Abstract
Purpose:
This article reviews the effects of the increase in bacterial resistance on the treatment of ocular infections.
Design:
Interpretive assessment.
Methods:
Literature review and interpretation.
Results:
Ocular bacterial infections include conjunctivitis, keratitis, endophthalmitis, blepharitis, orbital cellulitis, and dacryocystitis. Treatment for most ocular bacterial infections is primarily empiric with broad-spectrum antibiotics, which are effective against the most common bacteria associated with these ocular infections. However, the widespread use of broad-spectrum systemic antibiotics has resulted in a global increase in resistance among both Gram-positive and Gram-negative bacteria to a number of the older antibiotics as well as some of the newer fluoroquinolones used to treat ophthalmic infections. Strategies for the prevention of the increase in ocular pathogen resistance should be developed and implemented. In addition, new antimicrobial agents with optimized pharmacokinetic and pharmacodynamic properties that have low toxicity, high efficacy, and reduced potential for the development of resistance are needed.
Conclusions:
New antimicrobial agents that treat ocular infections effectively and have a low potential for the development of resistance could be a part of strategies to prevent the global increase in ocular pathogen resistance.
Introduction
Ophthalmic infections can cause damage to structures of the eye, which can lead to vision loss and even blindness if left untreated.Citation1 The effective use of antibiotics to treat ophthalmic infections requires an understanding of the disease and the pharmacokinetics and pharmacodynamics of the drugs used for the treatment.Citation1,Citation2 The most common ocular infection seen by primary care physicians worldwide is bacterial conjunctivitis, which is self-limiting and largely presents as an acute infection.Citation3,Citation4 Bacterial keratitis, an infection of the cornea often associated with contact lens wear, ocular trauma, or ocular surface disease, is less common but poses a risk of loss of vision.Citation5–Citation8 Endophthalmitis is a rare but potentially sight-threatening infective complication of intraocular surgery (primarily cataract), intravitreal injections, and ocular trauma.Citation9,Citation10 Bacterial blepharitis is an inflammation of the eyelids, particularly at the lid margins, that may be associated with a low-grade staphylococcal bacterial infection.Citation11 Orbital cellulitis and other periorbital infections can be caused by a variety of organisms, including bacteria, and occurs as a complication of surgery, nonsurgical trauma, or the retention of a foreign body.Citation12 Dacryocystitis, or infections of the lacrimal sac, are common at all ages and occur due to acquired or congenital obstruction of nasolacrimal duct.Citation13 Although treatment guidelines for these ocular infections recommend that laboratory culture and smear tests be conducted, when possible, for determination of the causative pathogens,Citation14 in practice the initial choice of antibiotic therapy is generally made without knowing the identity or susceptibility of the ocular pathogen.Citation1,Citation9,Citation15,Citation16 Broad-spectrum antibiotic therapy for bacterial infections is initially used in order to prevent a decline in vision or permanent vision loss that may require surgical intervention.Citation9,Citation16,Citation17 Endophthalmitis, bacterial keratitis, and orbital cellulitis require aggressive initial broad-spectrum antibiotic therapy, which can subsequently be tapered or modified after the results from laboratory culture and smear tests are obtained.Citation18 In this context, it must be noted that most ophthalmic antibiotics are approved for bacterial conjunctivitis only, with few indicated for keratitis and none for endophthalmitis.Citation19
Several therapeutic classes of antibiotic agents are available for ophthalmic indications. These agents differ in their mechanism of action, coverage of important pathogens, and bactericidal versus bacteriostatic effects. The penicillins, cephalosporins, aminoglycosides, and fluoroquinolones are bactericidal agents (ie, kill bacteria)Citation20 and are generally used to treat ocular infections. Bacteriostatic drugs like tetracyclines, macrolides, chloramphenicol, and sulfonamides, which inhibit bacterial growth, are used in cases in which there is a specific benefit or an allergy issue. Antibiotics can be used systemically or topically to control ocular infection. Topically applied antibiotics are more effective in achieving rapid, high concentrations of the antibiotic at the site of infection compared to systemically administered antibiotics. Frequent or inappropriate, systemic long-term use of an antibiotic may result in the development of bacterial antibiotic resistance. Therefore, topical administration of antibiotics may be a better choice, although the occurrence of drug resistance with topical antibiotics used for prolonged periods has been reported.Citation1 Ophthalmic antibiotics are generally formulated as solutions or suspensions, but some are also available as ointments (eg, erythromycin, polymyxin, or bacitracin). Ointments theoretically provide prolonged exposure, since they do not get removed from the site of infection as rapidly as ophthalmic solutions/suspensions do because of rapid tear film turnover.Citation1 However, hydrophilic antibiotics often crystallize within the ointment base, which may impact their release, available concentration, and effectiveness.Citation1 Other factors that affect the exposure of ocular drugs include the integrity of the corneal epithelial barrier, inflammation of the ocular tissues, and the microtoxicity associated with the use of preservatives.Citation1 Thus, the clinician may choose from a number of formulations of agents based on the location and severity of the infection, comorbidities, and the safety and tolerability of the antibiotic as well as bacterial susceptibility.
Rapid use of antibiotics for severe ocular infections is routine in ophthalmic practice, as pathogenesis of ocular bacteria results in release of toxins and degradative enzymes that can damage the integrity of ocular tissues and cause sight-damaging sequelae. Although older ophthalmic antibiotics such as chloramphenicol, sulfonamides, polymyxins, bacitracin, and aminoglycosides and early-generation fluoroquinolones are still prescribed, they are less effective than the advanced-generation fluoroquinolones for treating ocular infections because of a limited spectrum of activity and/or the development of pathogen resistance.Citation21,Citation22 The advanced-generation fluoroquinolones (eg, moxifloxacin and gatifloxacin) have a broader spectrum of activity and are more effective against common ocular pathogens.Citation23
The development of bacterial resistance to specific antibiotics is an important consideration for clinicians treating ocular infections. Bacterial resistance has been emerging worldwide, likely due to widespread and inappropriate dosing of broad-spectrum antibiotics for systemic infections, exacerbated by inadequate compliance to full treatment duration.Citation24 Of note, the Ocular Tracking Resistance in the U.S. Today (TRUST) program, which annually evaluates the in vitro susceptibility of Staphylococcus aureus, Streptococcus pneumoniae, and Haemophilus influenzae to a number of ophthalmic antibiotics in national samples of ocular isolates, reported a 12.1% increase in the incidence of methicillin-resistant S. aureus (MRSA) strains from January 2000 to December 2005, with more than 80% of MRSA resistant to fluoroquinolones.Citation25,Citation26 While these numbers are alarming, one limitation of studies on the emergence of resistance among ocular pathogens is that the determination of bacterial susceptibility to ophthalmic antibiotics is typically based on systemic drug exposure breakpoints, the concentrations at which bacterial isolates are deemed susceptible or resistant to a particular drug.Citation27,Citation28 The data used to determine breakpoints are derived from systemic dosing and the average concentration of drugs in tissues after systemic administration. Since topical administration produces a higher concentration of antibiotic in ocular tissues than that achieved following systemic therapy, these breakpoints, defined by the Clinical and Laboratory Standards Institute (CLSI), do not apply.Citation27 Nevertheless, as discussed later in this review, there are many reports of clinical treatment failure due to ocular pathogen drug resistance. These reports highlight the need to reevaluate and implement improved treatment guidelines for the prevention of pathogen resistance to ocular anti-infective therapies,Citation26,Citation27 and the need to develop new antibiotics with greater efficacy, lower toxicity, and lower resistance potential than older agents.Citation29
Ocular infections and current treatment options
Bacterial conjunctivitis
Bacterial conjunctivitis, or red eye, which involves inflammation of the conjunctival mucosa, is more common in young children and the elderly than in other age groups.Citation3 The etiology of conjunctivitis can be allergic, toxic, or infectious. Symptoms of bacterial conjunctivitis include a purulent discharge around the eye, hyperemia, and a burning or stinging sensation.Citation3,Citation15 The most common causal pathogens in bacterial conjunctivitis are S. aureus, S. pneumoniae, and H. influenzae. Staphylococcus epidermidis, Enterococcus spp., Moraxella spp., streptococci viridans group, Escherichia coli, Serratia marcescens, Pseudomonas aeruginosa, and Proteus mirabilis have also been isolated less frequently from bacterial conjunctivitis samples.Citation3,Citation30,Citation31 Gram-positive pathogens accounted for 52.5% of positive cultures, 72.1% of which were S. aureus ().Citation31 Staphylococci infections are more common in adults, while S. pneumoniae and H. influenzae are more common in children.Citation31
