Abstract
Enormous progress has been made in the treatment of Parkinson’s disease (PD). As a result of advances in experimental therapeutics, many promising therapies for PD are emerging. Levodopa remains the most potent drug for controlling PD symptoms, yet is associated with significant complications such as the “wearing off” effect, levodopa-induced dyskinesias and other motor complications. Catechol-o-methyl-transferase inhibitors, dopamine agonists and nondopaminergic therapy are alternative modalities in the management of PD and may be used concomitantly with levodopa or one another. The neurosurgical treatment, focusing on deep brain stimulation, is reviewed briefly. Although this review has attempted to highlight the most recent advances in the treatment of PD, it is important to note that new treatments are not necessarily better than the established conventional therapy and that the treatment options must be individualized and tailored to the needs of each individual patient.
Medical treatment of Parkinson’s disease
Enormous progress has been made in the treatment of Parkinson’s disease (PD) over the past half century, but levodopa remains the most potent drug for controlling PD symptoms (CitationJankovic 2008a). Prior to instituting medical therapy, a correct diagnosis of PD must be established and the level of impairment (motor, sensory, autonomic and mental) determined (). Each patient’s therapy is to be individualized, and diverse drugs other than levodopa are presently available. Among these are the dopamine agonists (DA), catechol-o-methyl-transferase (COMT) inhibitors and nondopaminergic agents (). Head-to-head comparisons of drugs within classes are rare, and the differences that have emerged are related to the effects on motor fluctuations, dyskinesias, on/off times and adverse effects of the specific agents within each class (CitationJankovic and Stacy 2007).
Figure 1 Pharmacologic treatment options available for PD.
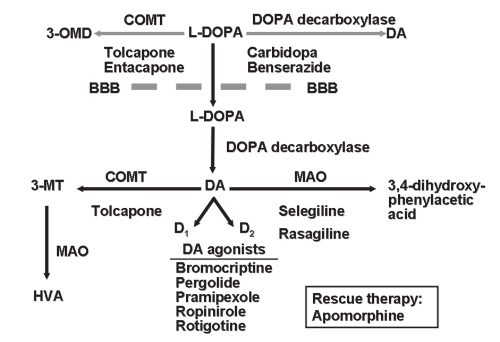
Table 1 Guidelines for treatment of Parkinson’s disease
Levodopa
Levodopa is the most potent drug for controlling PD symptoms, particularly those related to bradykinesia (CitationJankovic 2002a). However, because levodopa therapy is frequently associated with motor complications, such as fluctuations and dyskinesias, there is ongoing debate as to when in the course of PD it is most appropriate to initiate levodopa therapy (CitationStern 2004; CitationWeiner 2004). The addition of carbidopa, a peripheral dopa decarboxylase inhibitor, enhances the therapeutic benefits of levodopa. In patients who are particularly sensitive to peripheral side effects such as nausea and vomiting, additional carbidopa (Lodosyn®) may be added to the conventional carbidopa/levodopa preparation.
A majority of patients treated with levodopa experience motor fluctuations, dyskinesias or other complications after 5 years of treatment (CitationJankovic 2005). Since motor fluctuations and dyskinesias are primarily related to the dose and duration of levodopa treatment (CitationSchrag and Quinn 2000), most parkinsologists advocate therapeutic strategies designed to delay the onset of levodopa therapy in order to delay the onset of levodopa-related motor complications (CitationJankovic 2002b).
The reported frequency of motor complications between the different studies varies, partly because of differences in definitions of the thresholds for recognizing motor complications (CitationMarras and Lang 2003). One of the most common problems in patients taking levodopa is delayed onset of response after ingesting a dose of levodopa. A delay in achieving “on” state or a total response failure accounted for more than 60% of daily “off” time among 327 patients with advanced PD (CitationBlindauer et al 2003).
There are different types of levodopa-induced dyskinesias, such as the “peak-dose dyskinesias”, “biphasic dyskinesias” and “wearing-off” dyskinesias (CitationFahn 2000; CitationJankovic 2002a). Besides cumulative dose and duration of levodopa treatment, there are other risk factors that should be considered before initiating levodopa therapy. Young-onset PD patients seem particularly likely to develop levodopa-induced dyskinesias. Certain genetic forms of PD, such as PARK2 and PARK8 have been associated with a higher risk of levodopa-related motor complications (CitationLucking et al 2000; CitationSchrag and Schott 2006).
There are three strategies designed to improve levodopa-induced dyskinesias: 1) reduce the dosage of levodopa, 2) use drugs known to ameliorate dyskinesias, and 3) surgery. Several drugs, including amantadine, have been reported to improve levodopa-induced dyskinesias without necessitating the reduction in levodopa dosage (CitationVerhagen Metman et al 1999). The addition of a COMT inhibitor, MAO-I inhibitor or a dopamine agonist inhibitor may be used in the management of levodopa-induced motor complications (CitationJankovic et al 2007) (). Other drugs with antidyskinetic effect include clozapine, fluoxetine, propranolol, the cannabinoid receptor agonist nabilone, and fipamezole. Some of the new antiepileptic drugs are being investigated as potential therapies for levodopa-induced dyskinesias. For example, levetiracetam (Keppra®) was found to significantly reduce levodopa-induced dyskinesias in MPTP-lesioned marmosets (CitationHill et al 2003). In patients with severe motor fluctuations, apomorphine, a subcutaneous dopamine agonist, may be used as rescue therapy (CitationPietz et al 1998).
Table 2 Antidyskinesia drugs
The “wearing off” effect, the most frequent form of motor fluctuation, appears to be related to the shortening of levodopa’s half-life in the striatum as a result of impaired capacity to store and buffer the striatal concentration of levodopa, due to a loss of striatal dopaminergic terminals (CitationVerhagen Metman et al 2000). Amantadine, a NMDA receptor blocker, has been found to ameliorate motor fluctuations in parkinsonian animals and patients (CitationVerhagen Metman et al 2000; CitationPereira et al 2005). In patients with “wearing-off” and “on-off” phenomena, the response to apomorphine, a postsynaptically acting dopamine agonist, is shortest and steepest in patients with the most severe motor fluctuations (CitationManson et al 2002). In addition, apomorphine is capable of sustaining a long-duration response (CitationNutt and Carter 2000).
Strategies designed to prolong and smooth out the therapeutic concentrations of levodopa-related motor fluctuations usually improve by increasing the frequency of administration of levodopa. Slow-release preparations of levodopa, such as Sinemet® CR, offer the possibility of “smoothing out” clinical fluctuations by slowly releasing the levodopa from a special matrix. In addition to prolonging the “on” time, smoothing out the wearing off response and reducing the total number of doses and tablets taken per day, Sinemet CR also seems helpful in alleviating troublesome nighttime rigidity, thus allowing patients to have more restful nights and better nighttime mobility. Potential disadvantages of Sinemet CR over standard preparations include delayed or poor response after the morning dose (absence of the “morning kick”) and an exacerbation and prolongation of peak-dose dyskinesias.
Continuous dopaminergic stimulation (CDS) has been advocated as a strategy to prevent or control levodopa-related motor fluctuations presumably associated with pulsatile stimulation associated with levodopa dosing, although this concept has been challenged (CitationNutt 2007). CDS methods include duodenal infusions of levodopa, oral solutions of levodopa made by dissolving it with ascorbic acid in water, a dispersible form of levodopa (Etilevodopa®), subcutaneous or intramuscular injections of levodopa ethylester, and intravenous (and intraventricular) administration of levodopa methyl ester, but the latter methods are not practical and have not translated into clinical practice (CitationStocchi et al 2005).
COMT inhibitors
Another strategy to prolong DA response utilizes the inhibition of COMT by drugs such as entacapone (Comtan®). Entacapone, because of its short half-life, requires frequent administration (200 mg, up to 8 times per day); most patients take entacapone with each dose of levodopa (CitationSchrag 2005). Tolcapone (Tasmar®), another COMT inhibitor, is rarely used because of a report of three cases of acute fulminant liver failure (CitationAssal et al 1998; CitationOlanow et al 2000) leading to black box warning and intensive monitoring requirements (CitationEllison 1998). The safety and tolerability of adjunctive tolcapone initiated simultaneously with levodopa was recently evaluated, with a focus on changes in liver transaminases and potential hepatotoxicity (CitationLees et al 2007). In this study, 677 levodopa-naive patients in early stages PD were randomized to receive placebo or tolcapone 100 mg three times daily, added to standard doses of levodopa plus carbidopa or benserazide. In both placebo and tolcapone treated patients, there were mild elevations in transaminase levels, less than 3 times the upper limit of normal (ULN), whereas potentially serious increases of up to or over 3 times the ULN were infrequent (1.8% in the tolcapone treated group compared to 1.2% in those treated with placebo, p = 0.5), supporting the safe use of tolcapone in selected patients who are monitored for potential liver toxicity. According to current CitationFDA recommendations (1998), the monitoring should include serum alanine aminotransferase (ALT) and aspartate aminotransferase (AST), prior to starting treatment with tolcapone. These enzymes should be monitored every two weeks for the first year, every 4 weeks for the next 6 months and then every 8 weeks thereafter. Prior to increasing tolcapone, ALT and AST levels should be monitored and subsequently scheduled at the above mentioned frequency.
