Abstract
Post-coronary artery bypass grafting encephalopathy (CABGE) is associated with cognitive decline in a significant number of post-cardiac surgery cases. Patients may experience this condition as a result of being maintained on a heart-lung machine, which is referred to as the “pump”. The pump is used to circulate oxygenated blood during heart or valve surgery and may contribute to complication with oxygen flow to the brain. In some cases, the emotional traumatic effects of CABGE may produce symptoms of anxiety that can often mimic the cognitive decline associated with cardiac bypass and use of the pump. When this is the case, cognitive–behavioral assessment may be useful in helping patients to differentiate symptoms generated by anxiety from those produced by the effects of the pump. A discussion section addresses further implications of such overlapping symptoms and therapeutic strategies for treatment and remediation, along with the potential adverse effects that may occur through psychotherapy.
Despite improvements in surgical and anesthesiological techniques, persistent higher cognitive dysfunction frequently occurs in post-cardiac surgery patients, particularly when coronary artery bypass grafts (CABG) are involved (CitationSelnes and McKhann 2002). CABG is one of the most commonly performed surgical procedures in the US (CitationMushinski 1997). It is also reported that some degree of encephalopathy complicates CABG recovery and is evident in as many as three quarters of patients at the time of discharge from the hospital and a third of the patients after 6 months (CitationNewman et al 2001). Pre- and post-CABG neuropsychological testing has documented, reported, or measured cognitive dysfunction in 80%–90% of patients (CitationDiegeler et al 2000; CitationMark and Newman 2002). Post-coronary artery bypass grafting encephalopathy (CABGE) may include symptoms of confusion, diminished concentration, and loss of short-term memory, and of word and face recognition. These symptoms may persist for up to 5 years post-CABG. In the CitationNewman et al (2001) study, among the 261 patients who underwent CABG, the incidence of cognitive decline was found to be 53% of patients upon discharge, 36% at 6 weeks, 24% at 6 months, and 42% at 5 years. Moreover, cognitive dysfunction at discharge was a significant predictor of long-term higher cognitive dysfunction.
The etiology of the long-term cognitive changes remains unclear. To date, none of the long-term follow-up studies have included a control group, particularly one with similar cardiovascular risk factors. This confounds the determination as to whether the degree of cognitive decline is attributed to the cardiopulmonary bypass procedure, cerebral micro-infarctions, age-related factors, or anxiety.
In some of these cases, the etiology may clearly be the result of age-related factors. In others, however, it may be the result of procedures involving a heart-lung machine known as the “pump”, which is routinely used in cardiac surgery. The idea behind the pump is for it to perform the function of the heart and lungs while the surgical procedure is taking place. A potential problem with this procedure involves the clamping of the blood vessels or the passage of blood through the heart-lung pump. Both may release microemboli in the form of atherosclerotic debris, such as fat particles, blood clots, calcific plaque, or even air bubbles that may, in turn, travel distally to occlude the blood vessels and deprive the tissues of oxygen. When this condition occurs in the brain, it results in a shower of emboli that produces scattered cortical micro-infarcts that can contribute to cognitive impairment post-operatively. These are often identified on B-scan magnetic resonance imagery (MRI); however, some may be too small to be detected. Even red blood cells can be damaged as they journey through the machine, losing their capacity to carry sufficient oxygen to the brain and the rest of the body. As a result, patients may experience cognitive impairment, or what is defined as, “a decrease in one’s performance of various cognitive skills”, such as diminished long- and short-term memory and retrieval, concentration, or attention difficulties and slowed reaction times. Cognitive impairment occurs in at least 20% of cases from baseline even when neuroimaging findings are often normal. At times, patients may complain of a “cognitive spaciness”, or difficulty in organizing their thoughts and perceptions, and that they do not feel “quite right”, thus giving rise to the term “pumphead” (CitationMark and Newman 2002). Interestingly, the effects of varying states of anxiety can produce many similar symptoms, and have been reported in the literature as a potential confounding aspect with other medical conditions (CitationDattilio 2000, Citation2001, Citation2005; CitationDattilio and Castaldo 2001).
