRKDwivediANHealthcare Knowledge Management. Issues, Advances, and SuccessesNew YorkSpringer2007
- WickramasingheNGuptaJNDSharmaSCreating Knowledge-Based Healthcare OrganizationsLondon and Hershey, PAIdea Group Publishing2005
- CowellRKnowledge management essential, not optionalNurs Manage20061361013
- ChunharasSAn interactive integrative approach to translating knowledge and building a “learning organization” in health services managementBull World Health Organ200684865265716917653
- WalsheKRundallTGEvidence-based management: from theory to practice in health careMilbank Q200179342945711565163
- GrayMEvidence-based Healthcare and Public Health. How to make decisions about health services and public health3rd edEdinburgh, UKChurchill Livingstone Elsevier2009
- ArmstrongRWatersERobertsHSandyOPopayJThe role and theoretical evolution of knowledge translation and exchange in public healthJ Public Health2006284384389
- DavisDContinuing education, guideline implementation, and the emerging transdisciplinary field of knowledge translationJ Contin Educ Health Prof200626151216557510
- GrahamIDTetroeJWhither knowledge translation: an international research agenda [comment]Nurs Res2007564 SupplS86S8817625480
- HedgesJRThe knowledge translation paradigm: historical, philosophical, and practice perspectivesAcad Emerg Med2007141192492717704350
- WilliamsCAPreparing the next generation of scientists in translation researchWorldviews Evid Based Nurs20041Suppl 1S73S7717129339
- RamaswamiAZimmermanJBIntegrating developed and developing world knowledge into global discussions and strategies for sustainability. 2. Economics and governanceEnviron Sc Technol2007411034223017547158
- LapaigeVLa Santé Publique Globalisée [Globalized Public Health]Québec, CanadaLes Presses de l’Université Laval2009
- Pablos-MendezAShademaniRKnowledge translation in global healthJ Contin Educ Health Prof2006261818616557508
- ZwarensteinMReevesSKnowledge translation and interprofessional collaboration: where the rubber of evidence-based care hits the road of teamworkJ Contin Educ Health Prof2006261465416557506
- WeinsteinSMStrategic partnerships: bridging the collaboration gapJ Infus Nurs200427529730115385893
- IsraelBAParkerEACommunity-based participatory research: lessons learned from the Centers for Children’s Environmental Health and Disease Prevention ResearchEnviron Health Perspect2005113101463147116203263
- IsraelBASchulzAJParkerEABeckerABReview of community-based research: assessing partnership approaches to improve public healthAnnu Rev Public Health1998191732029611617
- Canadian Health Services Research FoundationIssues in Linkage and Exchange Between Researchers and Decision makers Available from: http://www.chsrf.ca/knowledge_transfer/pdf/linkage_e.pdf. Accessed September 14, 2008.
- JonesLWellsKStrategies for academic and clinician engagement in community-participatory partnered researchJAMA2007297440741017244838
- MacaulayACPromoting participatory research by family physiciansAnn Fam Med20075655756018025494
- MinklerMWallersteinNCommunity-Based Participatory Research for Health: From process to outcome2nd edSan Francisco, CAJossey-Bass2008
- LapaigeVGosselinPBélangerDSanté et Adaptation aux Changements Climatiques: Quel transfert de connaissances intégré et comment? [Colloque organisé en partenariat avec l’Institut national de santé publique du Québec]78e Congrès de l’Association francophone pour le savoir (ACFAS)2010 May 10Montreal, Canada
- BaumbuschJSemeniukPMcDonaldHEasing the transition between hospital and home: translating knowledge into actionCan Nurse20071038242917990402
- BoisselJPAmsallemECucheratMNonyPHaughMCBridging the gap between therapeutic research results and physician prescribing decisions: knowledge transfer, a prerequisite to knowledge translationEur J Clin Pharmacol200460960961615378222