Theoretically, the COMT inhibitors have an advantage over Sinemet CR in that they do not delay the absorption of levodopa and, although they increase the levodopa plasma concentration, they do not increase the time to reach the peak concentration or the maximal concentration of levodopa (CitationRuottinen and Rinne 1998). While this pharmacologic action of the COMT inhibitors may prolong the “on” time without markedly increasing dyskinesias, most studies do report increased levodopa-induced dyskinesia in patients taking COMT inhibitors, requiring a substantial (>25%) reduction in daily levodopa dosage. Thus patients, with and without fluctuations, benefit from the addition of entacapone to their levodopa treatment. Except for nausea and increased dyskinesia, entacapone is usually well tolerated. Early intervention, such as phone calls to the patients, clearly improves compliance, and this translates into not only increased “on”-time and reduced levodopa dosage, but also further improvement in quality of life measures (CitationGrandas et al 2007).
In 2003, the US FDA approved triple combination tablets (Stalevo®) containing carbidopa, levodopa, and entacapone for end-of-dose wearing off. In a randomized, crossover study of 132 healthy subjects, the levodopa AUC (area under the curve) was essentially the same when used in the triple combination versus when administered separately, indicating equivalent pharmacokinetics (CitationHeikkinen et al 2003; CitationHauser 2004).
Dopamine agonists
The possibility that levodopa is neurotoxic, and that the onset of levodopa-induced complications may be related to the duration of treatment, are the two most important reasons why many experts recommend delaying levodopa therapy until parkinsonian symptoms clearly begin to interfere with patients’ functioning and normal lifestyle. In order to delay or prevent levodopa-induced complications many parkinsonologists recommend using DA agonists as the initial or early form of dopaminergic therapy (CitationJankovic 2000). When used as monotherapy, DA agonists provide only modest improvement in parkinsonian symptoms, but the improvement may be sufficient to delay the introduction of levodopa by several months or years.
Dopamine agonists (DA) exert their pharmacologic effect by directly activating DA receptors, bypassing the presynaptic synthesis of DA. Experimental and clinical studies have provided evidence that activation of the D2 receptors is important in mediating the beneficial antiparkinsonian effects of DA agonists, but concurrent D1 and D2 stimulation is required to produce optimal physiological and behavioral effects (CitationBrooks 2000) (). In contrast to the traditional DA agonists (bromocriptine and pergolide), pramipexole and ropinirole are nonergolines and therefore are expected to have a lower risk of complications such as peptic ulcer disease, vasoconstrictive effects, erythromelalgia, pulmonary and retroperitoneal fibrosis, and valvular heart disease (CitationTintner et al 2005; CitationRoth 2007; CitationZanettini et al 2007). Pramipexole often causes dose-dependent and idiosyncratic peripheral edema (CitationTan and Ondo 2000). Because of the potential for valvular heart disease, the ergot dopamine agonists have been essentially discontinued from medical practice.
Table 3 Pharmacology of dopamine agonists
Pramipexole has been shown to be a safe and effective drug when used as monotherapy in early stages of PD (CitationParkinson Study Group 2002) and in mild to moderate PD (CitationWeiner et al 2001). In addition to its beneficial effects on the PD clinical symptoms and levodopa sparing (about 25% reduction in daily levodopa dosage), pramipexole has been demonstrated to possibly exert a neuroprotective effect and to enhance neurotrophic activity in mesencephalic dopaminergic cultures (CitationZou et al 1999).
Ropinirole has been also demonstrated to be effective in early PD (CitationKorczyn et al 1999; CitationRascol et al 2000). In clinical practice, dosages high as 24 mg may be needed to achieve optimal response (CitationKorczyn et al 2002). Some studies have shown that dosages of ropinirole as high as 35 mg per day are safe and provide additional benefits in patients with advanced PD (CitationCristina et al 2003). In addition to increasing dosages of DA agonists, several studies have explored the potential for synergistic effects of combined DA agonist therapy. For example, CitationStocchi et al (2003) found in an open label study that the addition of cabergoline to other DA agonists significantly improved the UPDRS scores and motor fluctuations and that dual DA agonist therapy may be useful in patients with PD with or without levodopa.
Meta-analysis comparing adverse effects of ropinirole to pramipexole showed that there was no significant difference in the risk of dizziness, nausea, or hypotension with either drug individually or in combination when compared with levodopa (CitationEtminan et al 2003). The use of ropinirole appeared to be associated with a higher risk of hypotension and somnolence as compared with pramipexole when compared with placebo and the use of pramipexole appeared to be associated with a higher risk of hallucinations than use of ropinirole when compared with placebo.
Apomorphine is a water soluble DA and is consequently suitable for intravenous, subcutaneous, sublingual, or intranasal administration (CitationOndo et al 1999a; CitationPoewe and Wenning 2000). Subcutaneous injections or continuous infusions have been found useful even in advanced PD by reducing the “off” time without necessarily increasing dyskinesias (CitationPietz et al 1998). In our study of sublingual apomorphine in patients with advanced PD, we found a marked reduction in the UPDRS score, an increase in “on” time, an increase in tapping speed, and a significant reduction in levodopa dosage (CitationOndo et al 1999b). Several reports have also suggested that apomorphine may exert a neuroprotective effect in MPTP animals and other models (CitationGrünblatt et al 1999). A formulation of a novel highly selective D2 DA agonist, rotigotine, in a silicone based transdermal system (4.5–18 mg/patch) approved by the FDA in 2007 for the treatment of early PD (CitationJankovic et al 2007; CitationWatts et al 2007), has also been found to be effective in the treatment of advanced PD (CitationLeWitt et al 2007). The improvement in the UPDRS appears to be dose-dependent, and the drug was well tolerated at plasma levels that produce clinical improvement at doses of 8.4 to 67 mg, except for some side effects usually associated with DA agonists, such as somnolence, nausea, vomiting, and occasional skin irritation (CitationParkinson Study Group 2003; CitationPoewe and Leussi 2005). Rotigotine (Neupro®) is available as 2 mg, 4 mg, and 6 mg per day patches. In March 2008, Schwarz Pharma, the German pharmaceutical company who developed the drug, now marketed by UCB Pharma, announced their decision to withdraw the drug from the US market due to formation of crystals in the patches, which interferes with the absorption of the drug into the skin. The company is currently working diligently to correct the problem and is consulting with the FDA to make sure that future supplies meet the highest quality standards.
Although levodopa is clearly the most effective drug for the treatment of motor symptoms of PD, whether levodopa should be used in early stages of PD or delayed until later in the disease process has been the subject of many debates. This debate is partly fueled by the observation that in patients with early onset PD (particularly before the age of 40), their disease course is longer and they have a particularly high risk for developing motor fluctuations and dyskinesias. The argument to delay levodopa therapy is chiefly supported by studies showing that early use of dopamine agonists delays the need for levodopa and thus delays the onset of levodopa-related motor complications, particularly motor fluctuations and dyskinesias, and that dopamine agonists may exert favorable disease-modifying effects (CitationLe and Jankovic 2001; CitationParkinson Study Group 2002; CitationSimpkins and Jankovic 2003; CitationWhone et al 2003). The strategy of early initiation of levodopa is supported by studies that indicate that levodopa provides a longer period of superior motor control, slower progression of disability, longer life expectancy (CitationLees et al 2001; CitationRajput et al 2002), and no difference in “clinically relevant” dyskinesias between levodopa and dopamine agonist treated patients (CitationLees et al 2001). There is a lower incidence of hallucinations, vomiting, and leg edema with levodopa as compared to dopamine agonists (CitationWhone et al 2003), and no in vivo evidence of levodopa toxicity (CitationLe and Jankovic 2001). Since younger patients seem to be at a higher risk of levodopa-related motor complications, delaying levodopa therapy seems to be a prudent practice at least in this population of PD patients.
Nondopaminergic therapy
In addition to the dopaminergic drugs, nondopaminergic drugs, such as the anticholinergics and amantadine, may provide satisfactory symptomatic relief in early phases of anti-PD therapy. The anticholinergic drugs, such as trihexyphenidyl or benztropine, are particularly useful in younger patients who are primarily bothered by tremor. Although quite effective, their usefulness is limited by the anticholinergic side effects such as cognitive impairment, dry mouth and urinary symptoms. The tricyclics are often used not only because of their antidepressant effects, but also because of their anticholinergic properties. Mirtazapine (Remeron®), a novel antidepressant that enhances noradrenergic and serotonergic transmission and acts as a presynaptic alpha-2, 5HT2, and 5HT3 receptor antagonist, has been reported to improve rest tremor and levodopa-induced dyskinesia (CitationPact and Giduz 1999). Istradefylline, a novel adenosine antagonist, has been also reported to provide modest benefit in PD patients with levodopa-related motor complications (CitationJankovic 2008b). Rapid eye movement (REM) sleep behavior disorder (RBD), which may be the initial manifestations of Parkinsonism, may respond to night-time clonazepam. Drooling (sialorrhea), one of the most embarrassing symptoms of PD caused by impaired swallowing, has been successfully treated with botulinum toxin injections (CitationBhatia et al 1999; CitationPal et al 1999; Sheffield and Jankovic 2007).