A major challenge for practitioners may be in differentiating the etiology of such symptoms, especially those that tend to linger beyond the usual post-operative phase. This is particularly important because medications, such as benzodiazepines, that alleviate anxiety may worsen cognitive function in patients with CABGE owing to other causes. Consequently, measures for detecting anxiety-driven symptoms can be extremely helpful here, along with cognitive–behavioral techniques for reducing such symptoms. The use of cognitive–behavioral therapy as an effective treatment of anxiety has been well documented in the research literature (CitationDattilio and Salas-Auvert 1999; CitationBarlow 2002), and several anxiety measures have been used successfully to determine degrees of anxiety. One of the more popular instruments is the Anxiety Disorder Interview Schedule-IV (ADIS-IV) (CitationDiNardo et al 1994), a structured interview process designed to assess conditions for anxiety and mood disorders according to the DSM-IV. It also evaluates the presence of coexisting disorders, such as depression, and aids clinicians in rendering a differential diagnosis between anxiety disorder and other states. In addition, the ADIS-IV evaluates symptom severity, degree of impairment, and clinical history, and is widely used by clinicians and in research facilities that treat panic. Psychological or neuropsychological testing is rarely administered as a baseline prior to surgical procedures, because such testing is expensive and requires time. Therefore, a comparison of any pre- or post-surgical symptomatology is unlikely. However, the use of a post-surgical anxiety assessment may be a way to rule out the origin of symptoms, particularly if such assessment measures can tap into anxiety traits that may have existed premorbidly. For example, the ADIS-R may identify characteristics of anxiety disorders that would have their roots in other than just reactionary circumstances. Assessment measures such as the State-Trait Anxiety Inventory (STAI) would also indicate long-standing anxiety traits (CitationSpielberger et al 1970).
The Wechsler Intelligence Scales are another measure that may be helpful in pre- and post-assessment. These scales are an individually administered composite intelligence test that appears in a battery format. They assesses different areas of intellectual abilities. The Wechsler Intelligence Scales are considered to be among the best psychological tests, because they have sound psychometric properties and produce information that is relevant to practitioners (CitationWatkins et al 1995; CitationCamara et al 2000). These are all areas in which cognitive impairment may occur during the post-operative phase.
The following is a case example of a patient who, after suffering a CABGE, developed prolonged symptoms that were attributed to chronic anxiety rather than prolonged neurological effects of the pump.
Case example
Sol, a 48-year-old Caucasian male, experienced a sudden myocardial infarction while swimming, but did not lose consciousness. He was taken to the hospital where he underwent emergency coronary bypass surgery and remained on a cardiac pump for several hours. There were no reported complications during the bypass procedure, which was successful, and Sol recovered uneventfully. However, he began to report post-operative cognitive deficits that were discovered after extubation and his awakening from anesthesia. This condition initially included disorientation, some general “spaciness”, and agnosia (the loss of ability to recognize familiar objects). Sol’s surgeon informed him that this was not unusual, and was probably the result of CABGE. He was informed that these neurological symptoms eventually would abate, but they created significant arousal and fear for Sol, who complained that he detested being “out of control” and “feeling strange”. Sol was described by his family and friends as a “type A personality, an ambitious driven man who headed a top accounting firm”. Thus, over time, the anxiety he experienced served to exacerbate his feeling as though he simply “couldn’t get his head clear”. He reported that he did not feel as mentally sharp as he had before the surgery, and that he simply couldn’t shake the “fog” from his head. Moreover, he developed a fear that he would never be able to shake free of this sensation and that it would impair his future work performance.