Table 1 Prevalence of most common isolates from patients with bacterial conjunctivitis recovered within the 2-year periodCitation31
Although clinical resolution of bacterial conjunctivitis occurs without any treatment in most patients by 7 days, treatment with broad-spectrum topical antibiotics accelerates the rate of clinical resolution and decreases the risk of contagious spread.Citation4,Citation15,Citation30,Citation32 Topical antibiotics indicated for bacterial conjunctivitis include aminoglycosides (eg, gentamicin and tobramycin), polymyxin-based combinations (eg, polymyxin B sulfate and trimethoprim), azithromycin, fluoroquinolones (eg, ciprofloxacin, levofloxacin, ofloxacin, moxifloxacin, and gatifloxacin), and, outside of the United States, chloramphenicol.Citation4,Citation30
Bacterial keratitis
Bacterial keratitis is a potentially devastating ocular infection that may occur when the corneal epithelial barrier is compromised due to injury or trauma, leading to ulceration and infiltration of inflammatory cells.Citation33 Infection largely involves Gram-positive S. aureus, S. epidermidis, and several Streptococcus and Bacillus spp., as well as Gram-negative bacteria like P. aeruginosa, S. marcescens, Moraxella lacunata, Microbacterium liquefaciens, and H. influenzae. Immediate diagnosis and treatment are important to avoid vision-threatening outcomes, including corneal scarring or perforation.Citation1 Clinical signs and symptoms include mild to severe ocular pain, photophobia, decreased vision, tearing, discharge, inflammation, focal white opacity in the corneal stroma (infiltrate), staining of the area (indicating an epithelial defect), corneal thinning, stromal edema, mild to severe anterior chamber reaction, and eyelid edema.Citation7,Citation8,Citation34 The most common predisposing factors for bacterial keratitis are ocular trauma, contact lens wear (especially extended wear), ocular surface disease, and prior ocular surgery.Citation7,Citation34
Standard treatment of bacterial keratitis is a combination of cefazolin and tobramycin or an aminoglycoside such as gentamicin and a second-generation cephalosporin such as cefuroxime to avoid aminoglycoside retinal toxicity.Citation11 Ciprofloxacin 0.3%, ofloxacin 0.3%, and levofloxacin 1.5% are indicated in the United States for the treatment of corneal ulcer;Citation35–Citation37 monotherapy with fluoroquinolones may now be the preferred treatment, especially if the infection is associated with wearing contact lenses.Citation7 However, the emerging resistance of Gram-positive organisms to older agents and fluoroquinolones has underscored the importance of the clinical practice recommendation to culture all corneal ulcers before antimicrobial treatment.Citation16 Newer fluoroquinolones are therefore recommended for initial therapy of bacterial keratitis to avoid progression of the ocular infection to corneal perforation, endophthalmitis, and even loss of the eye.Citation33
Endophthalmitis
Endophthalmitis is a rare but potentially sight-threatening complication of intraocular surgery, intravitreal injections, and ocular trauma.Citation9,Citation38,Citation39 The incidence of endophthalmitis following cataract surgery has increased over the last decade despite many technical advances and faster visual recovery,Citation40 and ranges from 0.2% to 0.7% in the United States and Europe.Citation10,Citation41,Citation42 The risk for occurrence of endophthalmitis following intravitreal injection of corticosteroids has been estimated to be 0.8% from noninfectious causes and 0.6% to 1.6% from infectious causes.Citation37,Citation43–Citation46 Risk factors for endophthalmitis can be preoperative (blepharitis, lachrymal duct obstruction, contact lens use, and secondary intraocular lens implantation), intraoperative (inadequate eyelid or conjunctival disinfection, surgery lasting for more than 1 hour, loss of vitreous humor, or unplanned ocular penetration) or postoperative (wound abnormalities, inadequately buried sutures, suture removal, and vitreous incarceration in the surgical wound).Citation47 Coagulase-negative Staphylococcus (CoNS) and Bacillus spp. are the most common pathogens of posttraumatic endophthalmitis.Citation48 A postcataract study with 497 patients with endophthalmitis showed that more than 90% of the isolates were Gram-positive, mostly CoNS, and that the in vitro susceptibility profiles of these pathogens had changed over a decade.Citation49 A review of 1182 consecutive open-globe injuries identified 10 patients with culture-proven endophthalmitis. Endophthalmitis-related isolates from these patients included Streptococcus spp. (46.2%), CoNS (23.1%), and Bacillus cereus (15.4%).Citation48
Intravitreal antibiotics including vancomycin and an aminoglycoside or third-generation cephalosporin are used to treat bacterial endophthalmitis, while vitrectomy may be needed for severe cases.Citation9 Since the causal organisms of endophthalmitis may often be the patient’s own conjunctival bacterial flora, many of the routinely used prophylactic measures aim to decrease the number of ocular bacteria before and after surgery.Citation50,Citation51 Prophylaxis for endophthalmitis includes ocular antibiotics and anti-inflammatory agents used in the pre-, peri-, and postoperative period,Citation10,Citation52 as well as intracameral use of cefuroxime at the end of surgery.Citation53 Gatifloxacin and moxifloxacin are routinely administered topically along with the antiseptic povidone-iodine before cataract removal.Citation11,Citation52 Topical moxifloxacin was shown to reduce the incidence of endophthalmitis to less than 0.1% in a retrospective, observational case review of 20,013 patients,Citation50 while intracameral use of cefuroxime at the end of surgery also reduced the occurrence of endophthalmitis to less than 0.1%.Citation53 More than 75% of ophthalmologists in the United States and Europe use preoperative antibiotics, among which the fluoroquinolones have grown increasingly popular.Citation48,Citation54,Citation55 Neither topical antibiotics nor intracameral cefuroxime are indicated for endophthalmitis.
Bacterial blepharitis
Bacterial blepharitis is an infection and inflammation of the eyelid margin associated with hyperemia with crusting on the eyelashes. The most common complications of untreated blepharitis are abnormal eyelash growth (ie, trichiasis), scarring of the eyelids, and injury to the cornea due to constant irritation, which may cause small corneal ulcers.Citation56 The most common causal pathogens for bacterial blepharitis are S. aureus and CoNS.Citation56,Citation57 The standard of care in bacterial blepharitis is antibiotic therapy along with lid scrubs and hot compresses. Ointments of erythromycin, bacitracin, or polymyxin have routinely been used.Citation11 Antibiotic therapy in chronic bacterial blepharitis has to be optimized in order to avoid the development of antibiotic resistance due to long-term antibiotic use.Citation11 In cases where ocular rosacea is a contributing factor to eyelid inflammation in bacterial blepharitis, oral tetracycline, doxycycline, or minocycline is also used.Citation11
Periorbital and orbital cellulitis
Preseptal (periorbital) and postseptal (orbital) cellulitis are potentially vision-threatening bacterial infections of the periocular tissue. While preseptal cellulitis involves only the lid structures and periorbital tissues anterior to the orbital septum, postseptal cellulitis involves tissues behind the septum, and it is seen more commonly in children and adolescents than adults. Routes of infection include trauma, bacteremia, sinusitis, and upper respiratory infections. Signs and symptoms include swelling of the eye, pain, fever, erythema, impaired ocular motility, afferent pupillary defect, proptosis, and visual loss. Sinus radiographs, computed tomography, magnetic resonance imaging, and orbital ultrasonography are used for prognosis. The most common pathogen is H. influenzae. If there is an associated local wound, the pathogens may include S. aureus and Streptococcus pyogenes.Citation58
Traditionally, azithromycin, cephalosporins, penicillins, and clindamycin have been used in oral form to provide broad-spectrum coverage against staphylococci, streptococci, and anaerobes associated with ocular sinusitis (nonviral) and orbital cellulitis.Citation59 Alternatively, vancomycin or other intravenous antibiotics may be used.Citation58,Citation59 Optic nerve function is monitored every 4 hours (through pupillary reactions, visual acuity, color vision, and light brightness appreciation). Treatment, which may be modified according to laboratory results, typically lasts 7 to 10 days.Citation58 Surgery is indicated if there is a lack of response to antibiotic treatment or other complications occur.Citation1
Dacryocystitis
Dacryocystitis is a painful inflammation of the lacrimal sac resulting from congenital or acquired obstruction of the nasolacrimal duct. In adults, it is idiopathic or the result of an obstruction from infection, trauma, or dacryolith, or rarely a neoplasm.Citation60 In dacryocystitis, the medial lower lid location is protruding, tender, and painful, with discharge and tearing. The most common isolates in dacryocystitis are P. aeruginosa, S. aureus, Enterobacter aerogenes, Citrobacter, S. pneumoniae, E. coli, and Enterococcus spp.Citation61,Citation62 Treatment of dacryocystitis includes hot packs with topical and systemic antibiotics to cover penicillinase-producing staphylococcal organisms.Citation6 Clearing the drainage system, along with treatment with parenteral and topical antibiotics until the infection clears, is the standard therapy for dacryocystitis.Citation1 Topical antibiotic treatment includes ceftazidime, ciprofloxacin, and cefuroxime.Citation62 A higher incidence of Gram-negative organisms, particularly Pseudomonas, may indicate a trend in dacryocystitis infections towards antibiotic resistance.Citation62 It is important to modify the antibiotic therapy based on a patient’s response, laboratory culture, and sensitivity results to avoid the development of drug-resistant chronic dacryocystitis.