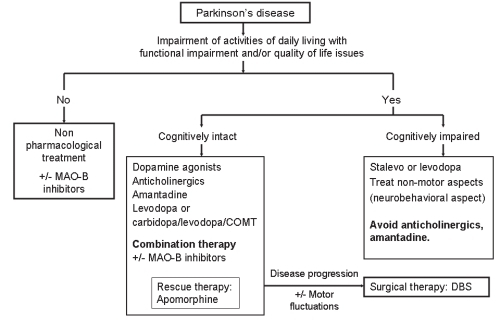
The most important principle in the management of PD is to individualize therapy and to target the most disabling symptoms. The selected therapy should be based on scientific rationale and designed not only to control symptoms, but also to slow the progression of the disease (). Since younger patients are likely to require dopaminergic therapy for longer time and are at increased risk for the development of levodopa complications, levodopa sparing strategies, such as the use of MAO inhibitors and DA agonists, are even more critical in this population (CitationJankovic 2000). Certain symptoms of PD, such as dysarthria, dysphagia, freezing and other “axial” symptoms, usually do not respond to dopaminergic therapy and may be mediated by nondopaminergic systems (CitationBonnet 2000; CitationKompoliti et al 2000). It is very likely that with better understanding of the mechanisms of neurodegeneration, novel and more effective therapeutic strategies will be available in the near future.
Figure 2 Treatment guidelines for the progressive stages of Parkinson’s disease.
Adjunctive therapy
While neuroprotective strategies slow or halt the progression of the disease, these strategies must be implemented early (CitationSchapira 2004). Clinically relevant effects of putative neuroprotective agents are difficult to measure and so more and more studies utilize not only clinical ratings, but also ancillary techniques, such as 18F-l-DOPA PET and 123I β-CIT SPECT, to longitudinally measure the progression of nigrostriatal degeneration.
The finding that deprenyl (selegiline) prevents MPTP-induced Parkinsonism has stimulated interest in antioxidative therapy as a means of retarding progression of PD and other neurodegenerative diseases. In the largest clinical trial designed to address the potential protective effects of selegiline, “Deprenyl and Tocopherol Antioxidative Therapy of Parkinsonism” (DATATOP), the outcomes of treatments with deprenyl, alpha-tocopherol (vitamin E) and a combination of these putative antioxidants in comparison to a placebo were compared. The results showed that deprenyl-treated patients reached the end-point 9 months after the group treated with placebo or tocopherol. The waning of the effects of selegiline on delaying end-point after the first year, coupled with slight but significant improvement in motor performance after initiation of selegiline and slight (nonsignificant) worsening after 1-month washout, has been used as an argument in favor of predominantly symptomatic rather than protective effect. In a follow up study, levodopa treated PD patients who have been taking selegiline for 7 years, compared to those who were changed to placebo after 5 years, showed significantly slower decline, less wearing off, on-off motor fluctuations, and less freezing, but more dyskinesias (CitationShoulson et al 2002). This is consistent with another study of the same patient population, which showed that patients randomized to selegiline had a lower risk of freezing than those assigned to placebo (CitationGiladi et al 2001).
In clinical studies, rasagiline, a selective, irreversible MAO B inhibitor, provides a modest benefit as an adjunctive therapy in PD patients experiencing levodopa related motor fluctuations. A double-blind, placebo-controlled trial showed that after a 10-week treatment with rasagiline, 12 of 43 (28%) of patients had an improvement in total UPDRS score of 30% or greater, compared with none in the placebo group (p < 0.05) (CitationStern et al 2004). In an 18-week, double-blind trial of 687 patients randomized to receive once-daily rasagiline, entacapone (with each dose of levodopa), or placebo (the LARGO trial), both rasagiline and entacapone reduced “off” time by 1.2 hours as compared with placebo (0.4 hour reduction, p ≤ 0.0001). The mean daily dose of levodopa was reduced on rasagiline and on entacapone, and was increased on placebo (CitationRascol et al 2005). Other variables showed that rasagiline was superior to placebo and to entacapone in reducing UPDRS motor score, and at least as effective as entacapone in reducing “off” time compared to baseline (CitationParkinson Study Group 2005).
In one study of 80 patients with early PD, CitationShults and colleagues (2002) found that in comparison to placebo, 1200 mg of CoQ10 was associated with a slower decline in UPDRS and a positive trend in decline UPDRS decline favoring CoQ10. In this study, patients never previously treated with l-DOPA were randomized to receive placebo or one of three doses of CoQ10: 300, 600, or 1200 mg/day. In addition, they were also receiving 300 IU vitamin E, which was thought to act as a carrier of CoQ10 across the blood-brain barrier. The patients were followed for 16 months or until they required l-DOPA. The drug was found to be well tolerated, and there was no difference in adverse effects between CoQ10 and placebo. When compared to baseline, the group receiving placebo deteriorated by 12 points in the UPDRS, whereas patients receiving 1200 mg deteriorated by only 6.7 points. Furthermore, patients receiving CoQ10 had on the average 44% less decline in mental function, movement and ability to perform daily living tasks than the placebo group. This difference was statistically significant only for the 1200 mg/day group, but there was no difference between placebo and the lower dose groups. Treatment did not delay the disability severe enough to require l-DOPA. The study was highly suggestive, yet was not definitive. There is no evidence that vitamin supplements, including vitamin C and E, or carotenoids reduce the risk of PD (CitationZhang et al 2002). Further studies are needed to determine whether CoQ10 and other quinines, such as idebenone, may serve as either substitutive electron carriers or antioxidant compounds in disorders with known or suspected mitochondrial dysfunction.
Antiglutamatergic drugs
Interactions between dopamine and glutamate in striatal medium spiny neurons have been found to play an important role in PD, and there is considerable theoretical and experimental support for the use of glutamate antagonists as potential neuroprotective drugs (CitationChase and Oh 2000). Several studies have demonstrated that the neuronal activity is increased in the subthalamic nucleus (STN) and in the internal segment of globus pallidum (GPi) of parkinsonian animals and humans (Obeso et al 2000a). Since STN provides excitatory, glutamatergic input to GPi, glutamate inhibition would be expected to improve Parkinsonism. Some studies indeed have shown that N-methyl-D-aspartate (NMDA) antagonists prevent the selective toxicity of MPP+ and that an ablation of STN attenuates the loss of DA neurons in rats exposed to the mitochondrial toxin 3-nitroproprionic acid (3-NP) or the catecholamine toxin (6-OHDA) (CitationNakao et al 1999). Certain anticholinergic drugs and amantadine posses NMDA-blocking properties and amantadine have been shown to not only ameliorate parkinsonian symptoms, but also to improve motor fluctuations and levodopa induced dyskinesias (CitationVerhagen Metman et al 1999; CitationLuginger et al 2000).
Future therapies
One particularly promising therapeutic and potentially neuroprotective approach involves the use of neurotrophic factors, such as neurturin (NTN) (CitationKordower et al 2006) and the glial cell-line-derived neurotrophic factor (GDNF) (CitationGash et al 1998). These trophic factors have been reported to enhance the survival of midbrain dopaminergic neurons in vitro and to rescue degenerating neurons in vivo. These encouraging observations have led to a pilot human trial of GDNF administered by an implanted intracerebroventricular catheter in patients with moderately advanced PD conducted in several centers in North America. However, because of lack of observed efficacy and frequent occurrence of nausea, anorexia, tingling (L’hermitte’s sign), hallucinations, and depression, these trials were suspended (CitationNutt et al 2003). In a one-year follow-up of five patients with PD in whom GDNF was continuously infused directly into the putamen, there were no serious clinical side effects, a 39% improvement in the off-medication motor sub-score of the UPDRS and a 61% improvement in the activities of daily living sub-score. Furthermore, levodopa-induced dyskinesias were reduced by 64% and, in contrast to fetal implants (see below) there were no off dyskinesia. This clinical improvement was accompanied by a 28% increase in putamen PET F-DOPA uptake (CitationGill et al 2003). Results from a recently completed multicenter trial, however, show no benefit from GDNF (CitationLang et al 2006) and further studies have been suspended because of evidence of cerebellar toxicity in experimental primates.
CERE-120 is an adeno-associated virus type 2 (AAV2) vector encoding human NTN (AAV2-NTN). In a recent open label trial, 12 patients with advanced PD were stereotactically administered bilateral intraputaminal CERE-120 (CitationMarks et al 2006). Two doses were evaluated, with six patients in each cohort. UPDRS and off-medication motor scores improvement of 20% and 25%, respectively, were observed at both three and six months in the low dose cohort. Improvement in the total off-medication motor scores was approximately 26% and 22%, respectively, at three months in the high dose cohort. Rigidity and bradykinesia measurements showed the greatest improvement, off-time was reduced by 27% and “on”-time was doubled without dyskinesias through six months in the low dose cohort, with similar trends in the high dose cohort. The intraputaminal administration of CERE-120 was well tolerated. Ongoing double-blind clinical trials are under way to determine the efficacy and safety of CERE-120 in patients with PD.
