Abstract
Purpose:
To investigate multifocal visual evoked potentials (mfVEP) of the amblyopic and fellow eye in amblyopia due to anisometropia.
Methods:
We recorded mfVEP in both eyes of 15 anisometropic amblyopic patients and 15 normal control subjects. The responses from the central 7.0° arc of the visual field were measured, and changes in latency and amplitude were compared between the amblyopic, fellow, and normal control eyes.
Results:
There was a significant difference in the latency and amplitude of mfVEP between the amblyopic and fellow eyes. The responses in the central region of the visual field (rings 1 and 2) had a longer latency and smaller amplitude in the amblyopic eye. In contrast, there was no difference in mfVEP latency or amplitude between the fellow eye and normal control eyes.
Conclusion:
These results suggest that mfVEP may be used as an alternative objective method for diagnosis and monitoring of anisometropic amblyopia.
Introduction
Amblyopia is a developmental loss of visual sensitivity caused by experience of discordant binocular images early in life, and refers to a decrease in best corrected visual acuity of an eye with no organic pathology.Citation1 Despite many interesting theories and neurophysiologic investigations in animal models, it is not clearly understood how and where in the visual system the visual connections that result in amblyopia are altered.Citation2–Citation4 Amblyopia is primarily a cortical phenomenon, caused by unequal competitive input from the two eyes into area 17 of the primary visual cortex. However, additional structural and functional abnormalities have also been observed in the lateral geniculate body of animals and humans.Citation1,Citation2,Citation5,Citation6
A number of studies have indicated that the conventional visual evoked responses in these cases are abnormal.Citation3,Citation5,Citation6 These abnormalities in visual evoked potentials (VEP) are related to loss of high spatial frequency contrast sensitivity, and can be marked in anisometropic amblyopic patients. It has also been shown that the decrease in visual acuity for amblyopic eyes is greater in the fovea than at the periphery of the visual field, and the contrast sensitivity for a fixed spatial frequency across the visual field of amblyopic patients shows a greater depression in the fovea than peripherally.Citation7,Citation8 Recently, multifocal VEP (mfVEP) have been used widely to investigate pathologic changes or functional variations in the visual system.Citation9–Citation11 Using this technique, numerous locations in the visual fields can be stimulated simultaneously, and individual responses from each of them can be extracted.
In this study, we measured the mfVEP across the foveal and parafoveal area in each eye of anisometropic amblyopic patients and compared the differences between the amblyopic eye, fellow eye, and normal control eyes.
Materials and methods
Fifteen patients aged 6–10 years (mean 7.66 ± standard deviation [SD] 1.44) with amblyopia due to anisometropia were examined in the Department of Ophthalmology at the University of Athens. In all of the amblyopic eyes examined, the cornea and lens were clear, and no retinal or optic nerve diseases which might influence mfVEP values were observed. Also, there was no nystagmus or latent nystagmus. Amblyopia was diagnosed on the basis of a clear history after the age of 5 years and on orthoptic examination revealing foveal fixation without strabismus or microtropia. Refractive errors were corrected before testing. Age, refraction, and best corrected visual acuity of the subjects are shown in . In the normal control subjects, the age was 10–15 years, the spherical or astigmatic error was less than 1.0 diopter, and best corrected visual acuity was 6/6. The research followed the tenets of the Declaration of Helsinki and informed consent was obtained from the parents of the patients after the nature of the study was explained.
Table 1 Clinical data for studied subjects
Recording of multifocal visual evoked potentials
We used theVERIS system 4.2 (Visual Evoked Response Imaging System 4.2, Electro-Diagnostic Imaging, San Francisco, CA) to record the mfVEP. The stimulus array consisted of 60 sectors, each with 16 checks, comprising 8 black and 8 white. The stimulus array was scaled and displayed on a monochrome monitor driven at 75 Hz. The luminance of the white checks was 200 cd/m2 and for the black checks was 3 cd/m2, producing a contrast of 97%. The background luminance of the screen was 100 cd/m2. The diameter of the first stimulus ring was 0.5–3.0° of arc, 3.0–7.0° for the second stimulus ring, and 7.0–12.0° for the third stimulus ring. To obtain mfVEP, the signals were fed into an amplifier and band-pass filtered at 3–100 Hz. The gain of the amplifier was × 100,000.
For signal derivation, the active electrode was placed 2 cm above the inion and the reference electrode was placed 2 cm below the inion. A ground electrode was attached to the center of the forehead. The fellow eye was closed and the total recording time was 8 minutes.
Subjects viewed with appropriate refractive correction and were instructed to maintain fixation at the center of the stimulus marked with an “X”. The mfVEP waveforms were divided into five groups, from the center to the periphery, according to their different eccentricities. Because the intersubject and intrasubject variance of traces of the outermost rings was very large, only data from rings 1 and 2 were analyzed.