Bacterial resistance in ocular infections
The emerging resistance of ocular pathogens to topical antimicrobial agents is a worldwide problem. The emergence of bacterial resistance is influenced by characteristics of the pathogens, antibiotic-prescribing practices including the widespread use of systemic antibiotics, and health care guidelines.Citation63 Data from the worldwide surveillance programs TRUST, GLOBAL, PROTEKT, ARM, SENTRY, ABC, and TSNCitation64–Citation69 document widespread resistance among the pathogens commonly responsible for systemic infections to many systemically administered antimicrobial agents.Citation63,Citation70,Citation71 Worldwide, S. pneumoniae has a 20% to 30% resistance rate to penicillin and a 25% to 35% resistance rate to macrolides and azalides.Citation72,Citation73 In addition, 20% to 30% of H. influenzae isolates produce β-lactamase, which confers resistance to ampicillin.Citation72,Citation73 Ocular pathogen resistance to antimicrobial agents is increasing in parallel with an increase in antibiotic resistance in general, and is a major concern, since it narrows treatment choices for the management of common ocular infections.Citation74 Surveillance studies that document resistance among ocular pathogens include Ocular TRUSTCitation25,Citation26 and analyses of data from The Surveillance Network (TSN).Citation27
Increasing bacterial resistance in conjunctival infections
Studies of bacterial isolates from ophthalmic infections have reported an increase in resistance to the older fluoroquinolone ciprofloxacin among S. aureus and the emergence of methicillin-resistant S. aureus (MRSA).Citation26,Citation65,Citation74,Citation75 A nearly 3-fold increase in resistance to the older fluoroquinolones, including ciprofloxacin, among S. aureus isolates from conjunctival swabs was noted over a 10-year period (1994 to 2003), and the prevalence of MRSA among S. aureus isolates increased from 4.4% to 42.9% (P = 0.001). Citation31 Of note, a recent study of multidrug-resistant isolates (total of 1324 isolates examined) from clinical trials in bacterial conjunctivitis reported a significant prevalence of ciprofloxacin resistance in conjunction with methicillin resistance −65% of MRSA isolates and 47% of methicillin-resistant S. epidermidis isolates were also ciprofloxacin resistant.Citation76 Resistance has also increased to erythromycin and oxacillin among Gram-positive isolates and to trimethoprim/sulfamethoxazole (TMP/SMX) among Gram-negative isolates.Citation31 In a bacterial conjunctivitis study in pediatric patients (N = 428, ages 2 to 36 months), antibiotic resistance rates were high for pneumococcal isolates (penicillin, 60%; TMP/SMX, 38%; erythromycin, 23%; tetracycline, 18%; clindamycin, 9%).Citation77 Multidrug resistance was reported in 20% of pneumococcal isolates, highlighting the potential role of conjunctivitis in the spread of antibiotic-resistant pathogens.Citation77
In a phase III study of resistance to azithromycin and moxifloxacin among conjunctival isolates, the MIC90 for tested organisms was below the CLSI-established resistance breakpoints for moxifloxacin and above the resistance breakpoints for azithromycin (3-fold higher for H. influenzae; ≥128-fold higher for S. epidermidis; ≥16-fold higher for S. pneumoniae; ≥128-fold higher for S. aureus).Citation78 In a killing kinetic study, moxifloxacin exhibited a faster speed of bacterial kill than other nonfluoroquinolone antibiotics (tobramycin, gentamicin, polymyxin B/trimethoprim, or azithromycin) in S. aureus, S. pneumoniae, and H. influenzae isolated from conjunctival swabs.Citation79 These studies indicate that advanced-generation fluoroquinolones may kill bacteria more rapidly, leading to a faster resolution of ocular infection in the eye than with older topical ocular antibiotics and thereby reducing the risk of ocular drug resistance.Citation79
The trend of growing ocular bacterial antibiotic resistance was also seen in a decrease in in vitro susceptibility to gentamicin and tobramycin in corneal and conjunctival samples. Susceptibility decreased among all tested pathogens from 88% to 95% at the beginning of the study to 50% to 80% at the end of the 15-year surveillance period in 2000.Citation80 Ninety percent of bacteria in the cornea and 95% of bacteria in the conjunctiva remained susceptible to ciprofloxacin, norfloxacin, and ofloxacin in 2000.Citation80 A subsequent 2-year Brazilian study (N = 219) also concluded that advanced-generation fluoroquinolones, such as gatifloxacin and moxifloxacin, were more active than older antibiotics against Gram-positive bacteria.Citation81 It is therefore important to treat bacterial conjunctivitis rapidly to decrease disease transmission, shorten symptom duration, and minimize the emergence and spread of resistant bacteria.Citation79
Increasing bacterial resistance in keratitis infections
An increase in bacterial resistance has also been observed for keratitis infections. A review of resistance patterns over 2 consecutive 10-month periods found an increase in resistance rates among Gram-positive bacterial keratitis isolates to ciprofloxacin, cefazolin, and gentamicin.Citation82 Increased resistance to these commonly used antibiotics indicated a need for close follow-up after initial treatment and suggested maintaining a low threshold for selecting alternative therapy.Citation82 Among Gram-negative bacteria, a retrospective chart review of 1312 bacterial isolates from 1984 through 1999 found a significant (P = 0.0019) increase in chloramphenicol resistance, suggesting that chloramphenicol is unlikely to provide prophylactic coverage for Gram-negative ocular infections.Citation83 In a study of 291 patients with presumed bacterial keratitis, 68% were culture positive, of which 83% of cultures were Gram-positive, 17% Gram-negative, and 2% polymicrobial.Citation6 In a 5-year retrospective review of patients (N = 131) with bacterial keratitis, P. aeruginosa and S. aureus were the most common isolates, and 15.4% of S. aureus isolates were resistant to fluoroquinolones.Citation33 Similar results were noted in another study in which, overall, 96.2% of Gram-positive cocci isolated from bacterial keratitis samples (N = 104) were susceptible to gatifloxacin, whereas 60.4% were susceptible to ciprofloxacin.Citation84 No differences in susceptibility were observed among Gram-negative isolates.Citation84 Corneal ulcer healing rates with gatifloxacin were significantly (P < 0.01) higher for infections caused by Gram-positive pathogens but not for those caused by Gram-negative pathogens, indicating that gatifloxacin may be a preferred (albeit off-label) alternative to ciprofloxacin as the first-line monotherapy in bacterial keratitis.Citation84
As discussed earlier, higher concentrations of topical drugs are achievable in the eye; however, systemic minimum inhibitory concentration (MIC) values (CLSI standards) continue to be used as the susceptibility breakpoint in the treatment of ocular infections. The effect of MIC breakpoints on the rate of clinical response of bacterial keratitis isolates (N = 663) to ciprofloxacin showed that for MIC ≤ 1 μg/mL, the cure rate was 74.5% (n = 272), but for isolates with MIC ≥ 1 μg/mL, the cure rate was only 57.7% (n = 15). This could indicate that ciprofloxacin-resistant bacteria respond slowly to a higher concentration of ciprofloxacin,Citation85 that organisms with higher MICs do not attain adequate pharmacodynamic goals for treatment, or that resistant mutants frequently emerge. Although this study may be limited by an inherent overestimation of the level of ciprofloxacin susceptibility on response rates, susceptibility testing of corneal cultures may predict the response of bacterial keratitis to fluoroquinolone therapy.Citation85
S. aureus isolated from bacterial keratitis samples (N = 177) that was resistant to the older fluoroquinolones ciprofloxacin, levofloxacin, and ofloxacin remained susceptible to the advanced fluoroquinolones gatifloxacin and moxifloxacin.Citation23 The MIC90 for the advanced-generation fluoroquinolones was lower than the MIC90 for the older agents for all other Gram-positive bacteria tested, indicating that the advanced fluoroquinolones exhibited greater potency against bacterial keratitis pathogens. Although ciprofloxacin still had the lowest MIC90 for Gram-negative bacteria, overall the newer fluoroquinolones offer significant advantages, especially for Gram-positive bacteria, in the treatment of bacterial keratitis.Citation23 In one recent study, however, P. aeruginosa and S. aureus isolates from 2 cases of bacterial keratitis after refractive surgery showed resistance to moxifloxacin and gatifloxacin, highlighting the need to develop newer anti-infective agents.Citation86
Increasing bacterial resistance in endophthalmitis and other ocular infections