In addition to neurotrophic factors, other therapeutic possibilities currently being investigated include retinal pigment epithelial cells (hRPE). These cells, located in the inner layer of neural retina, produce levodopa. When attached to cross linked gelatin microcarriers (Spheramine®) and implanted stereotactically into the striatum, the cells have improved parkinsonian symptoms in rodents, nonhuman primates and parkinsonian patients. A pilot, open label study of 6 patients showed 48% improvement in the UPDRS motor score after implantation in the most affected postcommissural putamen. All patients tolerated the implantation of Spheramine well and demonstrated improvement. At 6, 9, and 12 months postoperatively, the mean UPDRS-Motor score “off”, the primary outcome measure, improved 33%, (n = 6), 42% (n = 6), and 48% (n = 3), respectively. No “off-state” dyskinesias were observed (CitationWatts et al 2003). The 48% improvement was maintained at 24 months (CitationStover et al 2005a).
Treatment of neurobehavioral features
Treatment of cognitive deficits associated with PD is as challenging as the treatment of Alzheimer’s disease and other dementias. While the general assumption has been that cognitive deficits are a feature of late-stage PD, clinically inapparent cognitive changes on neuropsychiatric testing may be found (CitationWilliams-Gray et al 2006). With the introduction of cholinesterase inhibitors such as donepezil (Aricept®), rivastigmine (Exelon®), and galantamine (Reminyl®,) and the NDMA antagonist memantine (Namenda®) (CitationReisberg et al 2003), it is possible that cognition, orientation and language function will improve, and that such improvement will lead to a meaningful improvement in function. Both donepezil and rivastigmine improve cognition to the same effect, but donepezil is better tolerated (CitationWilkinson et al 2002). The largest and best-designed study of rivastigmine in dementia associated with PD involved 541 patients enrolled in a 24-week randomized, multicenter, double-blind clinical trial (CitationEmre et al 2004). The patients had a relatively mild dementia (MMSE 10–24), with onset of dementia about 2 years after onset of PD symptoms. The mean ADAS-cog score, the primary efficacy variable, improved by 2.1 points in the rivastigmine group, compared to 0.7 in the placebo group (p < 0.001), and the MMSE improved by 0.8 in the rivastigmine group and worsened by 0.2 in the placebo group (p = 0.03). At the end of the study, 55.5% were receiving 9 to 12 mg. The adverse effects that were significantly more frequent in the rivastigmine group were nausea, vomiting, dizziness, and tremor.
Rivastigmine should be started at 1.5 mg BID and increased at 4-week intervals to 3 mg BID and eventually to 6 mg BID. This slow titration is designed to prevent potential side effects such as nausea, vomiting, agitation and weight loss. In a recent database study conducted by the VA, over 4.5 million subjects were reviewed, with analysis restricted to those patients over 65 years who did not have a prior diagnosis of Alzheimer’s or Parkinson’s disease. The use of simvastatin was associated with a reduction in incident dementia; and after adjusting for cardiovascular disease, hypertension, diabetes and the use of neuroleptics, simvastatin was also observed to be associated with a reduced incidence of PD (CitationWolozin et al 2007).
In addition to motor side effects related to levodopa therapy, many PD patients experience a variety of psychiatric reactions, particularly psychosis with agitation, delusions, paranoid beliefs and hallucinations (CitationFénelon et al 2000). In PD patients with new symptoms of confusion or psychosis, factors unrelated to PD and PD-related treatment must be identified prior to modifying therapies or adding antipsychotics. Psychotic symptoms can be controlled by reducing the dosage of dopaminergic drugs (levodopa, dopamine agonists) and eliminating all other drugs that are not absolutely essential. CitationBorek and colleagues (2007) suggested eliminating anticholinergics first, followed by amantadine, monoamine oxidase inhibitors, dopamine agonists, COMT inhibitors, then reducing the amount of levodopa. Atypical antipsychotics offer the best strategy for controlling drug-induced psychosis without the need to adjust the dosage of dopaminergic drugs (CitationFriedman and Factor 2000). While quetiapine has been used successfully based on open label findings, two double-blind studies did not find significant differences in the management of psychosis in patients with PD when compared with placebo (CitationOndo et al 2005a; CitationRabey et al 2007). Other atypical antipsychotics such as risperidone, olanzapine, ziprasidone and aripiprazole have been found to worsen motor performance without demonstrating statistically significant improvement of dopamine-induced psychosis (CitationRich et al 1995; CitationBreier et al 2002; CitationOndo et al 2002; CitationFriedman et al 2006). This is in contrast with studies where quetiapine (CitationMancini et al 2004; CitationMerims et al 2006) and ziprasidone (CitationGomez-Esteban et al 2005) improved the psychotic symptoms without causing variation in their motor performance. Treatment with atypical neuroleptics, such as clozapine, has been associated with improved prognosis (CitationFactor et al 2003). The use of clozapine has been limited due to the potential to cause agranulocytosis, which is an idiosyncratic reaction, and not dose-related (CitationFernandez et al 2003). Cholinesterase inhibitors such as donepezil (CitationFabbrini et al 2002) and rivastigmine (CitationReading et al 2001) have been found to be beneficial, without worsening of the UPDRS, in small, open label studies.
Depression has an estimated prevalence of 40%–50%, and is one of the most common behavioral disturbances in PD (CitationTandberg et al 1996; CitationZesiewicz et al 1999). It may present at any stage of the disease, and may precede the appearance of motor symptoms (CitationCummings 1992). Risk factors for PD-related depression include female sex, a history of depression, early-onset PD (ie, before the age of 55 years) and “atypical” Parkinsonism (eg, prominent akinesia/rigidity or extensive vascular disease) (CitationWeintraub et al 2007). The subthalamic nucleus has been implicated in mood disorders in PD patients, as deep brain stimulation (DBS) has been found to have antidepressant, depressive and mania-inducing effects (CitationTakeshita et al 2005). Because depressive symptoms, such as flat affect, anxiety, cognitive impairment, fatigue, weight loss, and sleep disturbances often overlap with those of PD, diagnosis is often under-recognized. In a cohort of over 400 newly diagnosed patients with PD, followed for an average of 14.6 months, 27.6% (114) screened positive for depression. Of these, 40% were neither treated nor referred for psychiatric evaluation (CitationRavina et al 2007). The same study found depression to be a significant predictor of more impairment in activities of daily living and increased need for symptomatic therapy of PD. Given the effects of depression on motor function and quality of life, prompt recognition and early treatment are integral aspects in the management of PD. Tricyclic antidepressants, while not necessarily the drug of first choice (due to their side effect panel), may be considered in the treatment of depression in PD (CitationMiyasaki et al 2006). The anticholinergic properties of the TCAs may be helpful in PD patients with drooling, overactive bladder and insomnia. Selective serotonin reuptake inhibitors (SSRIs) have been recommended as first-choice antidepressants in PD considering their tolerability, and acceptable side effect profile and drug-drug interactions (CitationBorek et al 2007). There are some conflicting data whether the selective serotonin receptor inhibitors (SSRIs) exacerbate Parkinsonism, but a study of 30 PD patients, (CitationCeravolo et al 2000) found paroxetine, one of the typical SSRIs, at doses of 20 mg/day, to be safe and effective in the treatment of depression associated with PD. Caution must be exercised when using selegiline in combination with SSRIs and TCAs, as there is a small but increased risk of developing a serotonin syndrome. Antiparkinsonian medications, such as selegiline (CitationAllain et al 1991; CitationBaronti et al 1992), bromocriptine (CitationJouvent 1983), pergolide (CitationRektorova et al 2003) and pramipexole (CitationBarone et al 2003) have been reported to have antidepressant effects.
Like depression, anxiety has been reported in up to 40% of PD patients (CitationStein et al 1990; CitationVasquez et al 1993); similarly, anxiety may precede the appearance of motor symptoms by many years, and usually before onset of depression (CitationShiba et al 2000). The most common anxiety disorders in PD are panic disorder, generalized anxiety disorder and social phobia (CitationVasquez et al 1993; CitationRichard 2005). Anxiety has been reported to occur in patients experiencing “on-off” states, particularly the “off” period (CitationStein et al 1990; CitationVasquez et al 1993). In these instances, adjustment of antiparkinsonian medications may be effective in managing anxiety. SSRIs, with their favorable side effect profile, are used as first-line treatment; onset of anxiolytic effects usually occurs between 2 and 4 weeks, with dose adjustment after 1 month (CitationBorek et al 2007).
Apathy is characterized by loss of motivation, and diminished goal-directed behavior. It affects over 10% of PD patients, and is believed to be due to prefrontal lobe dysfunction (CitationStarkstein et al 1992; CitationLuck et al 2002). Apathy is independent of depression and anxiety, being mainly determined by cognitive impairment (CitationDujardin et al 2007). With no known treatment, antidepressants are given in the hope that the apathy is a component of a depressive syndrome (CitationBorek et al 2007).
