Abstract
The nomenclature of each part of the lacrimal canaliculus, for example the vertical portion, does not always reflect the true course. Since we have sometimes observed findings suggesting the so called vertical portion of the lower lacrimal canaliculus inclined laterally, we re-examined the course of the vertical portion. Twenty-eight postmortem lower eyelids in 16 Japanese were examined and divided into 2 groups. The first group was 14 lower eyelids of 7 cadavers. Eyelids were incised sagittally from the lower lacrimal punctum. The second group was 14 lower eyelids of 9 cadavers; these were incised from the lower lacrimal punctum with 5 degrees lateral inclination to the sagittal plane. In the first group, 10 canaliculi of 7 cadavers were interrupted at the halfway point of the vertical portion. Four canaliculi of 4 cadavers included the whole length of the vertical portion. In the second group, all specimens included the whole length of the vertical portion. Most vertical portions of the lower lacrimal canaliculus demonstrated a laterally inclined course of approximately 5 degrees, although some took a completely vertical course.
The lacrimal canaliculus consists of vertical and horizontal portions and the common canaliculus (CitationDoxanas and Anderson 1984). The vertical portion, into which the puncta leads, is the initial part of the canaliculus (CitationWhitnall 1979; CitationDoxanas and Anderson 1984; CitationHwang et al 2005). At the base of this vertical portion, the canaliculus dilates and forms a receptacle for the collection of tears, called the “ampulla” (CitationWhitnall 1979; CitationDoxanas and Anderson 1984). The canaliculus then turns horizontally in a medial direction along the eyelid margin (CitationWhitnall 1979; CitationDoxanas and Anderson 1984; CitationBedrossian 2002). The horizontal portions of the upper and lower canaliculi unite before entering the lacrimal sac as the common canaliculus, or internal common punctum; however, approximately 10 percent of cases show separate openings to the lacrimal sac (CitationBedrossian 2002). The lateral 5/6 of the canaliculi, including the vertical portion, is covered by the muscle of Riolan or Horner’s muscle (CitationWhitnall 1979; CitationKakizaki et al 2005, Citation2007).
Although the anatomy of the lacrimal canaliculus is generally understood as above, the nomenclature does not always reflect the true course. The vertical portion is directed slightly anteriorly (CitationBedrossian 2002). As well, occasionally there are further recesses in the ampulla directed in the opposite direction, that is, laterally (CitationWhitnall 1979). The horizontal portion, as it courses medially, inclines towards its equivalent in the opposite eyelid (CitationWhitnall 1979).
We speculated that the vertical portion of the lower lacrimal canaliculus inclines laterally, based on our observations. First, when we removed a lower eyelid tumor with a full thickness skin excision, regardless of the complete vertical incision outside the lower lacrimal punctum, we came across the vertical portion of the lower lacrimal canaliculus. Second, when the insertion of a lacrimal probe into a lower lacrimal punctum was not so easy to perform, a lateral inclination of a probe could ease its insertion.
In the present study, we used cadavers to examine whether the vertical portion of the lower lacrimal canaliculus inclined, by observing from the lateral direction.
Materials and methods
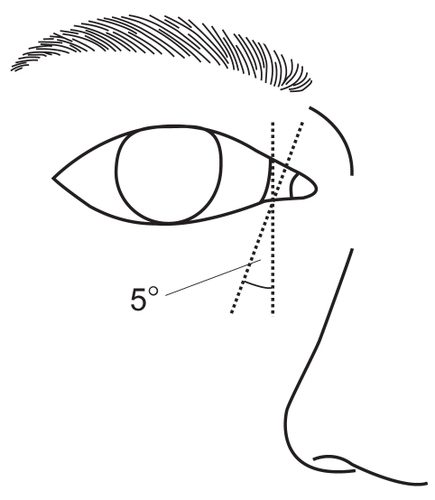
Twenty-eight post mortem lower eyelids (14 right, 14 left) from 16 Japanese cadavers were examined and divided into 2 groups. One group of 14 lower eyelids of 7 cadavers (7 right, 7 left; 3 males, 4 females) with an average age at death of 80.4 years (range: 73~97), were sagittally incised from the lower lacrimal punctum (). The other 14 lower eyelids of 9 cadavers (7 right, 7 left; 4 males, 5 females) with an average age at death of 76.3 years (range: 69~95) were incised from the lower lacrimal punctum with 5 degrees lateral inclination to the sagittal plane ().
Figure 1 Diagram of the incisional lines. One incision is done sagittally from the lower lacrimal punctum; the other is done at 5 degrees lateral inclination to the sagittal plane.
All specimens were fixed with 10% buffered formalin before use. All cadavers were registered in the cadaveric service of Aichi Medical University, with proper consent from our Institutional Review Board and approval to use them for educational purposes and studies. All methods for securing human tissue were humane and complied with the tenets of the Declaration of Helsinki.
We examined whether the vertical portion of the lower lacrimal canaliculus inclined laterally. All medial samples were taken and observed laterally.
Results
In the first group, which underwent a strict sagittal incision, 10 canaliculi of 7 cadavers (6 right, 4 left; male 5 eyelids, female 5 eyelids) were interrupted at the halfway point of the vertical portion and so the distal part of the canaliculi were not included (, ). However, 4 canaliculi of 4 cadavers (1 right, 3 left; male 1 eyelids, female 3 eyelids) did include the whole length of the vertical portion.
Figure 2A With a complete sagittal incision, the vertical portion of the lacrimal canaliculus is interrupted at the halfway point and so the distal part of the canaliculus is not included here.