Antimicrobial resistance, including to the advanced-generation fluoroquinolones, has been identified from endophthalmitis isolates as well. The in vitro cross-resistance of gatifloxacin and moxifloxacin versus older fluoroquinolones was evaluated among 111 CoNS isolates recovered from patients with endophthalmitis over 15 years from January 1, 1990, through December 31, 2004.Citation87 More than 65% of the CoNS isolates resistant to ciprofloxacin (n = 38) also demonstrated in vitro cross-resistance to gatifloxacin (65.8%) and moxifloxacin (71.1%), indicating a significant increase in ocular pathogen resistance to fluoroquinolones over the 15-year period.Citation87 Increasing in vitro resistance to gatifloxacin and moxifloxacin may have important implications for the prevention and treatment of postoperative endophthalmitis and reinforce the need to develop new fluoroquinolones.Citation87
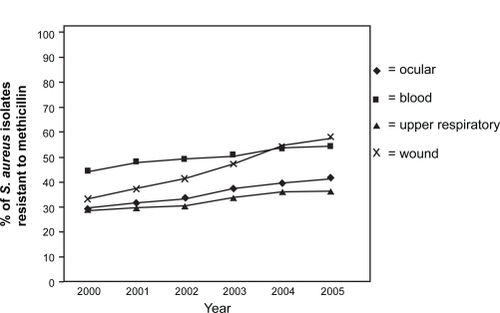
Overall, among bacterial isolates from ocular infections, MRSA strains increased from 29.5% in 2000 to 41.6% in 2005 ().Citation27 In this study of ocular isolates from more than 200 laboratories, fluoroquinolones were consistently active against methicillin-susceptible S. aureus (MSSA), S. pneumoniae, and H. influenzae but not against more than two-thirds of MRSA isolates.Citation27 Moxifloxacin, gatifloxacin, levofloxacin, and ciprofloxacin were, respectively, effective against 92.1%, 90.2%, 90.6%, and 91.1% of MSSA isolates, but only against 27.4%, 29.0%, 26.5%, and 31.6% of MRSA isolates.Citation25 In comparison, resistance among P. aeruginosa isolates was 10.5% to ciprofloxacin and gentamicin and 13.2% to gatifloxacin and ofloxacin.Citation27
Figure 1 Percentage of S. aureus isolates resistant to methicillin (MRSA rate) according to specimen source (2000 to 2005 based on TSN database analysis). Reproduced with permission from Asbell PA, Sahm DF, Shaw M, Draghi DC, Brown NP. Increasing prevalence of methicillin resistance in serious ocular infections caused by Staphylococcus aureus in the United States: 2000 to 2005. J Cataract Refract Surg. 2008;34(5):814–818.Citation27 Copyright © 2008 Elsevier.
Similar trends were observed by the Ocular TRUST program, which evaluates the annual change of in vitro antimicrobial susceptibilities of S. pneumoniae, H. influenzae, and S. aureus in national samples of ocular isolates.Citation26 In this study, 17% of S. aureus isolates were methicillin resistant. About 75% to 85% of MRSA isolates were resistant to ciprofloxacin, levofloxacin, moxifloxacin, and gatifloxacin; 64% were resistant to tobramycin; and 91% were resistant to azithromycin. Increased in vitro MRSA resistance suggests the need to consider newer, more potent anti-infective agents when MRSA is a likely pathogen.Citation26 The susceptibility rates of MSSA, S. pneumoniae, and H. influenzae to ciprofloxacin and levofloxacin varied from year to year, while the susceptibility patterns for the newer fluoroquinolones gatifloxacin and moxifloxacin in S. pneumoniae remained stable over the 8-year period studied ().Citation26 The Ocular TRUST 2 surveillance study reported that methicillin resistance in staphylococci was a marker for multidrug resistance. Susceptibility profiles for S. aureus, CoNS, S. pneumoniae, and H. influenzae to different ocular antibiotics also showed that newer fluoroquinolones were the most consistently active agents across the range of ocular pathogens.Citation88 A European study of susceptibility to topical antimicrobial agents among 532 ocular pathogens found that overall resistance was substantially higher among MRSA isolates and lower among MSSA isolates as well ().Citation89
Figure 2 S. pneumoniae susceptibility in ocular isolates by drug from the Ocular Tracking Resistance in the U.S. Today (TRUST 1) longitudinal surveillance program, 1999 through 2006. Reproduced with permission from Asbell PA, Colby KA, Deng S, et al. Ocular TRUST: nationwide antimicrobial susceptibility patterns in ocular isolates. Am J Ophthalmol. 2008;145(6):951–958.Citation26 Copyright © 2008 Elsevier.
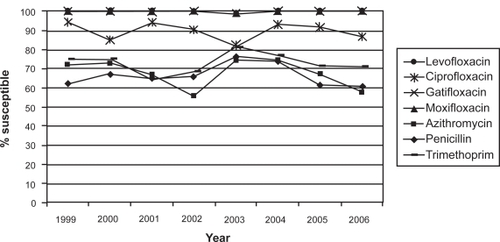
Table 2 Ocular pathogen susceptibility to topical antimicrobial agents (not shown: 36 nonpneumoniae streptococci, 39 miscellaneous)Citation89
As is evident from the studies discussed above, the increasing resistance of ocular pathogens to antibiotics has followed global increases in resistance to systemic antibiotics.Citation71 These changes have important implications for the selection of antibiotic therapy for ocular infections.Citation75 It is important to choose antibiotics with rapid bactericidal activity, based on a combination of microbiology (low MIC90 values) and pharmacokinetic (PK) and pharmacodynamic (PD) data that predict killing of bacteria with limited development of pathogen resistance. The advanced-generation fluoroquinolones moxifloxacin and gatifloxacin have been efficacious for resolving ocular infections but have also been used systemically, increasing the chances of ocular pathogens having resistance to these agents.Citation75,Citation90–Citation92 Although most of the new fluoroquinolones in development are being developed for systemic use, ideally newer agents should be specifically designed for topical ophthalmic use with an optimized combination of PK and reduced MIC90 (and thus optimized PD) versus MRSA isolates for increased efficacy and safety.Citation27,Citation90–Citation92 Breakpoints specific for topically administered ophthalmic antibiotics are needed to better understand resistance among ocular pathogens.Citation90–Citation92 Use of effective PD profiles of these new drugs to optimize antibiotic administration, maximize bactericidal effect, and minimize toxicity can lead to better clinical outcomes and prevention of bacterial resistance.Citation93
Importance of pharmacokinetics and pharmacodynamics in the development of new agents in ocular infection therapy
Over the last decade, several lines of research have helped us understand the relevance of PD data in the development of new antibiotics for ocular infection.Citation93 In preclinical studies, for a given organism, PD parameters provide a measurement for the rate and extent of bacterial kill and help to provide guidance on optimal modes of drug administration and reducing antibiotic resistance.Citation93 A key measure for the optimization of an antibiotic’s PD is the amount of time the free drug remains available at an exposure greater than the MIC (T < MIC) for a pathogen, defined as the time-dependent killing of the pathogen. Another measure for PD optimization of an antibiotic is the ratio of area under the free-drug concentration time curve (AUC) at 24 hours to the MIC (concentration-dependent killing) or AUC:MIC.Citation94 The maximum concentration of the drug in target tissue after a dose (Cmax) compared to MIC (Cmax/MIC) is another parameter used to obtain the PD index. The relative importance of each of the PD parameters to a drug’s antibacterial activity varies among antibiotics.Citation94 For the fluoroquinolones, it has been estimated that a Cmax:MIC90 ratio of at least 10 and an AUC:MIC90 ratio of at least 100 are required to predict microbiological and clinical efficacy.Citation95
The PD properties of an antibiotic vary by organism. A study of 7 fluoroquinolones compared the AUC:MIC ratio with an index based on the time needed after the removal of antibiotic for surviving bacteria to resume growth and reach 109 CFU/mL bacterial culture growth density.Citation96 The AUC:MIC ratio and the antimicrobial effect index (IE) were shown to be specific to each fluoroquinolone, with moxifloxacin and grepafloxacin having 1.4 times the anti-staphylococcal effects of ciprofloxacin.Citation96 When comparing therapeutically attainable total drug AUCs of fluoroquinolones in humans with the IE and the known ciprofloxacin susceptibility breakpoint, moxifloxacin, grepafloxacin, and trovafloxacin would require smaller AUC:MIC ratios to attain the same acceptable antistaphylococcal effect as ciprofloxacin, indicating greater potency of the newer fluoroquinolones.Citation96
Optimal antibiotic PD may reduce the development of resistant mutants. Recent data with the fluoroquinolones suggest that a mutant-prevention concentration (MPC) may exist for certain organisms, such as S. pneumoniae.Citation97 Although MPC has not been applied to other classes of antibiotics in general, the MPC for fluoroquinolones defines the antimicrobial drug concentration threshold that would require an organism to possess 2 mutations simultaneously for growth in the presence of the drug.Citation29,Citation98 Mutant prevention concentration and PD enable a clinician to optimize antimicrobial therapy by sustaining an antibiotic’s ability to kill organisms while suppressing the emergence of resistant subpopulations of organisms.Citation29,Citation99,Citation100
It is possible to extend the duration of antibiotic exposure for the ocular pathogen through the use of topical ocular antibiotics since these agents can achieve higher concentrations of the drug in the eye than systemic antibiotics. Factors that lead to high concentrations in the eye include the concentration of the formulation, its lipophilicity, and its aqueous solubility.Citation101 To meet the need for differing ocular concentrations, ophthalmic antibiotics may be available in more than one formulation: for example, levofloxacin 0.5% and 1.5% for bacterial conjunctivitis and keratitis, respectively.Citation37,Citation102 However, topical formulations are often limited by formulation, such as solubility and stability, and by toxicity issues that could make it difficult to achieve increased efficacy through higher concentrations.
