Abstract
Insomnia is a leading cause of sleep disturbance in primary care practice affecting >30% of people in the United States and can result in psychological and physiological consequences. We aim for a focused discussion of some of the underpinnings of insomnia and practical tips for management (eg, algorithms). A PubMed search was conducted using English language papers between 1997–2007, with the terms “sleep,” “insomnia”; “primary care” and “clinics”; “comorbid conditions”; “treatment” and “management.” Sleep, psychiatric and medical disorders significantly affect sleep, causing patient suffering, potentially worsening of other disorders and increasing the use of primary care services. We provide an outline for practical assessment and treatment of insomnia in primary care, including the strengths and weaknesses of medications.
Introduction
Insomnia, defined as difficulty initiating and maintaining sleep, is the most common sleep disorder in the United States (US).Citation1 About one-third of the adult population in the US experience insomnia at some point in their lives,Citation2 and is a persistent problem in approximately 10% of US adults.Citation3,Citation4 The prevalence of insomnia increases with age, and is more common in women than in men.Citation5 Lower socioeconomic status, divorce, widowhood, separation, recent life stressors, depression, and substance abuse increase the risk of insomnia.Citation6,Citation7 Insomnia has also been independently associated with worse health-related quality of life in outpatients at family medicine, internal medicine, endocrinology, cardiology, and psychiatry clinics.Citation3,Citation8,Citation9 Women are twice as likely to suffer from insomnia than men, due to bodily changes (eg, pregnancy, menopause), or perhaps as some of the social factors (eg, unemployed or divorced) may be more common in women.Citation4
Unfortunately, many primary care patients often have insomnia and may additionally complain of early awakening and nonrestorative sleep.Citation2 This can result in numerous physical and psychological consequences, including medical (eg, blunted hypothalamic-pituitary-adrenal axis, and impaired host defenses) and psychiatric (eg, anxiety and mood, and cognitive) disorders.Citation2
Normal sleep architecture refers to a characteristic pattern of sleep and consists of two major stages, nonrapid eye movement (NREM; comprises 75%–80% of total sleep) and rapid eye movement (REM). Normal adult sleep begins with NREM and alternates between NREM and REM every 90 minutes. Normal sleep latency is approximately 10–20 min and total sleep time (TST) averages 6–9 hours. NREM sleep is characterized by relatively quiescent brain activity, decreased metabolic rate, and slow-wave sleep, which are theorized to be necessary for physiologic restoration. Sleep is greatest when very young and least when old.
The etiology of sleep disruption is multi-factorial and includes the patient’s underlying illness(es), medical treatments, and biopsychosocial factors. The goals of this paper are: 1) to discuss factors that lead to insomnia in medical patients, 2) to provide a practical approach for working up insomnia, and 3) to offer principles and algorithms to guide management of insomnia.
Factors affecting sleep
Insomnia and other sleep disorders are caused by: medical, neurological, pain, and psychiatric disorders. In addition, medications and environmental factors can cause insomnia. Finally, conversely, sleep disorders can worsen medical conditions. This section provides an overview of these interactions.
General medical disorders
Causes of insomnia include sleep disordered breathing (SBD), congestive heart failure (CHF), diabetes mellitus, thyroid disorders, chronic obstructive pulmonary disease (COPD), gastroesophageal reflux (GER), cardiovascular disease, and renal disease.Citation10
Problems such as frequent nocturnal awakenings in patients with congestive heart failure (CHF) may be related to orthopnea or paroxysmal nocturnal dyspnea, or may reflect undiagnosed SDB problems such as obstructive sleep apnea (OSA) or Cheyne–Stokes Breathing (CSB). Treatment of CSB with CPAP seems to improve sleep quality and ejection fraction in patients with CHF.Citation11
Patients with COPD have decreased total sleep times (TST), SWS, and REM sleep.Citation10 Shortness of breath, nocturnal cough, and wheezing worsen sleep.Citation12 This leads to fatigue and sleep deprivation, which undermine the work of breathing and impair gas exchange. Airflow obstruction tends to worsen in the early morning hours in patients with COPD and asthma and may be related to REM effect on the diaphragm.