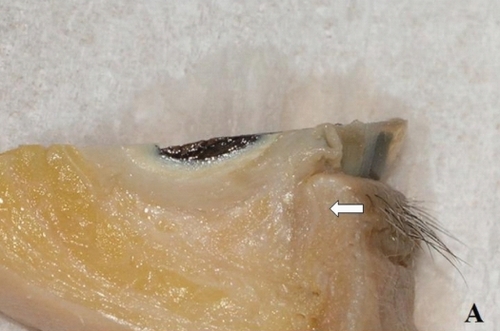
Figure 2B Line diagram of .

In the second group with 5 degrees laterally inclined incision, all specimens included the whole length of the vertical portion (, ).
Figure 3A For an incision at 5 degrees lateral inclination to the sagittal plane, the slice includes the whole length of the vertical portion.
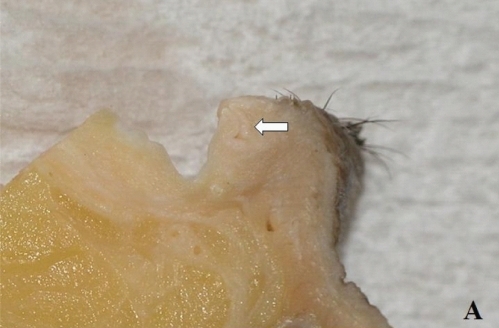
Figure 3B Line diagram of .

Discussion
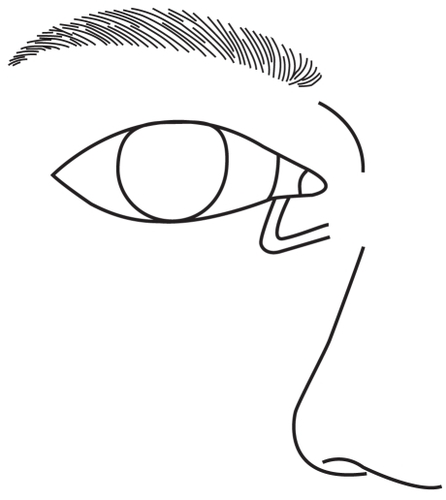
Most vertical portions of the lower lacrimal canaliculus examined here demonstrated a laterally inclined course of approximately 5 degrees (). However, the others took a completely vertical course.
Figure 4 Figure of the laterally inclined course of the vertical lower lacrimal canaliculus.
The course of the laterally directed vertical portion of the lacrimal canaliculus should be considered not only in lacrimal probing, syringing, and trephining but also in eyelid surgeries. The 5 degrees lateral inclination of the vertical portion significantly emphasizes the need of a laterally directed insertion and lateral lid traction during the passage of a lacrimal probe, syringing needle or trephine to accord with the true course of the vertical portion. As well, since the vertical portion takes its lateral course within 1 mm laterally from the lacrimal punctum (CitationWhitnall 1979; CitationHwang et al 2005), surgeons, during eyelid surgery, need to recognize the area within 1 mm laterally from the punctum as being a zone with a potential for serious lacrimal canalicular injury.
This inclination appears advantageous for the lacrimal drainage. In eye closing, the vertical portion changes its direction medially because of the inward eyelid movement (CitationKakizaki et al 2005) caused by the contraction of Horner’s muscle. At this time, the closure of the vertical portion may become insufficient, because the relative angle of the muscle of Riolan and the vertical portion of the lacrimal canaliculus becomes milder. To maintain the relative perpendicular angle to each other, the vertical portion may take a laterally directed position.
Our result can be applied to the living in eye opening. Although all the cadavers were in an eye-closed state, and the muscle tonus of the orbicularis oculi had been completely lost, this state would have been similar to the eye-opening state in live humans whose muscle tonus of the orbicularis oculi is little. As the lacrimal probing syringing and trephining is usually performed in eye-opening state, the present result is reasonable for the true clinical situations.
There are some limitations to our study. First, as the study samples were all taken from elderly cadavers, we may not be able to apply the results to younger generations. Confirming our results in a younger patient population through clinical procedures such as lacrimal probing is possible. Our experience is that the lateral inclination of a probe usually enables easy lacrimal probing, even in young generations. This appears to support the present outcome. Second, as we did not examine samples of Caucasians or Blacks, we cannot conclude that they have the same inclination. However, to date, racial variations have not been reported with regard to the lacrimal drainage system; therefore, we may be able to speculate that they have the same inclination.
In conclusion, most vertical portions of the lower lacrimal canaliculus are directed laterally at approximately 5 degrees. Surgeons need to recognize the true course so as not to cause injury to the vertical portion of the lower lacrimal canaliculus. This understanding should also make lacrimal probing easier. This anatomical view will be helpful for a better understanding of the lacrimal drainage system.
Disclosure
The authors have received no financial support and have no financial or conflict of interest related to this manuscript.
References
- BedrossianEHJrDella RoccaRCBedrossianEHJrArthusBP2002Surgical anatomy of the lacrimal systemOphthalmic Plastic Surgery Decision making and techniquesNew YorkMcGraw-Hill16572
- DoxanasMTAndersonRL1984Clinical Orbital AnatomyBaltimoreWilliams and Wilkins99100
- HwangKKimDJHwangSH2005Anatomy of lower lacrimal canaliculus relative to epicanthoplastyJ Craniofac Surg169495216327537
- KakizakiHZakoMMiyaishiO2005The lacrimal canaliculus and sac bordered by the Horner’s muscle form the functional lacrimal drainage systemOphthalmology1127101615808266
- KakizakiHZakoMMiyaishiO2007Overview of the lacrimal canaliculus in microscopic cross-sectionOrbit26237918097960
- WhitnallSE1979Anatomy of the Human Orbit and Accessory Organs of Vision2nd edNew YorkRobert E Krieger Publishing Company Inc2258