Abstract
Idiopathic intracranial hypertension (IIH) in pregnancy is often responsive to conservative management and usually carries a favorable prognosis. Pregnant patients may be managed with dietary control, corticosteroid therapy, diuretics, and occasionally serial lumbar puncture. We report an unusual case of permanent visual loss due to IIH in pregnancy, requiring aggressive CSF diversion and bilateral optic nerve sheath fenestration after failure to improve with a brief course of medical management and a lumbar puncture. Despite resolution of the papilledema, the subject’s acuity improved only to 20/40 in the right eye and remained no light perception in the left eye.
Introduction
Idiopathic intracranial hypertension (IIH) in pregnancy is often responsive to conservative management and usually carries a favorable prognosis. Pregnant patients may be managed with dietary control, corticosteroid therapy, diuretics, and occasionally serial lumbar puncture. The following case represents an unusual report of permanent visual loss due to IIH in pregnancy, which required aggressive cerebrospinal fluid diversion and bilateral optic nerve sheath fenestration.
Methods
Retrospective chart, radiographic, and photographic review.
Case report
A 22 year-old African American (G6P2, no spontaneous fetal loss) with a 13 week intrauterine pregnancy was transferred to our facility for further management of IIH. During her uncomplicated pregnancy, the patient gained approximately two pounds from a prepartum weight of 155 lbs. (prepartum body mass index = 28). The past medical history was otherwise unremarkable. A sister had systemic lupus erythematos. The patient took an oral contraceptive for six months prior to the pregnancy, and a daily prenatal vitamin during the pregnancy.
At gestational week 12, she presented to a local emergency department with complaints of headache and blurred vision for approximately one day. She was treated with acetaminophen/hydrocodone over the next six days. Despite treatment, the patient developed worsening headache and blurred vision, photophobia, dizziness, nausea, vomiting, and muscle stiffness and spasm in the neck and trapezius. She remained afebrile throughout her entire course. Her visual acuity at that time was reported as 20/100 in the right eye and light perception in the left eye. A computed tomographic (CT) scan without contrast and magnetic resonance venography (MRV), were both normal. She underwent a lumbar puncture in the lateral recumbent position with an opening pressure of 460 mmH2O. Cerebrospinal fluid (CSF) studies, including cytology, Gram stain, culture, cryptococcus antigen, and stain for acid-fast bacilli, were normal (protein = 32; glucose = 69; leukocytes = 2; 92% lymphocytes; red blood cells [RBC] = 1). The patient was treated with 250 mg intravenous methylprednisolone succinate every six hours and ceftriaxone. Other hematological values at that time included hemoglobin of 12.6 gram/deciliter, hematocrit of 36.4%, leukocyte count of 10.4 × 10−9/liter (L) and a platelet count of 274 × 10−9/L. A serum rapid plasma reagin was nonreactive.
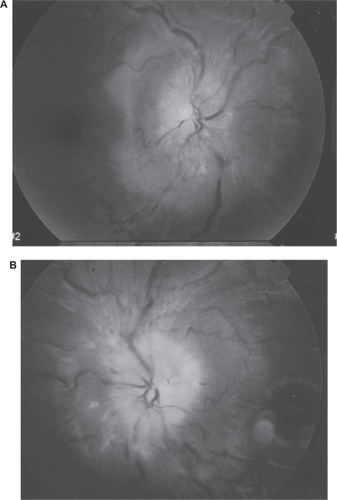
The patient was transferred to our facility for further management. Best corrected visual acuities were 20/100 in the right eye and no light perception (NLP) in the left eye. The patient correctly identified 10/10 Ishihara color plates with the right eye. The left pupil failed to react to light, although the efferent response was intact. Humphrey 24-2 fastpac visual field testing of the right eye revealed a mean deviation of −16.1. There was an enlarged blind spot, dense nasal depression, and peripheral constriction (). Extraocular movements were full, and the patient was orthophoric by Hirschberg testing. Slit lamp examination was noncontributory. Dilated funduscopic examination revealed moderately severe, bilateral papilledema without evidence of vitritis or other retinal disturbances ().
Figure 1 Humphrey 24-2 visual field testing with mean deviation of −16.1; right eye.