Approximately 50% of patients with chronic end-stage renal disease have insomnia and other sleep disorders.Citation13 Patients complain of restless leg syndrome, periodic limb movement disorder, bone pain, nausea and pruritis. The etiology of sleep disorders appears to be related to metabolic derangements associated with renal disease or from co-existing diabetes.
Endocrine disorders
Endocrine disorders have also been associated with sleep disruption. Studies suggest that patients with diabetes mellitus (DM) have decreased TST and impaired sleep quality secondaryCitation14 to nocturia and neuropathic pain.Citation15 There is accumulating evidence that poor sleep impairs glucose metabolic control. Inadequate quality or quantity of sleep is shown to be a risk factor for developing type 2 diabetes in large prospective studies, and predicted increased levels of HbA1c in type 2 diabetics.Citation16
Neurological disorders
Since the brain and its various systems are critical in regulating sleep and wakefulness, patients with neurologic disorders have an increased risk of developing sleep disorders. Patients with dementia, other neurodegenerative disorders (eg, Parkinson’s), epilepsy, and traumatic brain injury (TBI) have a higher prevalence of sleep disturbance and sleep disorders.Citation17 Post-stroke patients can develop insomnia or hypersomnia, which is a reduction in sleep latency, increased sleep, or excessive daytime sleepiness. Brain-injured patients are also susceptible to sleep problems, with incidences as high as 72.7% in the hospital (mostly sleep initiation and maintenance) and 51.9% in the community (mostly excessive somnolence);Citation18 many with circadian rhythm sleep disorders (CRSD).
Pain
Between 50% and 70% of patients with chronic pain complain of impaired sleep.Citation19 Sleep disruption is so common in fibromyalgia (75%) that it is considered to be a key diagnostic symptom.Citation20 In burn patients, pain was associated with increased intermittent awakenings, prolonged periods of wake time, poor pain tolerance, and complaints of higher pain intensity the following day.Citation21 Pain increases cortical arousals and awakening, and sleep deprivation increases pain sensitivity and vulnerability to pain by inhibiting opioid protein synthesis and/or reducing opioid receptor affinity.Citation21
Women’s health
Women have a higher rate of insomnia than men, nearly 2:1 in one survey.Citation4 Psychosocial risk factors may be higher in women and they also contest with significant changes during pregnancy. Peri- and post-menopausal changes (eg, nocturia, hot flashes) affect many women,Citation22 though ageing associated with such change may account for differences compared to pre-menopausal women.Citation23
Psychiatric disorders
Sleep problems are so common in psychiatric conditions that insomnia is listed as a symptom for mood (eg, manic or depressive), anxiety, and substance abuse disorders. Sleep disturbance in patients with undiagnosed psychiatric disorders may alert primary care providers to these problems. In a survey of 200 general medical patients in a hospital, 112 (56.5%) complained of insomnia and 100 (50%) met criteria for at least one psychiatric disorder – only 1.5% of those were charted – with depression most common at 35%.Citation24 The results showed that patients with insomnia had 3.6 times higher risk of having depression than those without insomnia.