Impulse control disorders (ICDs) have been described in PD patients treated with dopamine agonists (CitationVoon 2004), and consist of punding, compulsive gambling, compulsive shopping, compulsive eating, and hypersexuality. The first impulsive behavior described in patients with PD was punding and was initially attributed to treatment with levodopa (CitationFriedman 1994). Punding behavior, an intense fascination with repetitive, aimless behavior, as first described in amphetamine and cocaine abuse, is presumed to be secondary to dopaminergic excess. It has since been reported to occur in PD patients treated with dopamine agonists (CitationKurlan 2004). The incidence of punding varies from 1.4% to 14% (CitationEvans et al 2004; CitationMiyasaki et al 2007). CitationEvans and colleagues (2004) noted that punding in patients with PD occurred rather frequently and was associated with the use of either or both l-DOPA and dopamine agonists. They also suggested that requirements for large doses of dopaminergic therapy, frequent rescue doses and the use of rescue medications overnight should raise suspicion and prompt queries into patients’ pastimes. Patients complaining of sleep disturbance should also be asked specifically how they cope with periods of sleep deprivation. Punding may also be suspected if the addition of further dopaminergic therapy at night exacerbates rather than benefits patient’s insomnia. In the study by CitationEvan and colleagues (2004), patients with l-DOPA equivalent units (LEU) greater than or equal to 800 were recruited. Of these, punders were more likely to use apomorphine and cabergoline, and less likely to use entacapone. Increasing clinical severity of the punding behavior significantly correlated with higher total daily LEU dose, younger age, reduced sleep time overnight, and average number of daily rescue doses suggesting patients with punding may have dopa dysregulation.
Pathological gambling has been attributed by some to the use of dopamine agonists, but this putative association has not been confirmed (CitationDriver-Dunckley et al 2003; CitationDodd et al 2005). Younger age at PD onset, higher novelty seeking traits, and a personal or family history of alcohol use disorders have been found to be associated with a greater risk for pathological gambling with dopamine agonists (CitationVoon et al 2007). Contrary to typical obsessive-compulsive disorders, punding and other ICDs respond poorly to SSRIs, clomipramine and antipsychotics (CitationEvans et al 2004; CitationKurlan 2004). Treatment options such as decreasing the dose of DA, or switching to a different DA, produce the best results (CitationBorek et al 2007; CitationMiyasaki et al 2007).
Excessive daytime sleepiness (EDS), sleep fragmentation, altered dreaming and RBD affect over three-quarters of PD patients (CitationFriedman and Chou 2004). The existence of other causes of EDS, such as obstructive sleep apnea, use of sedative medication and the presence of concurrent medical illnesses must be established and treated. Both pramipexole and ropinirole (and possibly other DA agonists) have been associated with irresistible sleep attacks leading to motor vehicle mishaps (CitationFrucht et al 1999; CitationHauser et al 2000; CitationBrodsky et al 2003). Sleepiness correlated significantly with a longer duration of PD, more advanced PD, male gender, and the use of any DA (CitationOndo et al 2001). The soporific effects of the three most common DA (pramipexole, ropinirole, and pergolide) and even levodopa were similar (CitationOndo et al 2001; CitationBrodsky et al 2003). The risk of accidents can be prevented by discussing this potential side effect with the patient and their family, by warning them not to drive if they feel drowsy, and by encouraging them to take short naps on the side of the road as needed (CitationReyner and Horne 1998). Modafinil (Provigil®) at 100 to 200 mg twice a day is effective in reversing the excessive daytime drowsiness and the sedative effects of anti-PD medications (CitationHauser et al 2000; CitationOndo et al 2001), although a recent double-blind, placebo-controlled study failed to significantly improve EDS in PD patients when compared to placebo (CitationOndo et al 2005b). Vivid and often violent dreams, with prominent motor activity and loss of normal atonia during REM sleep characterize RBD. TCAs, SSRIs and MAO inhibitors can induce or aggravate RBD. Clonazepam is considered the treatment of choice with effectiveness in about 90% of patients (CitationGagnon et al 2006).
The nonmotor side effects of levodopa, such as hallucinations and orthostatic hypotension, are dose-related and these adverse effects could offset the potential benefits of prolonged motor response. In addition to adjusting levodopa dosing, reductions of anticholinergic drugs may also ameliorate dyskinesias. Dystonia often improves with the administration of baclofen, anticholinergic drugs, DA agonists, lithium, and local injections of botulinum toxin.
Neurosurgical treatments of Parkinson’s disease
It is beyond the scope of this manuscript to comprehensively review neurosurgical treatment of PD. Only a brief review will be provided here and the reader is referred to other published literature on for additional information about this important therapeutic strategy. The renewed interest in surgical treatment of movement disorders has been stimulated in part by improved understanding of the functional anatomy underlying motor control, as well as refinement of methods and techniques in neurosurgery, neurophysio logy, and neuroimaging (CitationJankovic 2001; CitationKrauss et al 2001).
Besides thalamotomy and pallidotomy, another promising surgical approach for the treatment of tremors and other movement disorders is high-frequency DBS via electrodes implanted in the VIM nucleus of the thalamus, GPi, STN or other subcortical nuclei. The mechanism of electrical stimulation is not known, but the following explanations have been offered: 1) disruption of the network (“jamming” of feedback loop from the periphery), 2) depolarization block, 3) preferential activation of inhibitory neurons, and 4) a functional ablation by desynchronizing a tremorogenic pacemaker.
Thalamic stimulation appears to be particularly effective in the treatment of parkinsonian tremor and ET. Our experience at Baylor is similar to that reported in other centers. In a blinded and open label trial of unilateral thalamic DBS in 33 patients (14 ET and 19 PD) with severe tremor refractory to conventional therapy, both groups of patients demonstrated a statistically significant decrease (p < 0.0001) in observed contralateral arm tremor, respectively (CitationOndo et al 1998). All measures of tremor, including writing samples, pouring tests, subjective functional surveys, and disability scores significantly improved. To compare thalamic DBS with thalamotomy, CitationSchuurman and colleagues (2000) conducted a prospective, randomized study of 68 patients with PD, 13 with ET, and 10 with multiple sclerosis. They found that the functional status improved more in the DBS group as compared to the thalamotomy group and tremor was suppressed completely or almost completely in both the DBS group and in the thalamotomy group. Although one patient in the DBS group died after an intracerebral hemorrhage, DBS was associated with significantly fewer complications than thalamotomy. In addition to improving distal tremor associated with PD and ET, VIM DBS can effectively control ET head tremor, which usually does not respond to conventional therapy.
Since bilateral thalamotomy can cause hypophonia, dysarthria, and dysphagia, DBS is now considered the best alternative, particularly in those patients who require bilateral procedures. Thalamotomy has the advantage over DBS in that there is no need for hardware, and for patients with disabling bilateral tremor, unilateral thalamotomy in combination with contralateral DBS may offer the optimal tremor control with the fewest adverse side effects. Chronic stimulation of the thalamus appears to be well tolerated and the risk of local gliosis is minimal (CitationHaberler et al 2000), although more extensive damage has been rarely reported (CitationHenderson et al 2002). Because of the ability to customize the stimulation parameters and the relatively low risk of complications, DBS is now considered the preferred surgical treatment for disabling PD-related tremor or ET.
Several studies have demonstrated that DBS of the GPi and STN improves parkinsonian symptoms and prolongs the “on” time (CitationLinizasaro 2003), as well as other aspects of quality of life (CitationDiamond and Jankovic 2005). The relative safety and efficacy of STN vs GPi DBS, however, has been compared formerly in only small studies (CitationBurchiel et al 1999). Although no difference between the two targets was found by Burchiel, their study had insufficient power to detect a difference between the two groups. The “off” UPDRS motor score has been reported to improve by 34% to 60% and the UPDRS ADL score by 30%–50% in patients undergoing STN or GPi DBS. Furthermore, dyskinesia has been reported to markedly improve, largely as a result of about 50% reduction in daily levodopa dosage.
Both STN and GPi DBS improve the off medication UPDRS motor score (CitationAnderson et al 2005), worsen the “on” motor states of the motor UPDRS, activities of daily living and gait, and improve the “off” medication UPDRS respect to the baseline (CitationRodriguez-Oroz et al 2005). Neither the STN nor the GPi DBS improves the “on” medication function. In a five year follow up after bilateral STN DBS on the first 49 consecutive patients, CitationKrack and colleagues (2003) found marked improvement in motor function while off medications and in dyskinesia while on medications. At five years, the LEU dose and the duration and severity of levodopa-induced dyskinesia were reduced compared to baseline. In a study of 30 patients with PD Hoehn and Yahr stages 3–4 while off medication randomized to either STN or GPi DBS, 89% improvement of dyskinesias in the GPi DBS group was observed, while in the STN DBS group, dyskinesias improved by 62% (Anderson et al 2003). Bradykinesia improved more in the STN group when compared to GPi stimulation (Anderson et al 2003), and STN DBS was associated to a greater decrease in levodopa dosage (CitationRodriguez-Oroz et al 2005), but more severe speech impairment, postural instability, and cognitive decline (Anderson et al 2003; CitationRodriguez-Oroz et al 2005). Since improvements in dyskinesia usually require a reduction in levodopa dosage, unilateral STN or GPi DBS is impractical because the side of the body contralateral to the unstimulated side would clearly worsen. Bilateral STN DBS appears to be more effective than unilateral STN DBS in improving Parkinsonism, but unilateral STN DBS may be appropriate for patients with asymmetric parkinsonian symptoms including a high amplitude tremor (CitationKumar et al 1999; CitationStover et al 2005b; CitationDiamond et al 2007). In addition to improving limb signs and the cardinal signs of PD, bilateral STN DBS has been found to also improve axial parkinsonian symptoms, particularly arising from chair and gait, but speech, neck rigidity, abnormal posture, and postural instability also improved (CitationBejjani et al 2000).