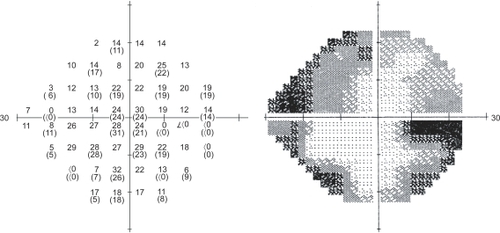
Figure 2 Severe disc edema, splinter hemorrhage, venous tortuosity, nerve fiber layer opacification and cotton-wool spots; A, right eye; B, left eye.
The patient was admitted to the high-risk obstetrics service with the diagnosis of IIH. Review of previous imaging studies (CT, MRV), and a subsequent high quality magnetic resonance image of the brain and orbits with fat suppression and contrast at our facility, revealed no abnormalities. Specifically, there was no hydrocephalus, mass lesion, meningeal or optic nerve enhancement. Her systolic blood pressure ranged from 104 to 137 mm of mercury (mmHg) and the diastolic from 55 to 60 mmHg.
Additional studies included: Westergren erythrocyte sedimentation rate (ESR) = 62 mm/hour (hr); normal thyroid function panel; protein C = 175 (normal range: 60–140); activated partial thromboplastin time = 23.7 seconds, and an equivocal Lyme screen. Relevant coagulation measures, including homocysteine level, protein S activity, Dilute Russel viper venom, and anticardiolipin IgG and IgM, were all normal. C-reactive protein and antinuclear antibody were normal. In addition, the patient had negative serologies for human immunodeficiency virus and hepatitis C. A tuberculosis skin test was negative. A hemoglobin electrophoresis was normal.
The patient received a gram of methylprednisolone succinate per day in divided doses. One day after admission, she underwent a bilateral ONSF and concurrent placement of a lumbar drain (5 ml/hr). Microscopic evaluation of specimens of the right and left optic nerve sheaths was normal. Gram stain and culture of the CSF bag specimen obtained during drainage were unremarkable, and repeated analysis revealed only rare lymphocytes, 31 RBC, and normal protein and glucose levels. The CSF VDRL was negative. The lumbar drain was removed on post-operative day three and the patient was discharged home on post-operative day four on 60 mg of prednisone.
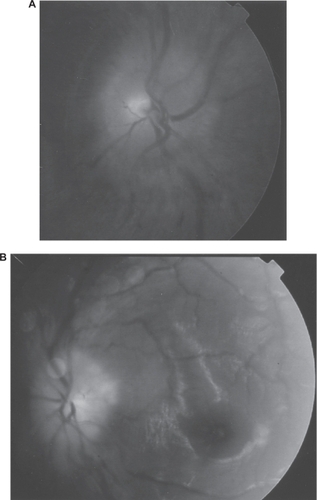
In follow-up, the visual acuity in the right eye improved to 20/40 and remained NLP in the left eye. The patient’s funduscopic examination showed resolution of disc edema but pallor developed bilaterally ().
Figure 3 Significant decrease of papilledema three days following ONSF and placement of lumbar drain; A, right eye; B, left eye.
Discussion
The patient’s course and tempo of visual loss is unusual for IIH. Extensive hematological, serologic, and structural evaluation for other causes of elevated intracranial pressure was unrevealing. Specifically, there was no evidence of meningitis, inflammatory optic neuropathy nor venous sinus thrombosis. Three laboratory abnormalities deserve further discussion. An elevated ESR was felt to be secondary to pregnancy rather than due to a primary inflammatory or viral process. A recent study by Citationvan den Broe and colleagues (2001) concluded that ESR ranges for pregnant patients vary with gestational age and hemoglobin level. For anemic patients in the first half of pregnancy, ESR is expected to be in the range of 40 to 95 mm per hour. Thus, the ESR was within normal limits for the patient’s stage of pregnancy. Secondly, according to a prospective study by CitationOruc and colleagues (2000), Protein C and Protein S anti-coagulant proteins typically decrease during a normal pregnancy on a dilutional basis. It is possible that the modest elevation in protein C in this case represents an acute phase response. Finally, the equivocal Lyme testing did not meet the Center for Disease Control and Prevention criteria for the diagnosis of Lyme disease.