Statistical analysis
Continuous data were tested using the Kolmogorov and Smirnov method to determine whether they followed a Gaussian distribution. The data sampled from the Gaussian distribution were compared using the unpaired t-test. Categoric data were tabulated and compared using the Chi-square test. A P value less than 0.05 was considered to indicate statistical significance.
Results
All patients were diagnosed with hypermetropia or hypermetropic astigmatism, except for one case (Case 9) who suffered from myopia (). The fellow eye was hypermetropic or emmetropic. The anisometropia was higher than 4 diopters between the amblyopic and fellow eye. Also, there was no significant difference in visual acuity between the fellow and normal control eyes.
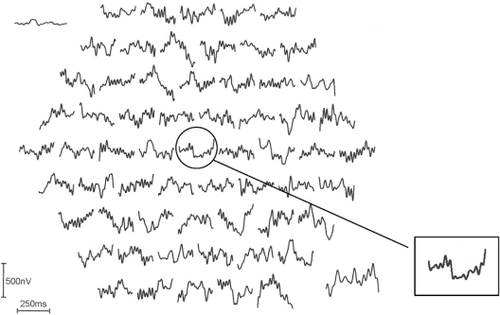
shows a monocular pattern reversal mfVEP recorded from the fellow eye of an amblyopic patient (Case 9 in ). The inset shows a typical normal single foveal response. shows a monocular pattern reversal mfVEP recorded from the amblyopic eye of the same patient. The amplitude of the center stimulus hexagon (ring 1) is attenuated compared with the trace of the fellow eye and traces adjacent to it.
Figure 1 Pattern reversal multifocal visual evoked potentials recorded from the fellow left eye of Case 10 in . The inset shows a normal foveal trace without attenuation and normal latency.
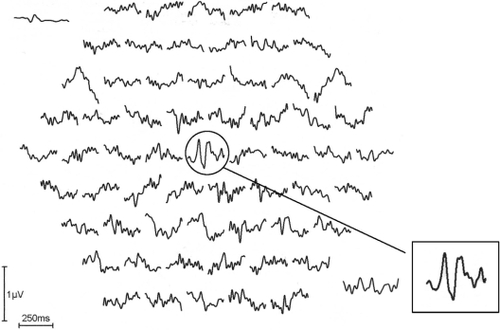
Figure 2 The multifocal visual evoked potentials recorded from the amblyopic right eye of the same subject in . The inset shows the pathologic foveal trace with decreased amplitude and increased latency.
shows the amplitude and latency in ring 1 and 2 of the mfVEP in the amblyopic, fellow, and normal control eyes.
Table 2 Values of multifocal visual evoked potentials for rings 1 and 2 in amblyopic, fellow, and normal control eyes
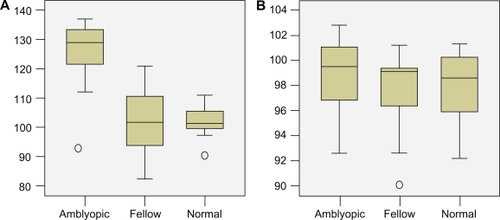
shows that the mean amplitude of mfVEP from the foveal area (ring 1) in the amblyopic eye was 17.5 μV/deg2 (SD ± 7.5), and the mean latency was 127.1 msec (SD ± 7.7). In the parafoveal area (ring 2), the mean amplitude was 6.9 μV/deg2 (SD ± 1.88) and the mean latency was 98.7 msec (SD ± 2.96). In the fellow eye, the mean amplitude of mfVEP in the foveal area (ring 1) was 50.75 μV/deg2 (SD ± 7.78) and the mean latency was 101.66 msec (SD ± 12.04). In the parafoveal area (ring 2), the mean amplitude was 8.4 μV/deg2 and the mean latency was 96.6 msec (SD ± 1.64).
The Kolmogorov and Smirnov method assumed that the data for both groups followed Gaussian distributions. The statistical analysis performed by using the unpaired t-test demonstrated that the retinal response density of ring 1 was significantly lower in the amblyopic eye (P < 0.0001). Conversely, the decrease in the parafoveal area (ring 2) was not statistically significant (P = 0.0333, ). The mean latency in the amblyopic eye was significantly higher in ring 1 than in the fellow eye (P < 0.0001). Conversely, the difference between the amblyopic and fellow eye in ring 2 was lower but not significantly so (P = 0.3175, ). Finally, there was no statistical difference in the values of multifocal electroretinography between the fellow and normal control eyes.
Figure 3 Box plots of data showing the difference of mean amplitude of multifocal visual evoked potentials in ring 1 (A) and ring 2 (B) in the amblyopic, fellow, and normal control eyes.
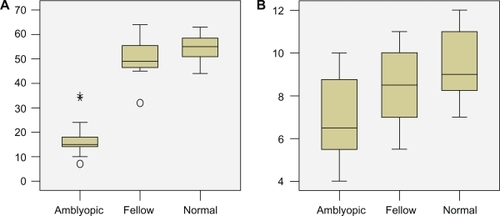
Figure 4 Box plots of data showing the difference of mean latency of multifocal visual evoked potentials in ring 1 (A) and ring 2 (B) in the amblyopic, fellow, and normal control eyes.