Except for mild deficit in lexical fluency, STN or GPi DBS does not appear to adversely affect cognitive performance (CitationPillon et al 2000), but some older patients have been found to have an impairment in frontal executive function (CitationSaint-Cyr et al 2000). Although bilateral STN is clearly effective in improving the cardinal as well as other parkinsonian symptoms, the procedure does not necessarily improve all the symptoms and, as a result of progression of cognitive, speech, and other deficits frequently associated with PD, the quality of life may not substantially improve in patients who exhibit these additional features (CitationHariz et al 2000).
Other therapeutic approaches
Besides conventional pharmacologic and surgical treatments, there are many other strategies currently being explored in the treatment of some PD symptoms (CitationJankovic 1999; CitationJankovic 2001) (). Speech therapy designed to stimulate increased vocal fold adduction with instructions to “increase loudness”, the so called Lee Silverman Voice Treatment (LSVT), using various verbal cues to regulate speech volume, and percutaneous collagen augmentation of the vocal folds (CitationHill et al 2003) have been used successfully to treat the hypophonic, hypokinetic dysarthria associated with PD.
Table 4 Experimental therapeutics of Parkinson’s disease
Although this review has attempted to highlight the most recent advances in the treatment of PD, it is important to note that new treatments are not necessarily better than the established conventional therapy and that the treatment options must be individualized and tailored to the needs of each individual patient (CitationJankovic 2000, Citation2002b).
Disclosure
The authors report no conflicts of interest.
References
- AllainHCougnardJNeukirchHCSelegilene in de novo parkinsonian patients: the French selegiline multicenter trialActa Neurol Scand1991136738
- AndersonVCBurchielKJHogarthPPallidal vs subthalamic nucleus deep brain stimulation in Parkinson diseaseArch Neurol2005625546015824252
- AssalFSpahrLHadengueATolcapone and fulminant hepatitisLancet1998199589752821
- BaroneIRektorIBaresMPramipexole and pergolide in the treatment of depression in Parkinson’s disease: a national multicentre prospective randomized studyEur J Neurol20031039940612823492
- BarontiFDavisTLBoldryRCDeprenyl effects on levodopa pharmacodynamics, mood and free radical scavengingNeurology19924254141549214
- BejjaniBPGervaisDArnulfIAxial parkinsonian symptoms can be improved: the role of levodopa and bilateral subthalamic stimulationJ Neurol Neurosurg Psychiatry20006859560010766889
- BhatiaKPMünchauABrownPBotulinum toxin is a useful treatment in excessive drooling of salivaJ Neurol Neurosurg Psychiatry19996769710577041
- BlindauerKthe Parkinson Study GroupDelayed response to levodopa and response failures account for a large percentage of daily off time in advanced Parkinson’s disease patients with motor fluctuationsNeurology200360812
- BonnetAMInvolvement of non-dopaminergic pathways in Parkinson’s disease. Pathophysiology and therapeutic implicationsCNS Drugs20001335164
- BorekLLChouKLFriedmanJHManagement of the behavioral aspects of Parkinson’s diseaseExpert Rev Neurother200777112517563253
- BreierASuttonVKFeldmanPDOlanzapine in the treatment of dopamimetic-induced psychosis in patients with Parkinson’s diseaseBiol Psychiatry2002524384512242060
- BrodskyMAGodboldJRothTOlanowCWSleepiness in Parkinson’s disease: A controlled studyMov Disord2003186687212784270
- BrooksDJDopamine agonists: their role in the treatment of Parkinson’s diseaseJ Neurol Neurosurg Psychiatry2000686859010811688
- BurchielKJAndersonVCFavreJComparison of pallidal and subthalamic nucleus deep brain stimulation for advances Parkinson’s disease: results of a randomized, blinded pilot studyNeurosurgery19994513758410598706
- CeravoloRNutiAPicciniAParoxetine in Parkinson’s disease: Effects on motor and depressive symptomsNeurology2000551216811071504
- ChaseTNOhJDStriatal dopamine- and glutamate-mediated dysregulation in experimental parkinsonismTINS2000238691
- CristinaSZangagliaRManciniFHigh-dose ropinirole in advanced Parkinson’s disease with severe dyskinesiasClin Neuropharmacol2003261465012782917
- CummingsJLDepression and Parkinson’s disease: a reviewAm J Psychiatry1992149443541372794
- DiamondAJankovicJThe effect of deep brain stimulation on quality of life in movement disordersJ Neurol Neurosurg Psychiatry20057611889316107348
- DiamondAShahedJJankovicJThe effects of subthalamic nucleus deep brain stimulation on parkinsonian tremorJ Neurol Sci200726019920317561121
- DoddMLKlosKJBowerJHPathological gambling caused by drugs used to treat Parkinson diseaseArch Neurol20056213778116009751
- Driver-DunckleyESamantaJStacyMPathological gambling associated with dopamine agonist therapy in Parkinson’s diseaseNeurology200361422312913220
- DujardinKSockeelPDevosDCharacteristics of apathy in Parkinson’s diseaseMov Disord2007227788417290451
- EllisonRHDear health professional letter regarding appropriate use of Tasmar1998Nutley, NJRoche Laboratories Inc
- EmreMAarslandDAlbaneseARivastigmine for dementia associated with Parkinson’s diseaseN Engl J Med200435125091815590953
- EtminanMGillSSamiiAComparison of the risk of adverse events with pramipexole and ropinirole in patients with Parkinson’s disease: a meta-analysisDrug Saf2003264394412688834
- EvansAHKatzenschlagerRPaviourDCPunding in Parkinson’s disease: its relation to the dopamine dysregulation syndromeMov Disord20041939740515077237
- FabbriniFBarbantiPAuriliaCDonepezil in the treatment of hallucinations and delusions in Parkinson’s diseaseNeurol Sci20022341312111620
- FactorSAFeustelPJFriedmanJHLongitudinal outcome of Parkinson’s disease patients with psychosisNeurology20036017566112796526
- FahnSThe spectrum of levodopa-induced dyskinesiasAnn Neurol200047211
- FénelonGMahieuxFHuonRZiéglerMHallucinations in Parkinson’s disease. Prevalence, phenomenology and risk factorsBrain20001237334510734005
- FernandezHHTrieschmannMEFriedmanJHTreatment of psychosis in Parkinson’s disease; safety considerationsDrug Saf2003266435912814332
- Food and Drug AdministrationNew Warnings for Parkinson’s Drug Tasmar19981116Rockville, MDT9881
- FriedmanJHBermanRMGoetzCGOpen-label flexible-dose pilot study to evaluate the safety and tolerability of aripiprazole in patients with psychosis associated with Parkinson’s diseaseMov Disord20062120788117013906
- FriedmanJHChouKLSleep and fatigue in Parkinson’s diseaseParkinsonism Relat Disord2004102735
- FriedmanJHFactorSAAtypical antipsychotics in the treatment of drug-induced psychosis in Parkinson’s diseaseMov Disord2000152011110752567
- FriedmanJHPunding on levodopaBiol Psychiatry19943635017993965
- FruchtSRogersJDGreenePDFalling asleep at the wheel: Motor vehicle mishaps in persons taking pramipexole and ropiniroleNeurology19995219081010371546
- GagnonJFPostumaRBMontplaisirJUpdate on pharmacology of REM sleep behavior disorderNeurology200667742716966533
- GashDMZhangZGerhardtGNeuroprotective and neurorestorative properties of GDNFAnn Neurol1998441215
- GiladiNMcDermottMPFahnSthe Parkinson Study GroupFreezing of gait in PD. Prospective assessment of the DATATOP cohortNeurology20015617122111425939
- GillSSPatelNKHottonGRDirect brain infusion of glial cell line-derived neurotrophic factor in Parkinson diseaseNat Med200395899512669033
- Gomez-EstebanJCZarranzJJVelascoFUse of ziprasidone in patients with psychosisClin Neuropharmacol200528111415965308
- GrandasFHernandezBPRACTICOMT Study GroupLong-term effectiveness and quality of life improvement in entacapone-treated Parkinson’s disease patients: the effects of an early therapeutic interventionEur J Neurol200714282917355548
- GrünblattEMandelSBerkuzkiTApomorphine protects against MPTP-induced neurotoxicity in miceMov Disord199914612810435498
- HaberlerCAleschFMazalPRNo tissue damage by chronic deep brain stimulation in Parkinson’s diseaseAnn Neurol200048372610976644
- HarizMIJohanssonFShamsgovaraPBilateral subthalamic nucleus stimulation in a parkinsonian patient with preoperative deficits in speech and cognition: Persistent improvement in mobility but increased dependency: A case studyMov Disord200015136910634253
- HauserRAWahbaMNAndersonWMModafinil treatment of pramipexole-associated somnolenceMov Disord20001512697111104221
- HauserRALevodopa/carbidopa/entacapone (Stalevo)Neurology2004626471