In light of the increasing antibiotic resistance pattern of bacteria worldwide, including resistance to the more potent, advanced-generation fluoroquinolones, the development of still newer, more potent fluoroquinolones and improvements in treatment protocols for ocular infections have become more important.
A novel fluoroquinolone under investigation for the treatment of ocular infections
Fluoroquinolones act by binding and inhibiting 2 enzymes involved in the synthesis of bacterial DNA – DNA gyrase and DNA topoisomerase IV – and are therefore considered to have a dual mechanism of action.Citation103 Newer fluoroquinolones such as gatifloxacin and moxifloxacin have potent activity against both of these enzymes in both Gram-negative and Gram-positive organisms. In contrast, older fluoroquinolones, such as ofloxacin and ciprofloxacin, preferentially bind DNA gyrase in Gram-negative organisms and topoisomerase IV in Gram-positive organisms, leading to the potential for resistance to these agents following a single mutation in the target enzyme.Citation103 In the newer fluoroquinolones, with strong affinities for both enzymes, double mutation of both target enzymes is needed for high-level resistance to develop.Citation103
Besifloxacin (Besivance™; Bausch and Lomb Inc., Rochester, NY, USA), is a new fluoroquinolone that was recently approved by the US Food and Drug Administration for the treatment of bacterial conjunctivitis. This agent has a unique structure which may increase its potency.Citation104 Besifloxacin ophthalmic suspension 0.6% has been developed exclusively for the treatment of ocular infections, reducing the risk of the emergence of resistant strains due to prior widespread systemic exposure to that agent.Citation104 Besifloxacin’s mechanism of action is similar to that of other fluoroquinolones in that it kills bacteria through inhibition of DNA gyrase and topoisomerase IV.Citation105 Unlike older representatives of that drug family, besifloxacin has balanced dual activity, inhibiting both enzymes at similar as well as lower concentrations. Thus, the inhibition of the enzymatic activities of DNA gyrase and topoisomerase IV of S. pneumoniae occurs at lower concentrations with besifloxacin than with ciprofloxacin, and even with moxifloxacin.Citation105 Since both enzymes are targeted simultaneously, mutations leading to high-level resistance to besifloxacin cannot occur in a single step. While mutations that increased the MIC values for besifloxacin were found in laboratory strains of E. coli, S. aureus, and S. pneumoniae, the increase in MIC was far greater for the comparators ciprofloxacin and moxifloxacin.Citation105 Besifloxacin has been shown to be active in vitro against a broad spectrum of pathogens, including the most common pathogens of bacterial conjunctivitis as well as drug-resistant isolates ().Citation76,Citation106
Table 3 MIC90 values for besifloxacin against common causes of bacterial conjunctivitisCitation76,Citation106
Besifloxacin demonstrated efficacy in an in vivo murine infection model and excellent ocular pharmacokinetics in rabbits, with ocular mean residence times of >7 hours and conjunctival concentrations in excess of the MIC90 for nonresistant ophthalmic isolates for >12 hours following a single dose.Citation104 Single doses of besifloxacin administered to rabbit eyes maintained high concentrations in tears, conjunctiva, and aqueous humor, with mean residence times of 923, 458, and 422 minutes, respectively.Citation104,Citation107 Compared with gatifloxacin and moxifloxacin, besifloxacin demonstrated greater exposure in tears and conjunctiva with lower systemic concentrations.Citation108 The conjunctival Cmax:MIC90 ratio for besifloxacin exceeds 10 for all 8 nonresistant species, and the AUC:MIC90 ratio exceeds 100 for all species except P. aeruginosa.Citation104 Based on a conjunctival besifloxacin Cmax of 63 μg/mL and a predicted (from PK modeling and simulations) AUC(0–24 h) of 214 μg·h/mL, 3 times per day (tid) dosing of besifloxacin 0.6% for 1 week should attain adequate therapeutic AUC:MIC90 ratios and prevent the development of 2-step resistant mutants.Citation104
In a rabbit model of MRSA-induced endophthalmitis, besifloxacin treatment resulted in significant improvement in clinical score (reductions in the signs and symptoms of endophthalmitis), while gatifloxacin, levofloxacin, and moxifloxacin were ineffective.Citation109 Besifloxacin also exhibited significant dose-dependent inhibition of IL-1β or lipopolysaccharidestimulated cytokines in human monocytes, with a comparable or better potency than moxifloxacin, indicating that besifloxacin may have anti-inflammatory activity.Citation110 Similarly, besifloxacin significantly inhibited IL-1 ß-induced release of proinflammatory cytokines in primary human corneal epithelial cells in a dose-dependent manner, with a comparable or better efficacy compared to moxifloxacin.Citation109 Although the clinical significance of anti-inflammatory activity has not been established, reducing inflammation associated with infections may enhance drug access to ocular tissue and reduce tissue damage.Citation109,Citation110
Human subjects (N = 64) administered a single-dose of besifloxacin ophthalmic suspension 0.6% in both eyes had mean tear AUC:MIC ratios (24 hours) ranging from 2464 to 20,533 for S. aureus, S. pneumoniae, S. epidermidis, and H. influenzae.Citation111 On average, besifloxacin concentrations of 1.6 μg/g or higher were sustained in tears for at least 24 hours after a single dose.Citation112 These values are greater than the MIC90 values for the common ocular pathogens and are above the exposure needed to eradicate the organism and prevent the development of resistant mutants.Citation111 The PD data presented here are therefore indicative of a prolonged and effective ocular concentration of the drug. The high AUC:MIC ratio over 24 hours reported in this study suggests that the extended-release mucoadhesive polymer (DuraSite®; Insite Vision, Alameda, CA, USA) used for the besifloxacin ophthalmic suspension formulation is an optimal choice for the treatment of ocular infections. In this context, formulations such as in situ gelling ophthalmic delivery systems have also been reported to provide increased bioavailability for fluoroquinolones such as gatifloxacin, ciprofloxacin, and ofloxacin although it is not clear if or when these products may become available in the future.Citation113–Citation115
The efficacy and safety of besifloxacin ophthalmic suspension 0.6% was studied in two multicenter, randomized, double-masked, vehicle-controlled, parallel-design trials with patient populations of 269 and 957. In both trials, the efficacy and safety of besifloxacin ophthalmic suspension 0.6% tid for 5 days was compared with vehicle for the complete clinical resolution and eradication of bacterial infection.Citation116,Citation117 In the first trial, clinical resolution at the primary analysis visit (Day 8) occurred in 73.3% (44/60) of besifloxacin-treated patients with culture-confirmed conjunctivitis versus 43.1% (25/58) of patients receiving vehicle (P < 0.001).Citation116 Bacterial eradication occurred in 88.3% (53/60) of patients in the besifloxacin group versus 60.3% (35/58) of vehicle-treated patients (P < 0.001).Citation116 In the second trial, clinical resolution at the primary analysis visit (Day 5) occurred in 45.2% (90/199) of besifloxacin-treated patients with culture-confirmed conjunctivitis versus 33.0% (63/191) of patients receiving vehicle (P = 0.0084), while bacterial eradication occurred in 91.5% (182/199) of patients in the besifloxacin group versus 59.7% (114/191) of vehicle-treated patients (P < 0.0001).Citation117 In the first trial, the cumulative frequency of ocular adverse events (AEs) was similar between the 2 groupsCitation116; however, in the second trial, the cumulative frequency of ocular AEs was statistically greater in the vehicle treatment group (P = 0.0047), due, in part, to the higher incidence of conjunctivitis in the vehicle-treated group.Citation117