- BowenSMartensPThe Need to Know TeamDemystifying knowledge translation: learning from the communityJ Health Serv Res Policy200510420321116259686
- BucknallTKnowledge transfer and utilization: implications for home healthcare pain managementJ Healthc Qual2006281121916681296
- CurtisLJMacMinnWJHealth-Care Utilization in Canada: 2 Years of Evidence SEDAP Research Paper No. 190,McMaster UniversityOntario2007
- DrakeREGoldmanHHLeffHSImplementing evidence-based practices in routine mental health service settings [comment]Psychiatr Serv200152217918211157115
- EstabrooksCAThompsonDSLovelyJJEHofmeyerAA guide to knowledge translation theoryJ Contin Educ Health Prof2006261253616557511
- FrankJDi RuggieroEMowatDMedlarBDeveloping knowledge translation capacity in public health: the role of the National Collaborating CentersCan J Public Health2007984I112
- GagnonMPLegaréFFortinJPLamotheLLabrecqueMDuplantieJAn integrated strategy of knowledge application for optimal e-health implementation: a multi-method study protocolBMC Med Inf Decis Mak2008817
- GrahamIDLoganJInnovations in knowledge transfer and continuity of careCan J Nurs Res20043628910315369167
- GrahamIDLoganJHarrisonMBLost in knowledge translation: time for a map?J Contin Educ Health Prof2006261132416557505
- GrimshawJMSantessoNCumpstonMKnowledge for knowledge translation: the role of the Cochrane CollaborationJ Contin Educ Health Prof2006261556216557512
- HuninkMGlasziouPDecision Making in Health and Medicine. Integrating Evidence and ValuesCambridge, MACambridge University Press2005
- KernerJFKnowledge translation versus knowledge integration: a “funder’s” perspectiveJ Contin Educ Health Prof2006261728016557513
- KilianBJBinderLSMarsdenJThe emergency physician and knowledge transfer: continuing medical education, continuing professional development, and self-improvementAcad Emerg Med200714111003100717967962
- LandryRAmaraNPablos-MendezAShademaniRGoldIThe knowledge-value chain: a conceptual framework for knowledge translation in healthBull World Health Organ200684859760216917645
- LavisJNResearch, public policymaking, and knowledge-translation processes: Canadian efforts to build bridgesJ Contin Educ Health Prof2006261374516557509
- MittonCAdairCEMcKenzieEPattenSBWaye PerryBKnowledge transfer and exchange: review and synthesis of the literatureMilbank Q200785472976818070335
- Rycroft-MaloneJTheory and knowledge translation: setting some coordinates [comment]Nurs Res2007564 SupplS78S8517625479
- ShortellSMRundallTGHsuJImproving patient care by linking evidence-based medicine and evidence-based managementJama2007298667367617684190
- StrausSEGrahamIDMazmanianPEKnowledge translation: resolving the confusionJ Contin Educ Health Prof20062613416557515
- ThompsonGNEstabrooksCADegnerLFClarifying the concepts in knowledge transfer: a literature reviewJ Adv Nurs200653669170116553677
- TitlerMGMethods in translation scienceWorldviews Evid Based Nurs200411384817147757
- GrimshawJKT researchCIHR IHSPR-IPPH 7th Annual Summer Institute: Innovation in knowledge translation research and knowledge translation2008 June 22–25Cornwall, Ontario, Canada
- BeckURisk Society: Towards a new modernityLondon, UKSage Publications1992
- ForayDThe Economics of KnowledgeBoston, MAMIT Press2004
- Canadian Institutes of Health ResearchAbout Knowledge TranslationOttawa, CanadaCIHR Available from: http://www.cihr-irsc.gc.ca/e/29418.html. Accessed September 17, 2009.
- Agency for Healthcare Research and QualityTranslating Research into Practice Available from: http://grandts.nih.gov/grants/guide/pa-files/PA-02-066.html. Accessed October 10, 2006.