Discussion
In our study, the results from the mfVEP recordings concur with data showing impairment of vision in amblyopia due to anisometropia. We also demonstrated that the multifocal responses to a 7° stimulation in amblyopic eyes were severely depressed within the foveal and parafoveal areas compared with the fellow eyes. These differences in amplitude, as well as in latency, were statistically significant, especially within ring 1, which represents the foveal area. In contrast, there was no significant difference in response amplitude and latency between the fellow and normal control eyes.
Many previous studies have demonstrated that the latency and amplitude of pattern VEP, obtained by using large stimulating fields, are abnormal in amblyopia.Citation12–Citation14 However, these data do not show how the increase of latency and attenuation of amplitude vary with eccentricity in amblyopia. Our results show that the increase in latency and decrease of P1-N2 amplitude is more marked at the foveal region and is diminished in the parafoveal area. This is consistent with the results of Levi et alCitation8 and Yu et alCitation11 who demonstrated that visual acuity was more severely impaired in the foveal area than in the periphery of amblyopic eyes. A possible explanation of this phenomenon is that the center of the visual field in the normal eye has keen visual acuity and its development demands are an accurately focused image, whereas the periphery of the visual field has poorer visual acuity and requires a less accurate focus of the image.Citation11 However, recent studies suggest that the observed mfVEP deficits of amblyopic eyes may be largely attributed to their unsteady fixation.Citation15
Some studies have focused attention on the anatomic location of the VEP abnormalities. Shan et alCitation16 suggested that anisometropic amblyopia is primarily associated with an abnormal parvocellular visual system rather than function of the magnocellular visual system, which is why the dorsal layers of the lateral geniculate body are the most abnormal.Citation17 Parvocellular pathways tend to reflect visual function of the fovea, and account for the relatively greater defects observed in central than peripheral visual function in amblyopic individuals.Citation18 This may explain why mfVEP are more attenuated in the central region of the visual field, with less of an effect at the periphery.Citation13,Citation16
In summary, we suggest that assessment of mfVEP may enable objective and quantitative identification of depression of visual function in anisometropic amblyopia and that this may help to provide a more accurate diagnosis in ophthalmic practice.
Disclosure
The authors report no conflict on interest in this work.
References
- von NoordenGKBinocular Vision and Ocular Motility6th edSaint Louis, MOMosby2002
- ArdenGBBarnardWMMushinASVisually evoked responses in amblyopiaBr J Ophthalmol1974581831924600341
- KiorpesLVisual processing in amblyopia: Animal studiesStrabismus20061431016513565
- HoytCSNickelBLNilsonFAOphthalmological examination of the infant. Developmental aspectsSurv Ophthalmol1982261771897041306
- SokolSAbnormal evoked potentials in amblyopiaBr J Ophthalmol1983673103146838802
- DavisETBassSJShermanJFlash visual evoked potential (VEP) in amblyopia and optic nerve diseaseOptom Vis Sci1995726126188532302
- KirschenDGFlomMCVisual acuity at different retinal loci of eccentrically fixating functional amblyopiaAm J Optom Physiol Opt197855144150677256
- LeviDMKleinSAAitsebaomoAPDetection and discrimination of the direction of the motion in central and peripheral vision of normal and amblyopic observersVision Res1984247898006474836
- HoodDCOdelJGWinnBJThe multifocal visual evoked potentialJ Neuroophthalmol200323270289
- ZhangWZhaoKMultifocal VEP difference between early- and late-onset strabismus amblyopiaDoc Ophthalmol200511017318016328925
- YuMBrownBEdwardsMHInvestigation of multifocal visual evoked potentials in anisometropic and esotropic amblyopesInvest Ophthalmol Vis Sci199839203320409761281
- SokolSPattern visual evoked potentials. Their use in pediatric ophthalmologySokolSElectrophysiology and Psychophysics: Their Use in Ophthalmic DiagnosisBoston, MALittle, Brown & Co1980
- WagnerPNilssonBYVisual evoked responses to pattern-reversal stimulation in patients with amblyopia and/or defective binocular functionsActa Ophthalmol197856617627735770
- WagnerPPerssonHEVisual evoked responses to pattern-reversal stimulation in childhood amblyopiaActa Ophthalmol1980586977067211258
- ZhangBStevensonSSChengHEffects of fixation instability on multifocal VEP (mfVEP) responses in amblyopesJ Vis200816114
- ShanYMosterMLRoemerRAAbnormal function of the parvocellular visual cells in amblyopiaJ Pediatr Ophthalmol Strabismus200037737810779264
- MaguireGWSmithELHarwerthRSCrawfordMLOptically induced anisometropia in kittensInvest Ophthalmol Vis Sci198223263264
- DonahueSPThe relationship between anisometropia, patient age and the development of amblyopiaTrans Am Ophthalmol Soc200510331331617057809