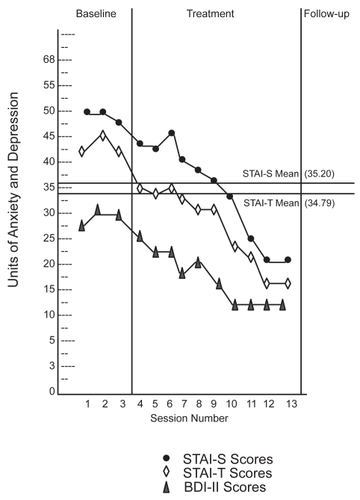
A psychological and neurological consult was ordered by Sol’s cardiovascular surgeon and attending cardiologist to assess his symptoms and to attempt to determine whether they were neurologically induced by a lack of oxygen at the time of the CABG, or were a product of his anxiety subsequent to the surgery or reflective of a pre-surgical state of anxiety. Several preliminary tests were administered 1 week post-operatively, including administration of the Wechsler Adult Intelligence Scale-III (WAIS-III), along with working memory. In addition, several anxiety measures were applied, some of which had the potential to tap into obsessional traits, such as the STAI, the ADIS-R, and the Thought Control Questionnaire. He was also administered the Beck Depression Inventory-II (BDI-II) (CitationBeck and Steer 1987). The results of these latter measures appear in .
Figure 1 Sol’s level of anxiety and depression.
Results
The results of the psychological testing suggested that Sol’s condition was caused by anxiety, not by encephalopathy. A further clue to the diagnosis was that the symptoms improved dramatically when benzodiazepines were given post-operatively, but worsened when the medication was discontinued at discharge. Several of the psychological test results were of great significance. Sol’s WAIS-III scores indicated that all of the subtests that measured cognitive functioning were within the above average to superior range. Such subtests scores as digit span–coding and matrix reasoning measure immediate rote recall and reversibility, the ability to shift thought patterns, and visual, spatial, and abstract reasoning. Symbol search, which measures the speed of processing information and encoding skills, as well as mazes that measure nonverbal reasoning, all fell within the superior range. Sol had also maintained good language development and logical abstractive (categorical) reasoning.
Even though Sol did display noticeable anxiety (fidgetiness and frequent sighing) while performing these subtests, his anxiety did not hamper his skill at achieving high scores. His responses to the anxiety measures were of particular interest. The results of the ADIS-R indicated that he was prone to obsessive–compulsive behaviors and generalized anxiety. He was extremely self-conscious about his cognitive faculties, as evidenced on the Thought Control Questionnaire and the Beck Anxiety Scale. The results of the STAI also indicated that Sol’s anxiety had been a dominant trait in his life.
In addition, Sol’s ongoing anxiety was measured by several instruments, such as the STAI and the BDI, which was also used to monitor his depression level since depression can be common subsequent to cardiac surgery. The results showed that Sol suffered a high level of anxiety in reaction to CABG, which, in itself, created acute anxiety, with obsessive symptoms as part of the syndrome. Consequently, Sol was diagnosed with anxiety disorder due to a medical condition, namely CABG secondary to a generalized anxiety disorder with obsessive features.
Sol’s pre-operative history described him as a “Type A personality”, who aimed for perfection. While he was not necessarily what would be characterized as a “perfectionist”, he was a high achiever professionally, having built and expanded his firm from a one-person operation to a company of 20 employees who were responsible for multimillion dollar accounts. His wife described him as mentally sharp. She also mentioned that he hated to be out of control.
During the clinical interview, Sol admitted that he had prided himself on being able to “think positively” and to push “unwanted thoughts” quickly out of his head. He truly believed that this discipline was the secret of his success. However, he felt that his surgery had diminished his potential, and he feared being “less sharp” and “attuned” to his environment, which would inevitably result in his demise.
It was suggested that Sol undergo treatment for anxiety reduction and cognitive mediation in order to attempt to reduce his level of anxiety and overall symptomatology. It was further determined that using such an intervention might be helpful in ruling out any residual neurological disorder. Sol had refused any additional anxiolytic medication, fearing that it might further “cloud his thinking”. In addition, he was against the use of “drugs” or medications because they were “unnatural”, in his view, and he expressed a desire to rely on psychotherapy alone.