- DiderichsenFEvansTWhiteheadMThe social basis of disparities in healthEvansTWhiteheadMDiderichsenFBhuiyaAWirthMChallenging Inequities in Health: From Ethics to ActionNew York, NYOxford University Press2001
- DenisJLLehouxPChampagneFA knowledge utilization perspective on fine-tuning dissemination and contextualizing knowledgeLemieux-CharlesLChampagneFUsing Knowledge and Evidence in Health Care. Multidisciplinary PerspectivesToronto, CanadaUniversity of Toronto Press20041840
- LabontéRSchreckerTPackerCRunnelsVGlobalization and Health–Pathways, Evidence and PolicyNew York, NYRoutledge2009
- LeeKHealth Impacts of Globalization: Towards Global GovernanceBasingstoke, UKPalgrave Macmillan2003
- LeeKGlobalization and Health: An IntroductionBasingstoke, UKPalgrave Macmillan2004
- WallaceBCToward Equity in Health: A new global approach to health disparitiesNew York, NYSpringer2008
- TashakkoriATeddlieCHandbook of Mixed Methods in Social and Behavioral ResearchThousand Oaks, CASage Publications2003
- MorseJMApproaches to qualitative-quantitative methodological triangulationNurs Res19914021201232003072
- MorseJMPrinciples of mixed methods and multimethod research designTashakkoriATeddlieCHandbook of Mixed Methods in Social and Behavioral ResearchThousand Oaks, CASage Publications2003189208
- LavisJNDaviesHOxmanADenisJLGolden-BiddleKFerlieETowards systematic review that inform health care management and policy makingRes Pol200510Suppl 13548
- ChecklandPBScholesJSoft Systems Methodology in ActionChichester, UKJohn Wiley and Son1990
- FennessyGBursteinFUsing Soft Systems as a Methodology for Researching Knowledge Management ProblemsMonash, AustraliaSchool of Information Management and Systems, Monash University2006 Available from: http://ftp.informatik.rwth-aachen.de/Publications/CEUR-WS/Vol-72/026%20Fennessy%20SSM.pdf. Accessed September 14, 2008.
- FennessyGDeveloping a Model for Knowledge Management within the Context of Evidence-Based Health CareSHIMR 2000 5th International Symposium on Health Information Management Research2000 June 12–13Sheffield, UK
- GibbonsMLimogesCNowotnyHSchwartzmanSScottPTrowMIntroductionGibbonsMLimogesCNowotnyHSchwartzmanSScottPTrowMThe New Production of Knowledge: The Dynamics of Science and Research in Contemporary SocietiesLondon, UKSage Publications1994116
- NowotnyHScottPGibbonsMRe-thinking Science: Knowledge and the Public in an Age of UncertaintyCambridgePolity Press2001
- ViensCHainsSProgramme de Recherche participative et évaluative visant l’Optimisation de la gestion des milieux de travail: Application de Connaissances, Transfert d’expertise, Interventions novatrices, Formation de leaders transformationnels (Pro-Actif)Canadian Health Services Research Foundation (FCRSS)2006–2010
- MillerSImpact of mixed methods and design on inference qualityTashakkoriATeddlieCHandbook of Mixed Methods in Social and Behavioral ResearchThousand Oaks, CASage Publications2003423455
- ErzbergerCKelleUMaking inferences in mixed methods: the rules of integrationTashakkoriATeddlieCHandbook of Mixed Methods in Social and Behavioral ResearchThousand Oaks, CASage2003457488
- ErzbergerCPreinGTriangulation: validity and empirically based hypothesis constructionQual Quant19972141154
- ScholteJAGlobalization – A Critical Introduction2nd edBasingstoke, UKPalgrave Macmillan2005
- LabonteRSpiegelJSetting global health research prioritiesBMJ200332672272312676822
- RischardJFHigh NoonNew York, NYBasis Books2002
- LapaigeVEvidence-based decision-making within the context of globalization: a “why-what-how” for leaders and managers of health care organizationsRisk Man Healthc Pol200923546
- LapaigeVProjet de programme de chaire. Chaire d’application transfrontières des savoirs “Climat, santé, écoapprentissages”En collaboration avec l’Institut national de santé publique du Québec (P. Gosselin). Présenté au Comité directeur du Plan d’action 2006–2012 sur les changements climatiques-Volet santéQuébec, Canada2009
- Gouvernement du Québec, Ministère du Développement durable, de l’Énergie et des ParcsLe Québec et les changements climatiques. Un défi pour l’avenirQuébec, CanadaGouvernement du Québec2008
- Gouvernement du Québec, Ministère du Développement durable, de l’Énergie et des ParcsTroisième bilan de la mise en æuvre du plan d’ action 2006–2012 sur les changements climatiques. Le Québec en actionQuébec, CanadaGouvernement du Québec2009
- WallaceBCIntroduction: the forces driving and embodied within the new field of equity in healthWallaceBCToward Equity in Health: A New Global Approach to health DisparitiesNew York, NYSpringer2008138
- Registry of Knowledge TranslationGlossaryHamilton, OntarioNational Collaborating Centre for Methods and Tools Available from: http://www.nccmt.ca/registry/glossary-eng.html. Accessed May 26, 2009.