A non-inferiority study compared the efficacy and safety of besifloxacin and moxifloxacin 0.5% tid for 5 days for the treatment of bacterial conjunctivitis (N = 1161, 533 of whom had positive cultures).Citation118 Clinical resolution at the primary analysis visit (Day 5) occurred in 58.3% and 59.4% of patients (besifloxacin and moxifloxacin, respectively; P = 0.652; CI, −9.48% to 7.29%), and bacterial eradication occurred in 93.3% and 91.1% (besifloxacin and moxifloxacin, respectively; P = 0.1238; CI, −2.44% to 6.74%), indicating that besifloxacin was non-inferior to moxifloxacin for the treatment of bacterial conjunctivitis.Citation118 Besifloxacin was well tolerated, with an incidence of AEs that was similar to that reported for vehicle or moxifloxacin with no unexpected findings.Citation118 Eye irritation was the only ocular AE statistically different between treatment groups, occurring in 0.3% of subjects on besifloxacin and 1.4% of subjects on moxifloxacin (P = 0.0201). The only nonocular AE that occurred in more than 1% was headache (1.2% besifloxacin, 1.6% moxifloxacin).Citation118
Strategies for prevention of antibiotic resistance in ocular pathogens
The Centers for Disease Control and Prevention and the World Health Organization have proposed strategies to preserve the usefulness of antibiotics.Citation119,Citation120 In addition to global surveillance programs, adequate training and awareness programs should be implemented.Citation119,Citation120 However, surveillance programs must be evaluated with reference to the PD data that influence the concentration of an antibiotic in the eye. Ocular TRUST data show that ciprofloxacin resistance has increased over the past decade.Citation26 The improved PD properties of the newer generation fluoroquinolones help to maximize the concentration of the antibiotic at the site of infection and help to reduce the incidence of bacterial resistance. Strategies to prevent or delay the development of antibiotic resistance among ocular pathogens include the prescription of antibiotics only when needed and the use of sensitivity testing to prescribe the appropriate antibiotic.Citation75 Additional recommended strategies for the prevention of antibiotic resistance are completion of the full course of therapy and the decrease in the use of antibiotics for growth promotion in animals and agriculture, as well as the development of new antibiotic agents with optimized PD.Citation121 Ultimate outcomes of treatment depend on efficacy and safety of the pharmacotherapy as well as adherence to the established guidelines. Prevention of ocular antibiotic resistance requires cooperation between patients, physicians (both eye care and non-eye care), and the pharmaceutical industry to keep current antibiotics effective for a longer time and to develop newer antibiotic agents to stay ahead of the changing microbial pathogenesis.
Conclusion
Evolving bacterial resistance represents a worldwide challenge in the clinical management of infection. A parallel increase in resistance among ocular pathogens has necessitated transitioning from older to newer, more potent antibiotics. In the future, antibiotics for ocular infections should possess a broad spectrum of activity against a wide range of pathogens and be effective and safe to use at the optimized PK/PD and MIC90 against resistant strains of bacteria.Citation22 Currently, the newer fluoroquinolones gatifloxacin and moxifloxacin, and in the near future besifloxacin, appear to represent the best choice for treating and preventing ophthalmic infections. Agents developed specifically for ocular use only may help to overcome the evolving global antibiotic resistance problem that has resulted from inappropriate widespread use of systemic antibiotics.
Acknowledgments and Disclosures
The author wishes to thank Richard S Perry, PharmD, of Churchill Communications and Richa Attre, PhD, of The Scienomics Group for writing and editorial assistance. The author declares no conflicts of interest.
References
- SnyderRGlasserDAntibiotic therapy for ocular infectionWest J Med199416165795847856158
- HughesLMauriceDA fresh look at iontophoresisArch Ophthalmol198410212182518296508622
- HovdingGAcute bacterial conjunctivitisActa Ophthalmol200886151717970823
- RosePManagement strategies for acute infective conjunctivitis in primary care: a systematic reviewExpert Opin Pharmacother20078121903192117696792
- AllanBDDartJKStrategies for the management of microbial keratitisBr J Ophthalmol19957987777867547792
- BourcierTThomasFBorderieVChaumeilCLarocheLBacterial keratitis: predisposing factors, clinical and microbiological review of 300 casesBr J Ophthalmol200387783483812812878
- GreenMApelAStapletonFRisk factors and causative organisms in microbial keratitisCornea2008271222718245962
- GreenMDApelAJNaduvilathTStapletonFJClinical outcomes of keratitisClin Experiment Ophthalmol200735542142617651246
- CalleganMCGilmoreMSGregoryMBacterial endophthalmitis: therapeutic challenges and host-pathogen interactionsProg Retin Eye Res200726218920317236804
- DeCroosFCAfshariNAPerioperative antibiotics and anti-inflammatory agents in cataract surgeryCurr Opin Ophthalmol2008191222618090893
- KowalskiRPDhaliwalDKOcular bacterial infections: current and future treatment optionsExpert Rev Anti Infect Ther20053113113915757463
- Tovilla-CanalesJLNavaATovilla y PomarJLOrbital and periorbital infectionsCurr Opin Ophthalmol200112533534111588494
- CampolattaroBNLuederGTTychsenLSpectrum of pediatric dacryocystitis: medical and surgical management of 54 casesJ Pediatr Ophthalmol Strabismus19973431431539168418
- Summary benchmarks for preferred practice pattern guidelinesSan Francisco, CAAmerican Academy of Ophthalmology2007
- American Academy of Ophthalmology Cornea and External Disease PanelPreferred practice pattern: conjunctivitisSan Francisco, CAAmerican Academy of Ophthalmology2003
- American Academy of Ophthalmology Cornea and External Disease PanelPreferred practice pattern: bacterial keratitisSan Francisco, CAAmerican Academy of Ophthalmology2005
- DartJKRadfordCFMinassianDVermaSStapletonFRisk factors for microbial keratitis with contemporary contact lenses: a case-control studyOphthalmology2008115101647165418597850
- DonahueSPKhouryJMKowalskiRPCommon ocular infections. A prescriber’s guideDrugs19965245265408891465
- BartlettJDOphthalmic Drug Facts20th edSt Louis, MOWolters Kluwer Health2009
- MulliganMJCobbsCGBacteriostatic versus bactericidal activityInfect Dis Clin North Am1989333893982671128
- FraunfelderFCorneal toxicity from topical ocular and systemic medicationsCornea200625101133113817172885
- SchlechBABlondeauJFuture of ophthalmic anti-infective therapy and the role of moxifloxacin ophthalmic solution 0.5% (VIGAMOX)Surv Ophthalmol200550Suppl 1S64S6716257312
- KowalskiRPDhaliwalDKKarenchakLMGatifloxacin and moxifloxacin: an in vitro susceptibility comparison to levofloxacin, ciprofloxacin, and ofloxacin using bacterial keratitis isolatesAm J Ophthalmol2003136350050512967804
- StrattonCWDead bugs don’t mutate: susceptibility issues in the emergence of bacterial resistanceEmerg Infect Dis200391101612533275
- AsbellPASahmDFNationwide antimicrobial susceptibility surveillance of ocular isolates: results of Ocular TRUSTPresented at the American Society of Cataract and Refractive Surgery Annual Meeting2007 Apr 22–May 2San Diego, CAAbstract #P-114.