Course of treatment
Sol was introduced to the cognitive–behavioral model of anxiety, particularly anxiety that occurred in the wake of a surgical procedure. The first step in treatment was psychoeducational, and it was designed to educate Sol about the properties of anxiety and how they are generated by the autonomic nervous system. Sol learned that peripheral vascular irregularities are not necessarily reasons for alarm. Although these symptoms are similar to those that may occur as a result of being maintained on the pump, there is also evidence that they may be exacerbated, or even generated, by anxiety. It was important for Sol to bear in mind, however, that he had previously experienced a genuine cognitive decline, or what he describes as “fuzziness”, as a result of the surgery and the pump on which he had been maintained, which would have a significant effect on his ability to reassure himself that what he was undergoing was benign autonomic activity.
The difficulty in Sol’s situation lay in the criteria that would be used to help him cognitively differentiate symptoms of anxiety from true symptoms caused by the pump. As is often the case with autonomic activity that may be compared with a heart attack, there is substantially more overlap or crossover. Thus, it was explained to Sol that the one method of determining the etiology of some of the symptoms might be progressive muscle relaxation and other relaxation techniques that would allow the symptoms of anxiety to abate, whereas they would have no effect on symptoms that were physiologically induced by the pump. The peripheral vascular symptoms, such as dizziness, fogginess, and difficulty in concentrating, were the points to be targeted.
Subsequent to this explanation of symptoms, Sol was taught progressive muscle relaxation and deep-breathing exercises. In addition, psychological components were discussed, particularly specific thoughts that could contribute to the exacerbation of his anxiety symptoms, including such thoughts as “The condition is permanent”, as well as other behaviors that provoked anxiety and led to the belief that his symptoms would produce lasting disability.
In addition, Sol was taught to reinterpret his body sensations in a different way, one that would allow him to view them as benign and not catastrophic. This was achieved by applying criteria to connotate the difference between the re-onset of the effects of the pump and the symptoms of anxiety. Again, the defining criteria pertained to whether relaxation-induced methods could cause the symptoms to abate, which would be a further indication that they were anxiety-driven, as opposed to their having no effect on him, which would signify that they were more permanent. This list was constructed with the cooperation of the attending neurologist in an attempt to better distinguish between these symptoms. If cognitive coping strategies and behavioral training had little or no effect on the condition, then it was agreed that it would serve as a clear indication that the condition was not anxiety-induced.
The STAI was used to monitor anxiety during the course of treatment. The BDI-II was also used to monitor his level of depression (see ).
Results showed a significant improvement in Sol’s symptoms in 8 weeks of treatment. This improvement was measured not only by reports on the Anxiety and Depression Scales, but also by Sol’s verbal reports. The use of the depression scale was implemented in order to monitor for any depression that might develop during the interim.
It was clear that his fears about his condition and about losing control of his faculties were inadvertently producing many of the symptoms of anxiety that mimic those produced by being on the pump.
Discussion
The aforementioned case is an excellent example of how premorbid anxiety existing prior to a medical procedure such as a CABG may exacerbate, and even mimic, symptoms that could otherwise be legitimately produced as an ancillary effect of a particular procedure.
An important question emerges: How can practitioners best prepare for pre-existing anxiety states that may affect patients during the early post-operative stages of a procedure? The estimated prevalence of pre-existing cognitive impairment in intensive-care units was reported in one study with an older population as being 31%–42%, depending on the instrument used (CitationPisani et al 2003). In addition, it is important to clinically differentiate the etiology of the symptoms in order to treat the patient effectively. It should be noted that it can be difficult to determine the severity of symptoms, since, in many cases, regardless of the etiology, the symptoms are perceived as threatening. However, an attempt must be made to help individuals cope with benign activities, particularly because such incidents may lead to false alarms and unnecessary complications during the recovery period. In the case of Sol, the use of cognitive–behavioral techniques was highly effective in helping to differentiate among, as well as eliminate, the reported symptoms.
It is not unusual for individuals to experience anxiety after such medical procedures, particularly when they may be accompanied by negative side-effects that they are experiencing for the first time. The Surgeon General of the United States recently confirmed the widespread prevalence of anxiety disorders. Therefore, it is a good likelihood that a fair number of candidates who submit for cardiac procedures will be prone to anxiety during the course of such procedures. Perhaps pre-screening for anxiety should be a priority in order to determine which patients may be susceptible to post-surgical anxiety, particularly anxiety with symptoms that mimic those that are seen with CABGE.