- HeikkinenHVarheALylyVNew levodopa, carbidopa and entacapone combination tabletsEuropean J Neurology200310164
- HendersonJMPellMO’SullivanDJPostmortem analysis of bilateral subthalamic electrode implants in Parkinson’s diseaseMov Disord200217133711835450
- HillMPBezardEBrotchieJMThe antiepileptic, levetiracetam (Keppra), modulates the process of priming for L-dopa-induced dyskinesia in MPTP-lesioned marmosetsEuropean J Neurology200310164
- JankovicJWattsRLMartinWTransdermal rotigotine: double-blind, placebo-controlled trial in Parkinson diseaseArch Neurol2007646768217502466
- JankovicJNew and emerging therapies for Parkinson’s diseaseArch Neurol1999567859010404979
- JankovicJParkinson’s disease therapy: Tailoring choices for early and late disease, young and old patientsClin Neuropharmacol2000232526111154092
- JankovicJSurgery for Parkinson’s disease and other movement disorders: Benefits and limitations of ablation, stimulation, restoration, and radiationArch Neurol2001581970211735770
- JankovicJLevodopa strengths and weaknessesNeurology2002581932a
- JankovicJJankovicJTolosaETherapeutic strategies in Parkinson’s diseaseParkinson’s Disease and Movement Disorders20024Philadelphia, PALippincott Williams and Wilkins116151b
- JankovicJMotor fluctuations and dyskinesias in Parkinson’s disease: Clinical manifestationsMov Disord200511116
- JankovicJParkinson’s disease: clinical features and diagnosisJ Neurol Neurosurg Psychiatry2008a793687618344392
- JankovicJAre adenosine antagonists, such as istradefylline, caffeine, and chocolate, useful in the treatment of Parkinson’s disease?Ann Neurol2008b63267918383071
- JankovicJStacyMMedical management of levodopa-associate motor complications in patients with Parkinson’s diseaseCNS Drugs2007216779217630819
- JouventRAbensourPBonnerAMAntiparkinsonian and antidepressant effects of high doses of bromocriptine. An independent comparisonJ Affect Disord1983514156222093
- KompolitiKWangQEGoetzCGEffects of central dopaminergic stimulation by apomorphine on speech in Parkinson’s diseaseNeurology2000544586210668714
- KorczynADBruntERLarsenJPA 3-year randomized trial of ropinirole and bromocriptine in early Parkinson’s diseaseNeurology1999533647010430427
- KorczynADThalamasCAdlerCHDosing with ropinirole in a clinical settingActa Neurol Scand2002106200412225314
- KordowerJHHerzogCDDassBDelivery of neurturin by AAV2 (CERE-120)-mediated gene transfer provides structural and functional neuroprotection and neurorestoration in MPTP-treated monkeysAnn Neurol2006607061517192932
- KrackPBatirAVan BlercomNFive-year follow up of bilateral stimulation of the subthalamic nucleus in advanced Parkinson’s diseaseN Engl J Med200334919253414614167
- KraussJKJankovicJGrossmanRGSurgery for Movement Disorders2001Philadelphia, PALippincott Williams and Wilkins1449
- KumarRLozanoAMSimeEComparative effects of unilateral and bilateral subthalamic nucleus deep brain stimulationNeurology199953561610449121
- KurlanRDisabling repetitive behaviors in Parkinson’s diseaseMov Disord2004194336915077241
- LangAEGillSPatelNKRandomized controlled trial of intraputamenal glial cell line-derived neurotrophic factor infusion in Parkinson’s diseaseAnn Neurol2006594596616429411
- LeW-DJankovicJAre dopamine agonists neuroprotective in Parkinson’s disease?J Drugs and Aging20011838996
- LeesAJKatzenschlagerRHeadJTen-year follow up of three different initial treatments in de-novo PD. A randomized trialNeurology20015716879411706112
- LeesAJRatziuVTolosaESafety and tolerability of adjunctive tolcapone treatment in patients with early Parkinson’s diseaseJ Neurol Neurosurg Psychiatry200778944817098835
- LeWittPALyonsKEPahwaRSP 650 Study GroupAdvanced Parkinson disease treated with rotigotine transdermal system: PREFER StudyNeurology2007681262717438216
- LinazasoroGVan BlercomNLasaAUnilateral subthalamic deep brain stimulation in advanced Parkinson’s diseaseMov Disord200318713612784280
- LuckGCBrownRGApathy in Parkinson’s diseaseJ Neurol Neurosurg Psychiatry2002736364212438462
- LuckingCBDurrABonifatiVAssociation between early onset Parkinson’s disease and mutations in the parkin geneNew Engl J Med200034215606710824074
- LugingerEWenningGKBöschSBeneficial effects of amantadine on dopa-induced dyskinesias in Parkinson’s diseaseMov Disord200015873811009193
- ManciniFTassorelliCMartignoniELong term evaluation of the effect of quetiapine on hallucinations, delusions and motor function in advanced Parkinson’s diseaseClin Neuropharmacol20042733715090935
- MansonAJTurnerKLeesAJApomorphine monotherapy in the treatment of refractory motor complications of Parkinson’s disease: Long-term follow up study of 64 patientsMov Disord20021712354112465062
- MarksWLVerhagen MetmanLStarrPNeurturin gene transfer for Parkinson’s disease: motor outcomes from the initial CERE-120 clinical trialMov Disord200621608
- MarrasCLangAEMeasuring motor complications in clinical trials for early Parkinson’s diseaseJ Neurol Neurosurg Psychiatry200374143612531932
- MerimsDBalasMPeretzCRater-blinded, prospective comparison: quetiapine versus clozapine for Parkinson’s disease psychosisClin Neuropharmacol200629331717095896
- MiyasakiJMAl HassanKLangAEPunding prevalence in Parkinson’s diseaseMov Disord20072211798117230464
- MiyasakiJMShannonKVoonVPractice parameter: evaluation and treatment of depression, psychosis, and dementia in Parkinson’s disease (an evidence-based review). Report of the subcommittee of the American Academy of NeurologyNeurology200666996100216606910
- NakaoNNakaiTNakaiKAblation of the subthalamic nucleus supports the survival of nigral dopaminergic neurons after nigrostriatal lesions induced by the mitochondrial toxin 3-nitropropionic acidAnn Neurol1999456405110319887
- NuttJGBurchielKJComellaCLRandomized, double-blind trial of glial cell line-derived neurotrophic factor (GDNF) in PDNeurology200360697312525720
- NuttJGCarterJHApomorphine can sustain the long-duration response to L-DOPA in fluctuating PDNeurology2000542475010636162
- NuttJGContinuous dopaminergic stimulation: Is it the answer to the motor complications of Levodopa?Mov Disord2007221916958130
- ObesoJARodriguez-OrozMCRodriguezMPathophysiology of the basal ganglia in Parkinson’s diseaseTINS200023819
- OlanowCWTasmar Advisory PanelTolcapone and hepatotoxic effectsArch Neurol2000572636710681087
- OndoWHunterCAlmaguerMEfficacy and tolerability of a novel sublingual apomorphine preparation in patients with fluctuating Parkinson’s diseaseClin Neuropharmacol19992214a10047926
- OndoWHunterCAlmaguerMSublingual apomorphine in patients with fluctuating Parkinson’s diseaseMov Disord1999146648b10435505
- OndoWJankovicJSchwartzKUnilateral thalamic deep brain stimulation for refractory essential tremor and Parkinson’s disease tremorNeurology199851106399781530
- OndoWGFayleRAtassiFModafinil for daytime somnolence in Parkinson’s disease: double blind, placebo controlled parallel trialJ Neurol Neurosurg Psychiatry20057616369b16291885
- OndoWGLevyJKVuonKVOlanzapine treatment for dopaminergic-induced hallucinationsMov Disord2002171031512360554
- OndoWGTintnerRDat VoungKDouble blind, placebo-controlled, unforced titration parallel trial of quetiapine for dopaminergic-induced hallucinations in Parkinson’s diseaseMov Disord20052095863a15800937
- OndoWGVuongKVKhanHDaytime sleepiness and other sleep disorders in Parkinson’s diseaseNeurology2001571392611673578
- PactVGiduzTMirtazapine treats resting tremor, essential tremor, and levodopa-induced dyskinesiasNeurology199953115410496290
- PalPKCalneDBCalneSBotulinum-A toxin in the treatment of sialorrhea in patients with Parkinson’s diseaseParkinsonism Relat Disord1999582
- Parkinson Study GroupDopamine transporter brain imaging to assess the effects of pramipexole vs levodopa on Parkinson disease progressionJAMA200228716536111926889
- Parkinson Study GroupA controlled trial of rotigotine monotherapy in early Parkinson’s diseaseArch Neurol2003601721814676046
- Parkinson Study GroupA randomized placebo-controlled trial of rasagiline in levodopa-treated patients with Parkinson disease and motor fluctuations: the PRESTO studyArch Neurol200562241815710852
- Pereira da Silva-JuniorFBraga-NetoPSueli MonteFAmantadine reduces the duration of levodopa-induced dyskinesia: A randomized, double-blind, placebo-controlled studyParkinsonism Relat Disord2005114495216154788