More than 70 cases (CitationNickerson and Kirk 1965; CitationElian et al 1968; CitationPowell 1972; CitationCaroscio and Pellmar 1978; CitationShekleton et al 1980; CitationAnderson 1983; CitationKassam et al 1983; CitationKoontz et al 1983; CitationDigre et al 1984; CitationPeterson and Kelly 1985; CitationKatz et al 1989; CitationShapiro et al 1995; CitationEvans and Friedman 2000; CitationHuna-Baron and Kupersmith 2001) of IIH during pregnancy are reported in the English language since 1960. A review of these reports revealed no case of blindness and only a handful of reported cases of permanent visual field loss (CitationNickerson and Kirk 1965; CitationPowell 1972; CitationShekleton et al 1980; CitationShapiro et al 1995). Our patient was unique in that she not only experienced permanent loss of visual acuity and visual field, but the onset and magnitude of loss was both rapid and extreme. This type of clinical progression of IIH in pregnancy is not typically reported. Furthermore, based on the cases presented in the literature, IIH in pregnancy is often responsive to conservative management with diet, bed rest, steroids, diuretics or lumbar puncture(s) (CitationNickerson and Kirk 1965; CitationPowell 1972; CitationCaroscio and Pellmar 1978; CitationAlderson 1983; CitationKassam et al 1983; CitationKoontz et al 1983; CitationDigre et al 1984; CitationPeterson and Kelly 1985; CitationKatz et al 1989; CitationHuna-Baron and Kupersmith 2001). Only a minority of cases requires aggressive therapy involving surgical intervention. In our case, conservative medical management failed and carbonic anhydrase inhibitors were not used because of their relative contraindication in pregnancy (category C: animal studies show adverse fetal effects[s]; no controlled human studies). Thus, rapid surgical intervention was needed to halt the progressive visual loss and probably contributed to ultimate improvement in visual acuity and field in the right eye.
Disclosure
This work is supported, in part, by an unrestricted Grant from Research to Prevent Blindness, Inc., New York, NY; Fund for the New Jersey Blind, Newark, NJ; Lions Eye Research Foundation of New Jersey, Newark, NJ; The Eye Institute of New Jersey, Newark, NJ; and the Gene C. Coppa Memorial Fund.
References
- AldersonTL1983Nonrecurrent pseudotumor cerebri in pregnancy: report of caseJ Am Osteopath Assoc82728316863052
- CaroscioJTPellmarM1978Pseudotumor cerebri: occurrence during the third trimester of pregnancyMt Sinai J Med4553941309079
- DigreKBVarnerMWCorbettJJ1984Pseudotumor cerebri and pregnancyNeurology3472196539432
- ElianMBen-TovimNBecharM1968Recurrent benign intracranial hypertension (pseudotumor cerebri) during pregnancyObstet Gynecol3168585646400
- EvansRWFriedmanDI2000The management of pseudotumor cerebri during pregnancyHeadache40495710849049
- Huna-BaronRKupersmithMJ2001Idiopathic intracranial hypertension in pregnancyJ Neurol24910788112195458
- KassamSHHadiHAFadelHE1983Benign intracranial hypertension in pregnancy: current diagnostic and therapeutic approachObstet Gynecol Surv38314216346167
- KatzVLPetersonRCefaloRC1989Pseudotumor cerebri and pregnancyAm J Perinatol644252789543
- KoontzWLHerbertWNPCefaloRC1983Pseudotumor cerebri in pregnancyObstet Gynecol6232476877689
- NickersonCWKirkRF1965Recurrent pseudotumor cerebri in pregnancy. Report of 2 casesObstet Gynecol26811135849290
- OrucSSarucMKoyuncuFM2000Changes in the plasma activities of protein C and protein S during pregnancyAust N Z J Obstet Gynaecol404485011194434
- PetersonCMKellyJV1985Pseudotumor cerebri in pregnancy. Case reports and review of literatureObstet Gynecol Surv4032394000567
- PowellJL1972Pseudotumor cerebi and pregnancyObstet Gynecol40713185083223
- ShapiroSYeeRBrownH1995Surgical management of pseudotumor cerebri in pregnancy: case reportNeurosurgery37829318559316
- ShekletonPFidlerJGrimwadeJ1980A case of benign intracranial hypertension in pregnancyBJOG873457
- van den BroeNRLetskyEA2001Pregnancy and the erythrocyte sedimentation rateBJOG1081164711762656