Secondly, the treatment of such anxiety is most immediately remediated by the use of pharmacotherapy, such as benzodiazepines or antidepressant compounds, which has been proven to be safe (CitationHansen 2003). In cases in which patients refuse such pharmacologic treatments, alternatives such as psychotherapy may be helpful. In the aforementioned case, the use of cognitive–behavioral techniques was effective as an alternative to medication.
While the potential risk of harm to post-cardiac patients is very low using psychotherapy, some does exist (Allen and Scheidt 1998; CitationLinden 2000). This has mostly to do with the potential effects of stress that is generated by discussing emotionally charged content. This may be particularly so in interventions such as group psychotherapy. It appears that the benefits of cognitive–behavioral techniques (stress reduction and the balancing of thoughts) far outweighs the risks (further confusion and the stress of restructuring one’s thinking) that may occur as a result of psychotherapy in general.
Acknowledgments
The authors wish to express their gratitude to Eric Frey of Lehigh University for his assistance in the literature search on this topic, as well as Raymond Singer for his helpful comments on an earlier draft of the article.
References
- AllanRScheidtS1998Group psychotherapy for patients with coronary heart diseaseInt J Group Psychother481872149563238
- BarlowDH2002Anxiety and its disorders: The nature and treatment of anxiety and panic2nd edNew YorkGuilford
- BeckATSteerG1987Manual for the revised Beck Depression Inventory San Antonio, TXThe Psychological Corporation
- CamaraWJNathanJSPuerdeAE2000Psychological test usage: Implications in professional psychologyProf Psychol Res Pr3114154
- DattilioFM2000Letter: Education and symptoms of anxiety in the wake of neurological illnessesJ Neuropsychiatry Clin Neurosci143545
- DattilioFM2001Cognitive-behavioral treatment of panic complicated by medical illnessPsychotherapy3821217
- DattilioFM2005Anxiety induced tremors in a 13-year-old female with ideopathic Parkinson diseaseJ Neuropsychiatry Clin Neurosci17912
- DattilioFMCastaldoJE2001Differentiating symptoms of panic from relapse of Guillaine-Barré syndromeHarv Rev Psychiatry9260511553530
- DattilioFMSalas-AuvertJA1999Panic disorder: Assessment and treatment through a wide-angle lensPhoenix, AZZieg, Tucker & Sons
- DieglerAHirschRSchneiderF2000Neuromonitoring and neurocognitive outcome in off-pump versus conventional coronary bypass operationAnn Thorac Surg691162610800812
- DiNardoPABrownTABarlowDH1994Anxiety Disorders Interview Schedule for DSM-IV: Lifetime Version (ADIS-IV-L)San Antonio, TXPsychological Corporation/Graywind Publications, Inc
- HansenS2003Mental health issues associated with cardiovascular disease in womenPsychiatr Clin North Am2669371214563104
- LindenW2000Psychological treatments in cardiac rehabilitation: Review of rationales and outcomesJ Psychosom Res484435410880665
- MarkDBNewmanMF2002Protecting the brain in coronary artery bypass graft surgeryJAMA28714485011903033
- MushinskiM1997Average charges for coronary artery bypass grafts and precutaneous transluminal coronary angioplasties, 1995Stat Bull Metrop Insur Co782089029706
- NewmanMFKrichnerJLPhillips-Bute2001Longitudinal assessment of neurocognitive function after coronary-artery bypass surgeryN Engl J Med344395911172175
- PisaniMInouyeSKMcNicollL2003Screening for pre-screening cognitive impairment in older intensive care unit patientsJ Am Geriatr Soc51591812752832
- SelnesOAMcKhannG2002Late cognitive decline after CABGE: inevitable or preventable?Neurology59660112221153
- SpielbergerCDGorsuchRLLusheneR1970Manual for the State-Trait Anxiety Inventory (form Y)Palo Alto, CAMind Garden
- WatkinsCECampbellVLNieberdingR1995Contemporary practice of psychological assessment by clinical psychologistsProf Psychol Res Pr265460