An outpatient survey noted that chronic insomnia patients were 40 times more likely to have depression and six times more likely to have an anxiety disorder compared to those without insomnia.Citation6 Longitudinal studies link prior insomnia with 2- to 5-times increased risk of mood and anxiety disorders and suicide.Citation25
An estimated 65% with major depression have difficulty falling asleep, frequent awakenings, or early morning awakenings.Citation26 Three patterns of sleep architecture abnormalities have been observed in patients with major depression: 1) sleep continuity disturbances characterized by prolonged sleep-onset, increased wake time during sleep, increased early morning wake time, and decreased total sleep time; 2) decreased proportion and length of SWS; and 3) REM sleep abnormalities such as reduced time to REM sleep, prolonged first REM sleep period, and increased REM sleep percentage.Citation26
Medications affecting sleep
Sedatives and opioids may help with sleep onset, but actually impair sleep architecture (). Hypnotic agents with a significant anticholinergic component, such as diphenhydramine, are particularly prone to decrease cognitive performance and may precipitate frank delirium. Hypnotics are often prescribed and mainly work for initial insomnia, but can sometimes worsen sleep. Similarly, benzodiazepines can be problematic, particularly in older patients by causing motor impairment and increasing risk for delirium. Other common offenders are anti-hypertensives, antihistamines, corticosteroids, antiepileptics, beta antagonists (particularly lipophilic ones like propranolol and timolol) decrease REM sleep and increase nightmares and insomnia, anabolic steroids and bronchodilator therapy.
Table 1 Drugs that affect sleep: Mechanisms and clinical implications
Table 2 Food and drug administration-approved drugs for insomnia
Medications used to treat common medical and psychiatric illnesses can also disrupt sleep (see ). These include selective serotonin reuptake inhibitors (SSRIs), monoamine oxidase inhibitors (MAOIs), and tri- and tetracyclic agents (TCAs).
Environmental factors
Many hospitals have difficulty adhering to the World Health Organization’s recommendation of keeping noise level to ≤35 dB in hospital rooms, particularly intensive care units (ICUs), daytime peaks up to 150–200 dB and nighttime peaks >80 dB. By comparison, a running vacuum cleaner is about 80 dB. It follows, then, that residences, hotels and apartments have varying dB levels, often affecting sleep. Irregular sleep schedules, parenting young children and nighttime bathroom trips are common for many.
Circadian rhythm sleep disorders are disorders that are related to the timing of sleep within the 24-hour day. They include time-zone change syndrome (ie, jet lag), shift work sleep disorder, irregular sleep-wake pattern, delayed or advanced sleep phase syndromes, and non-24-hour sleep-wake disorder. Some of these disorders are influenced by an individual’s control (eg, shift work or time zone change) or secondary to disorders of neurological mechanisms (eg, irregular sleep-wake pattern and advanced sleep phase syndrome).
Affect of sleep disorders on medical disorders
Data is mounting that primary sleep disorders, such as sleep disordered breathing (SDB), disturb sleep and exacerbate the pathophysiology associated with certain disease processes. Additionally, medical disease may directly impair sleep physiology leading to a cyclical interaction (eg, OSA leads to impaired sleep and increased heart rate and blood pressure, which then increases CHF, which leads to impaired sleep). OSA is a common sleep disorder, and pertinent in this discussion as a chronic cause of sleep maintenance insomnia. It is characterized by complete or partial pharyngeal obstruction that leads to apnea, snoring, choking and daytime somnolence.Citation27 SBD has been independently associated with cardiovascular diseases such as hypertension, heart failure, ischemic heart disease, atrial fibrillation, and cerebrovascular disease.Citation28
Assessment and evaluation of sleep
History
Analysis of sleep problems requires a focused, systematic assessment of potential factors that cause fragmented or interrupted sleep, as related by the patient and family. The history, physical examination and diagnostic tests yield important clues. Just as clinicians use pain as a clue to underlying illnesses, the practitioner should use insomnia to investigate for a cause, rather than immediately prescribing treatment ().
Figure 1 Overview of assessment and treatment of insomnia in primary care.