- AsbellPAColbyKADengSOcular TRUST: nationwide antimicrobial susceptibility patterns in ocular isolatesAm J Ophthalmol2008145695195818374299
- AsbellPASahmDFShawMDraghiDCBrownNPIncreasing prevalence of methicillin resistance in serious ocular infections caused by Staphylococcus aureus in the United States: 2000 to 2005J Cataract Refract Surg200834581481818471638
- HwangDGThe top four errors in prescribing antibioticsCataract Refract Surg Today220055558
- BlondeauJMHansenGMetzlerKHedlinPThe role of PK/PD parameters to avoid selection and increase of resistance: mutant prevention concentrationJ Chemother200416Suppl 311915334827
- BartlettJDJaanusSClinical Ocular PharmacologySt. Louis, MOButterworth Heinemann Elsevier2008
- CavuotoKZutshiDKarpCLMillerDFeuerWUpdate on bacterial conjunctivitis in South FloridaOphthalmology20081151515617572497
- SheikhAHurwitzBAntibiotics versus placebo for acute bacterial conjunctivitisCochrane Database Syst Rev20062CD00121116625540
- PachigollaGBlomquistPCavanaghHDMicrobial keratitis pathogens and antibiotic susceptibilities: a 5-year review of cases at an urban county hospital in north TexasEye Contact Lens2007331454917224678
- KeayLEdwardsKNaduvilathTMicrobial keratitis predisposing factors and morbidityOphthalmology2006113110911616360210
- Ciloxan [package insert]Fort Worth, TXAlcon Laboratories, Inc31998
- Ocuflox [package insert]Irvine, CAAllergan Inc71993
- Iquix [package insert]Jacksonville, FLVistakon Pharmaceuticals LLC42007
- BhavsarARIpMSGlassmanARThe risk of endophthalmitis following intravitreal triamcinolone injection in the DRCRnet and SCORE clinical trialsAm J Ophthalmol2007144345445617765429
- JonasJBIntravitreal triamcinolone acetonide: a change in a paradigmOphthalmic Res200638421824516763379
- TabanMBehrensANewcombRAcute endophthalmitis following cataract surgery: a systematic review of the literatureArch Ophthalmol2005123561362015883279
- WestESBehrensAMcDonnellPJTielschJMScheinODThe incidence of endophthalmitis after cataract surgery among the US Medicare population increased between 1994 and 2001Ophthalmology200511281388139415953637
- JohnsonMDoftBKelseySThe Endophthalmitis Vitrectomy Study: relationship between clinical presentation and microbiologic spectrumOphthalmology199710422612729052630
- JagerRAielloLPatelSCunninghamEJRisks of intravitreous injection: a comprehensive reviewRetina200424567669815492621
- JonasJBKreissigISpandauUHHarderBInfectious and noninfectious endophthalmitis after intravitreal high-dosage triamcinolone acetonideAm J Ophthalmol2006141357958016490517
- JonasJBSpandauUHRenschFVon BaltzSSchlichtenbredeFInfectious and noninfectious endophthalmitis after intravitreal bevacizumabJ Ocul Pharmacol Ther200723324024217593007
- JonasJBSpandauUHSchlichtenbredeFShort-term complications of intravitreal injections of triamcinolone and bevacizumabEye200822459059118292795
- YamJCKwokAKUpdate of the management of postoperative endophthalmitisHong Kong Med J200410533734315479963
- ChhabraSKunimotoDYKaziLEndophthalmitis after open globe injury: microbiologic spectrum and susceptibilities of isolatesAm J Ophthalmol2006142585285417056367
- RecchiaFMBusbeeBGPearlmanRBCarvalho-RecchiaCAHoACChanging trends in the microbiologic aspects of postcataract endophthalmitisArch Ophthalmol2005123334134615767476
- MoshirfarMFeizVVitaleATWegelinJABasavanthappaSWolseyDHEndophthalmitis after uncomplicated cataract surgery with the use of fourth-generation fluoroquinolones: a retrospective observational case seriesOphthalmology2007114468669117184840
- OlsonRReducing the risk of postoperative endophthalmitisSurv Ophthalmol200449Suppl 2S55S6115028480
- KelkarAKelkarJAmuakuWKelkarUShaikhAHow to prevent endophthalmitis in cataract surgeriesIndian J Ophthalmol200856540340718711270
- Endophthalmitis Study GroupEuropean Society of Cataract and Refractive SurgeonsProphylaxis of postoperative endophthalmitis following cataract surgery: results of the ESCRS multicenter study and identification of risk factorsJ Cataract Refract Surg200733697898817531690
- MasketSPreventing, diagnosing, and treating endophthalmitisJ Cataract Refract Surg19982467257269642575
- SchmitzSDickHKrummenauerFPfeifferNEndophthalmitis in cataract surgery: results of a German surveyOphthalmology1999106101869187710519579
- JacksonWBlepharitis: current strategies for diagnosis and managementCan J Ophthalmol200843217017918347619
- GrodenLMurphyBRodniteJLid flora in blepharitisCornea19911050532019106
- RutarTZwickOMCockerhamKPHortonJCBilateral blindness from orbital cellulitis caused by community-acquired methicillin-resistant Staphylococcus aureusAm J Ophthalmol2005140474074216226533
- CannonPKeagDRadfordRAtaullahSLeatherbarrowBOur experience using primary oral antibiotics in the management of orbital cellulitis in a tertiary referral centreEye200923361261518309335
- DasJDekaAKuriGBhattacharjeeKDasDGogoiKBacteriology of chronic dacryocystitis in adult population of northeast IndiaOrbit200827424324718716961
- KubalAGaribaldiDDacryoadenitis caused by methicillin-resistant Staphylococcus aureusOphthal Plast Reconstr Surg20082415061
- BriscoeDRubowitzAAssiaEChanging bacterial isolates and antibiotic sensitivities of purulent dacryocystitisOrbit2005242959816191795
- HarbarthSSamoreMHAntimicrobial resistance determinants and future controlEmerg Infect Dis200511679480115963271
- GumsJGBoatwrightDWTottiNMartinezMAntimicrobial resistance in 11 hospitals in Puerto Rico: results of an antimicrobial resistance management (ARM) programP R Health Sci J200726318118918035809
- GoldsteinMHKowalskiRPGordonYJEmerging fluoroquinolone resistance in bacterial keratitis: a 5-year reviewOphthalmology199910671313131810406613
- MilianiKL’HeriteauFAlfandariSSpecific control measures for antibiotic prescription are related to lower consumption in hospitals: results from a French multicentre pilot studyJ Antimicrob Chemother200862482382918658196
- HobanDFelminghamDThe PROTEKT surveillance study: antimicrobial susceptibility of Haemophilus influenzae and Moraxella catarrhalis from community-acquired respiratory tract infectionsJ Antimicrob Chemother200250Suppl S1495912239228
- KirbyJTMutnickAHJonesRNBiedenbachDJPfallerMAGeographic variations in garenoxacin (BMS284756) activity tested against pathogens associated with skin and soft tissue infections: report from the SENTRY Antimicrobial Surveillance Program (2000)Diagn Microbiol Infect Dis200243430330912151191
- TenoverFCMechanisms of antimicrobial resistance in bacteriaAm J Med20061196 Suppl 1S3S10; discussion S62–S70.16735149
- BarlowGNathwaniDIs antibiotic resistance a problem? A practical guide for hospital cliniciansPostgrad Med J20058196168069216272230
- CroftACD’AntoniAVTerzulliSLUpdate on the antibacterial resistance crisisMed Sci Monit2007136RA103RA11817534243
- BrownSDRybakMJAntimicrobial susceptibility of Streptococcus pneumoniae, Streptococcus pyogenes and Haemophilus influenzae collected from patients across the USA, in 2001–2002, as part of the PROTEKT US studyJ Antimicrob Chemother200454Suppl 1i7i1515265831
- JacobsMRFelminghamDAppelbaumPCGrunebergRNThe Alexander Project 1998–2000: susceptibility of pathogens isolated from community-acquired respiratory tract infection to commonly used antimicrobial agentsJ Antimicrob Chemother200352222924612865398
- MarangonFBMillerDMuallemMSRomanoACAlfonsoECCiprofloxacin and levofloxacin resistance among methicillin-sensitive Staphylococcus aureus isolates from keratitis and conjunctivitisAm J Ophthalmol2004137345345815013867
- BlomquistPHMethicillin-resistant Staphylococcus aureus infections of the eye and orbit (an American Ophthalmological Society thesis)Trans Am Ophthalmol Soc200610432234517471350
- McDonaldMBBlondeauJMDeCoryHHMultidrug-resistant strains in clinical trials of besifloxacin in the treatment of bacterial conjunctivitisPresented at the American Academy of Ophthalmology Annual Meeting2008 Nov 8–11Atlanta, GA, USAPoster 070.