- PietzKHagellPOdinPSubcutaneous apomorphine in late stage Parkinson’s disease: a long term follow upJ Neurol Neurosurg Psychiatry199865709169810943
- PillonBArdouinCDamierPNeuropsychological changes between “off” and “on” STN or GPi stimulation in Parkinson’s diseaseNeurology200055411810932277
- PoeweWLeussiFClinical studies with transdermal rotigotine in early Parkinson’s diseaseNeurology20056511416009878
- PoeweWWenningGKApomorphine: An underutilized therapy for Parkinson’s diseaseMov Disord2000157899411009181
- RabeyJMProkhorovTMiniovitzAEffect of quetiapine in psychotic Parkinson’s disease patients: a double-blind labeled study of 3 months’ durationMov Disord200722313817034006
- RajputAHFentonMEBirdiSClinical pathological study of levodopa complicationsMov Disord2002172899611921114
- RascolOBrooksDJKorczynADA five-year study of the incidence of dyskinesia in patients with early Parkinson’s disease who were treated with ropinirole or levodopa. 056 Study GroupN Engl J Med20001814849110816186
- RascolOBrooksDJMelamedELARGO study groupRasagiline as an adjunct to levodopa in patients with Parkinson’s disease and motor fluctuations (LARGO, Lasting effect in Adjunct therapy with Rasagiline Given Once daily, study): a randomised, double-blind, parallel-group trialLancet20053659475415766996
- RavinaBCamicioliRComoPGThe impact of depressive symptoms in early Parkinson’s diseaseNeurology200769342717581943
- ReadingPJLuceAKMcKeithIJRivastigmine in the treatment of parkinsonian psychosis and cognitive impairment: preliminary findings from an open trialMov Disord20011611719511748755
- ReisbergBDoodyRStofflerAMemantine Study GroupMemantine in moderate-to-severe Alzheimer’s diseaseN Engl J Med200334813334112672860
- RektorovaIRektorIBaresMPramipexole and pergolide in the treatment of depression in Parkinson’s disease: a national multicentre perspective randomized studyEur J Neurol20031039940612823492
- ReynerLAHorneJAFalling asleep whilst driving: are drivers aware of prior sleepiness?Int J Legal Med199811112039587793
- RichSSFriedmanJHOttBRRisperidone versus clozapine in the treatment of psychosis in six patients with Parkinson’s disease and other akinetic-rigid syndromesJ Clin Psychiatry19955655698530331
- RichardIHAnxiety disorders in Parkinson’s diseaseAdv Neurol200596425516383211
- Rodriguez-OrozMCObesoJALangAEBilateral deep brain stimulation in Parkinson’s disease: a multicentre study with 4 years follow upBrain20051282240915975946
- RothBLDrugs and valvular heart diseaseN Engl J Med20073566917202450
- RuottinenHMRinneUKCOMT inhibition in the treatment of Parkinson’s diseaseJ Neurol19982452534
- Saint-CyrJATrepanierLLKumarRNeuropsychologic consequences of chronic bilateral stimulation of the STN in Parkinson’s diseaseBrain2000123209110811004126
- SchapiraAHOlanowCWNeuroprotection in Parkinson’s Disease: mysteries, myths and misconceptionsJAMA20042913586414734599
- SchragASchottJMEpidemiological, clinical and genetic characteristics of early-onset parkinsonismLancet Neurol200653556316545752
- SchragAEntacapone in the treatment of Parkinson’s diseaseLancet Neurol200543667015907741
- SchragASQuinnNDyskinesias and motor fluctuations in Parkinson’s disease. A community-based studyBrain2000123229730511050029
- SchuurmanPRBoschABossuytPMMA comparison of continuous thalamic stimulation and thalamotomy for suppression of severe tremorN Engl J Med2000342461810675426
- ShibaMBowerJHMaragnoreDMAnxiety disorders and depressive disorders preceding Parkinson’s disease: a case-control studyMov Disord2000156697710928577
- ShoulsonIOakesDFahnSImpact of sustained deprenyl (selegiline) in levodopa-treated Parkinson’s disease: A randomized placebo-controlled extension of the deprenyl and tocopherol antioxidative therapy of parkinsonism trialAnn Neurol2002516041212112107
- ShultsCWOakesDKieburtzKEffects of coenzyme q10 in early Parkinson disease: evidence of slowing of the functional declineArch Neurol20025915415012374491
- SimpkinsNJankovicJNeuroprotection in Parkinson’s diseaseArch Int Med20031631650412885679
- StarksteinSEMaybergHSPreziosiTJReliability, validity, and clinical correlates of apathy in Parkinson’s diseaseJ Neuropsychiatry Clin Neurosci1992413491627973
- SteinMBHeuserIJJuncosJLAnxiety disorders in patients with Parkinson’s diseaseAm J Psychiatry1990147217202301664
- SternMBMarekKLFriedmanJDouble-blind, randomized, controlled trial of rasagiline as monotherapy in early Parkinson’s disease patientsMov Disord2004199162315300656
- SternMBDopamine agonists modify the course of Parkinson diseaseArch Neurol20046119697115596624
- StocchiFVaccaLBerardelliADual dopamine agonist treatment in Parkinson’s diseaseJ Neurol2003250822612883924
- StocchiFVaccaLRuggieriSIntermittent vs continuous levodopa administration in patients with advanced Parkinson disease: a clinical and pharmacokinetic studyArch Neurol2005629051015956161
- StoverNPBakayRASubramanianTIntrastriatal implantation of human retinal pigment epithelial cells attached to microcarriers in advanced Parkinson diseaseArch Neurol20056218337a16344341
- StoverNPOkunMSEvattMLStimulation of the subthalamic nucleus in a patient with Parkinson disease and essential tremorArch Neurol2005621413b15642861
- TakeshitaSKurisuKTropLEffect of subthalamic stimulation on mood state in Parkinson’s disease: evaluation of previous facts and problemsNeurosurg Rev2005281798615827764
- TanEKOndoWClinical characteristics of pramipexole-induced peripheral edemaArch Neurol2000577293210815140
- TandbergELarsenJPAarslandDThe occurrence of depression in Parkinson’s disease. A community-based studyArch Neurol19965417598639068
- TintnerRManianPGauthierPPleuropulmonary fibrosis after long-term treatment with the dopamine agonist pergolide for Parkinson diseaseArch Neurol2005621290516087771
- VazquezAJimenez-JimenezFJGarcia-RuizP“Panic attacks” in Parkinson’s disease: a long-term complication of levodopa therapyActa Neurol Scand1993871488424307
- Verhagen MetmanLDottoPDLePooleKAmantadine for levodopa-induced dyskinesias. A 1-year follow up studyArch Neurol1999561383610555659
- Verhagen MetmanLKonitsiotisSChaseTNPathophysiology of motor response complications in Parkinson’s disease: Hypotheses on the why, where, and whatMov Disord2000153810634235
- VoonVThomsenTMiyasakiJMFactors associated with dopaminergic drug-related pathological gambling in Parkinson diseaseArch Neurol200764212617296836
- VoonVRepetition, repetition and repletion: compulsion and punding behaviors in Parkinson’s diseaseMov Disord2004193677015077233
- WattsRLJankovicJWatersCRandomized, blind, controlled trial of transdermal rotigotine in early Parkinson diseaseNeurology200768272617202432
- WattsRLRaiserCDStoverNPStereotaxic intrastriatal implantation of human retinal pigment epithelial (hRPE) cells attached to gelatin microcarriers: a potential new cell therapy for Parkinson’s diseaseJ Neural Transm Suppl2003652152712946059
- WeinerWJFactorSAJankovicJThe long-term safety and efficacy of pramipexole in advanced Parkinson’s diseaseParkinsonism Relat Disord200171152011248592
- WeinerWJInitial treatment of Parkinson disease: levodopa or dopamine agonistsArch Neurol2004611966915596623
- WeintraubDSternWBIntervening in the neuropsychiatric features of Parkinson’s diseaseExpert Rev Neurother2007769971017563252
- WhoneALWattsRLStoesslAJSlower progression of Parkinson’s disease with ropinirole versus levodopa: The REAL-PET studyAnn Neurol2003549310112838524
- WilkinsonDGPassmoreAPBullockRA multinational, randomised, 12-week, comparative study of donepezil and rivastigmine in patients with mild to moderate Alzheimer’s diseaseInt J Clin Pract200256441612166542
- Williams-GrayCHFoltynieTLewisSJGCognitive deficits and psychosis in Parkinson’s disease: A review of Pathophysiology and therapeutic optionsCNS Drugs20062047750516734499
- WolozinBWangSWLiNCSimvastatin is associated with a reduced incidence of dementia and Parkinson’s diseaseBMC Med200719520
- ZanettiniRAntoniniAGattoGValvular heart disease and the use of dopamine agonists for Parkinson’s diseaseNew Eng J Med2007356394617202454
- ZesiewiczTAGoldMChariGThe occurrence of depression in Parkinson’s diseaseArch Neurol1999531759
- ZhangSMHernanMAChenHIntakes of vitamins E and C, carotenoids, vitamin supplements, and PD riskNeurology2002591161912391343
- ZouLJankovicJRoweDBNeuroprotection by pramipexole against dopamine- and levodopa-induced cytotoxicityLife Sci19996412758510227583