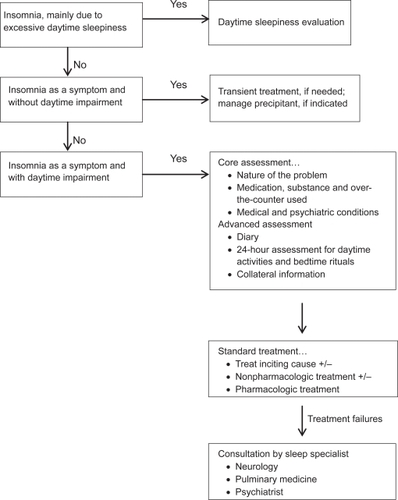
First and foremost, gaining an initial sense of acute vs chronic complaints will help guide the nature, depth, and breadth of a focused interview about insomnia and its differential. Acute insomnia may last from a single night to several weeks (stress, changes in schedule and time zone changes) may not require treatment. Mild insomnia often can be prevented or cured by practicing good sleep habits (see below). If the insomnia interferes with daily function because the patient is sleepy and tired, more investigation may be required, and sleeping pills may be indicated short- and long-term. Treatment for chronic insomnia includes first treating any underlying conditions or health problems that are causing the insomnia. Sleep habits, behavioral approaches and medications may be helpful.
Specific questions in the history to determine the exact nature of the complaint include:
Do you have problems falling asleep or staying asleep?
Do you frequently awaken, and is that associated with anything (eg, pain)?
Do you awaken tired or unrefreshed despite many hours of sleep?
What time do you go to bed and get up?
Is the insomnia related to any new habits lately (eg, travelling) or adjustments in day-night changes (eg, new shift at work)?
What activities do you normally have throughout the day?
Have there been any recent changes in your routine or health?
When going to sleep, how anxious are you or how mentally aroused are you?
The simplest method to ascertain the patient’s routine is to have him/her describe a typical day. Patients’ routines may be severely disrupted during illness or stress. Staying in bed for prolonged periods and sleeping during the day can impair nighttime sleep.
Chronic insomnia may require a personal or family history of over-the-counter medication, substance disorders, primary sleep disorders (eg, OSA, restless leg syndrome) or symptoms of common sleep problems.
Do you snore when you sleep? If so, how often? Do family members complain that you snore very loudly? Does drinking alcohol before sleep worsen the snoring?
Has anyone noticed that you appear to “stop breathing” while asleep?
Have you recently increased or decreased the amount of alcohol you drink? By how much, and over what period of time?
Do you use cocaine, methamphetamine, “speed,” or other substances?
Do you smoke? If so, when?
Patients may have underlying sleep and psychiatric disorders that they are unaware of, insufficiently diagnosed or simply forgotten when feeling ill. For example, OSA is often undiagnosed and may present with hypersomnlence or insomnia, exacerbated by illness. Snoring may be dismissed as insignificant or “normal” especially in male patients. Additional medical and psychiatric history should be obtained for anxiety, depression, substance and psychotic disorders. Alcohol and drug use can have profound effects on sleep, with the former normally suppressing REM sleep.
On more difficult patients, the provider can consider the following:
24-hour assessment of activities
Diary logging daily activities and sleep patterns by the patient over 7–30 days
Collateral information
Physical examination
Key issues on the physical examination include vital signs, signs of a medical condition (eg, obesity), changes from the last clinic visit, stigmata of substance use and mental status changes (mood, cognition, physical appearance).
Diagnostic tests and procedures
Primary care providers rarely order more advanced tests, instead deferring first to a consultation from neurology, pulmonology, psychiatry or other sleep specialists. Sleep is identified and quantified by polysomnography (PSG), but it is not that useful on most chronic insomnia patients. It may be useful with sleep apnea, periodic limb movements or parasomnias. Actigraphy is an objective means to assess rest activity patterns, by using a motion-sensitive bracelet on the non-dominant hand.
Management strategy to improve sleep in primary care patients
Optimizing sleep for patients includes nonpharmacological and pharmacological interventions. It is best not to assume that patients know or practice good sleep habits, or have regular sleep cycles. Those with a significant evidence base are noted with a * (some data) or ** (significant and/or high quality data).