- BuznachNDaganRGreenbergDClinical and bacterial characteristics of acute bacterial conjunctivitis in children in the antibiotic resistance eraPediatr Infect Dis J200524982382816148850
- OhnsmanCRitterbandDO’BrienTGirgisDKabatAComparison of azithromycin and moxifloxacin against bacterial isolates causing conjunctivitisCurr Med Res Opin20072392241224917688706
- LichtensteinSJWagnerRSJamisonTBellBStromanDWSpeed of bacterial kill with a fluoroquinolone compared with nonfluoroquinolones: clinical implications and a review of kinetics of kill studiesAdv Ther20072451098111118029337
- ChalitaMRHofling-LimaALParanhosAJrSchorPBelfortRJrShifting trends in in vitro antibiotic susceptibilities for common ocular isolates during a period of 15 yearsAm J Ophthalmol20041371435114700643
- OliveiraADD’AzevedoPAFranciscoWIn vitro activity of fluoroquinolones against ocular bacterial isolates in Sao Paulo, BrazilCornea200726219419817251812
- AfshariNAMaJJDuncanSMTrends in resistance to ciprofloxacin, cefazolin, and gentamicin in the treatment of bacterial keratitisJ Ocul Pharmacol Ther200824221722318331204
- TuftSJMathesonMIn vitro antibiotic resistance in bacterial keratitis in LondonBr J Ophthalmol200084768769110873974
- ParmarPSalmanAKalavathyCMComparison of topical gatifloxacin 0.3% and ciprofloxacin 0.3% for the treatment of bacterial keratitisAm J Ophthalmol2006141228228616458681
- WilhelmusKRAbshireRLSchlechBAInfluence of fluoroquinolone susceptibility on the therapeutic response of fluoroquinolone-treated bacterial keratitisArch Ophthalmol200312191229123312963604
- MoshirfarMMirzaianGFeizVKangPCFourth-generation fluoroquinolone-resistant bacterial keratitis after refractive surgeryJ Cataract Refract Surg200632351551816631067
- MillerDFlynnPMScottIUAlfonsoECFlynnHWJrIn vitro fluoroquinolone resistance in staphylococcal endophthalmitis isolatesArch Ophthalmol2006124447948316606872
- AsbellPASahmDFLongitudinal nationwide antimicrobial susceptibility surveillance in ocular isolates: results from Ocular TRUST 2Presented at: American Society of Cataract and Refractive Surgery Annual Meeting2007 April 27–May 2San Diego, CA, USA
- MorrisseyIBurnettRViljoenLRobbinsMSurveillance of the susceptibility of ocular bacterial pathogens to the fluoroquinolone gatifloxacin and other antimicrobials in Europe during 2001/2002J Infect200449210911415236917
- BrownLResistance to ocular antibiotics: an overviewClin Exp Optom200790425826217535364
- TzepiIVergadosIKanellakopoulouKPharmacokinetics of intravenously administered moxifloxacin in eye compartments: an experimental studyInt J Antimicrob Agents200933216016218947985
- WiseRAndrewsJThe bactericidal activity of gatifloxacin in plasma and urineClin Microbiol Infect19984739239611864354
- DrusanoGLPharmacokinetics and pharmacodynamics of antimicrobialsClin Infect Dis200745Suppl 1S89S9517582578
- AmbrosePGBhavnaniSMRubinoCMPharmacokinetics-pharmacodynamics of antimicrobial therapy: it’s not just for mice anymoreClin Infect Dis2007441798617143821
- WrightDHBrownGHPetersonMLRotschaferJCApplication of fluoroquinolone pharmacodynamicsJ Antimicrob Chemother200046566968311062185
- FirsovAALubenkoIYVostrovSNPortnoyYAZinnerSHAntistaphylococcal effect related to the area under the curve/MIC ratio in an in vitro dynamic model: predicted breakpoints versus clinically achievable values for seven fluoroquinolonesAntimicrob Agents Chemother20054972642264715980331
- BlondeauJMZhaoXHansenGDrlicaKMutant prevention concentrations of fluoroquinolones for clinical isolates of Streptococcus pneumoniaeAntimicrob Agents Chemother200145243343811158737
- MetzlerKHansenGMHedlinPHardingEDrlicaKBlondeauJMComparison of minimal inhibitory and mutant prevention drug concentrations of 4 fluoroquinolones against clinical isolates of methicillin-susceptible and -resistant Staphylococcus aureusInt J Antimicrob Agents200424216116715288315
- DrusanoGLLouieADezielMGumboTThe crisis of resistance: identifying drug exposures to suppress amplification of resistant mutant subpopulationsClin Infect Dis200642452553216421797
- TamVHLouieAFritscheTRImpact of drug-exposure intensity and duration of therapy on the emergence of Staphylococcus aureus resistance to a quinolone antimicrobialJ Infect Dis2007195121818182717492598
- RobertsonSMCurtisMASchlechBAOcular pharmacokinetics of moxifloxacin after topical treatment of animals and humansSurv Ophthalmol200550Suppl 1S32S4516257309
- Quixin [package insert]Jacksonville, FLVistakon Pharmaceuticals LLC42006
- BlondeauJMFluoroquinolones: mechanism of action, classification, and development of resistanceSurv Ophthalmol200449Suppl 2S73S7815028482
- WardKWLepageJFDriotJYNonclinical pharmacodynamics, phar-macokinetics, and safety of BOL-303224-A, a novel fluoroquinolone antimicrobial agent for topical ophthalmic useJ Ocul Pharmacol Ther200723324325617593008
- CambauEMatratSPanXSTarget specificity of the fluoroquinolone besifloxacin in Streptococcus pneumoniae, Staphylococcus aureus and Escherichia coliJ Antimicrob Chemother200963344345019147516
- BrunnerLSNortonSEBlondeauJMIn vitro activity of SS734, a novel fluoroquinolone, against pathogens associated with bacterial conjunctivitis[poster] 17th European Congress of Clinical Microbiology and Infectious DiseasesMarch 31–April 3, 2007Munich, GermanyPoster P1679.
- ProkschJWDriotJYWardKWNonclinical ocular and systemic pharmacokinetics of BOL-303224-A, a novel fluoroquinolone antimicrobial agent for topical ophthalmic usePresented at the Association for Research in Vision and Ophthalmology Annual Meeting2007 Apr 27–May 1Fort Lauderdale, FL, USAPoster #B654.
- ChappaAKProkschJWWardKWComparison of the ocular and systemic pharmacokinetics of besifloxacin, a novel fluoroquinolone antibiotic, with moxifloxacin and gatifloxacin in pigmented rabbitsPresented at the Association for Research in Vision and Ophthalmology Annual Meeting2008 Apr 27–May 1Fort Lauderdale, FL, USAPoster #D684.
- ZhangJZCavetMEWardKWAnti-inflammatory effects of besifloxacin, a novel fluoroquinolone, in primary human corneal epithelial cellsCurr Eye Res2008331192393319085374
- ZhangJZWardKWBesifloxacin, a novel fluoroquinolone antimicrobial agent, exhibits potent inhibition of pro-inflammatory cytokines in human THP-1 monocytesJ Antimicrob Chemother200861111111617965029
- GranvilCPSiou-MermetRComstockTJonasseMProkschJWOcular pharmacokinetics of besifloxacin, a novel fluoroquinolone antimicrobial agent for topical ophthalmic use, in healthy volunteersPresented at the Association for Research in Vision and Ophthalmology Annual Meeting2008 Apr 27–May 1Fort Lauderdale, FL, USAPoster #D691.
- ProkschJGranvilCPSiou-MermetRComstockTPaternoMWardKWOcular pharmacokinetics of besifloxacin following topical administration to rabbits, monkeys, and humansJ Ocul Pharm Ther2009254335341
- LiuZLiJNieSLiuHDingPPanWStudy of an alginate/HPMC-based in situ gelling ophthalmic delivery system for gatifloxacinInt J Pharm20063151–2121716616442
- MansourMMansourSMortadaNDAbd ElhadySSOcular poloxamer-based ciprofloxacin hydrochloride in situ forming gelsDrug Dev Ind Pharm200834774475218612913
- AbrahamSFurtadoSBharathSBasavarajBVDeveswaranRMadhavanVSustained ophthalmic delivery of ofloxacin from an ion-activated in situ gelling systemPak J Pharm Sci200922217517919339228
- KarpeckiPDePaolisMHunterJABesifloxacin ophthalmic suspension 0.6% in patients with bacterial conjunctivitis: a multicenter, prospective, randomized, double-masked, vehicle-controlled, 5-day efficacy and safety studyClin Ther200931351452619393842
- TepedinoMEHellerWHUsnerDWPhase III efficacy and safety study of besifloxacin ophthalmic suspension 0.6% in the treatment of bacterial conjunctivitisCurr Med Res Opin20092551159116919323612
- McDonaldMBProtzkoEEBrunnerLSEfficacy and safety of besifloxacin ophthalmic suspension 0.6% compared with moxifloxacin ophthalmic solution 0.5% for treating bacterial conjunctivitisOphthalmology200911691615162319643483
- Antibiotic/Antimicrobial Resistance: Clinical guidelinesAvailable at: http://www.cdc.gov/DRUGRESISTANCE/clinical.htm Accessed Dec. 5, 2008.
- World Health Organization Antimicrobial resistance. Available at: http://www.who.int/mediacentre/factsheets/fs194/en/print.html 2002 Fact sheet 194 Accessed Dec. 5, 2008.
- YoneyamaHKatsumataRAntibiotic resistance in bacteria and its future for novel antibiotic developmentBiosci Biotechnol Biochem20067051060107516717405