Nonpharmacologic interventions
Reduce nocturnal discomfort
○ Maximize pain management
○ For patients with GER: No PO after 8PM and keep head of bed elevated
Minimize iatrogenic insomnia
○ Avoid benzodiazepines for sleep (unless withdrawal state)
○ Avoid starting multiple medications and discontinue nonessential medications
○ Change medication regimens to promote sleep (eg, give “activating” medications in the morning and sedating medications to the evening)
○ Minimize opiates, antihistamines and anticholinergic agents
○ Avoid night-time diuretics whenever possible
○ Optimize nighttime glycemic control
Promote good sleep hygiene
○ No caffeine after 6 PM
○ Appropriate lighting and same time to bed
○ Encourage regular nocturnal sleep time, and discourage naps during the day
○ Meditation, yoga and/or relaxation training as a ritual and/or to reduce tension and anxiety
Exercise at least 3X/week before 6 PM
Improve the environment
○ Provide adequate day and night lighting
○ Offer sleep masks or ear plugs, if appropriate.
Short- or long-term customized lifestyle planning
○ May be pertinent to sleep-wake cycle disorders
○ Targets emotional, cognitive and physical manifestations
○ May be used with pharmacotherapy (eg, melatonin agents) (Renger 2008)
Cognitive behavioral therapy (CBT)
A number of randomized clinical trials have been done with CBT, showing great promise in primary and secondary insomnias, with 1–4 sessions (often biweekly) having short- and long-term effect.Citation29 Of interest is whether or not sedative hypnotics need to be discontinued for a CBT treatment, though in one study with clinical scales and most polysomnographic measures, CBT was highly effective with or without sedative-hypnotic cessation. It produced the greatest changes in total sleep time, REM sleep and sleep efficiency.Citation30 Finally, nurse-administered CBT has also been shown to be effective, which may have major implications for primary care practice.Citation31
Pharmacologic treatment
Pharmacologic treatment, if necessary, complements the nonpharmacologic interventions. The clinician must:
Decide on medications’ likelihood of efficacy, side effects, and risks
Find a fit between the patient, the type(s) of insomnia and the medication
Consider Food and Drug Administration (FDA) indications (and contraindications), evidence base and off-label uses
Choose a mechanism(s) of action in light of gamma-aminobutyric acid, histamine, serotonin, melatonin, adenosine, corticotrophin-releasing factor and other systems being targeted
Medication options
(* = open or small sample data, vs** = short-term, controlled data) vs*** = short- and long-term controlled data)
Medication options include the benzodiazepine GABAA receptor agonists (BzRAs)**, nonbenzodiazepine GABAA receptor agonists (non-BzRAs)**–***, melatonin-receptor agonists**, antidepressants (ADs)*, atypical antipsychotics (APs)* and other medications*.Citation32 The latter three groups are not FDA-approved for insomnia, but are commonly used. Suggestions for medication selection are based on the diagnosis, the evidence base and strength and weaknesses of the medications ( and ).
Figure 2 Pharmacologic treatment algorithm for insomnia in primary care.
Abbreviations: BzRAs, benzodiazepines; Non-BzRAs, nonbenzodiazepines; OSA, obstructive sleep apnea.
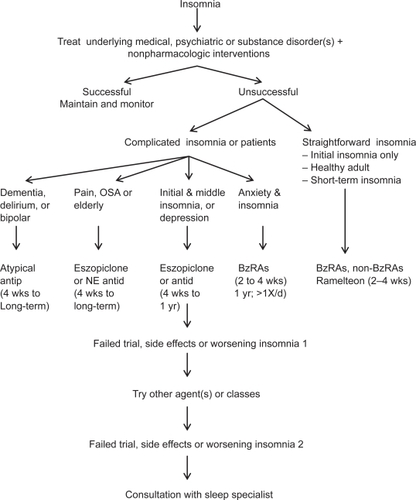
The FDA has approved three classes of medications for the treatment of insomnia: BzRAs, non-BzRAs and melatonin-receptor agonists.Citation33 The number of comparison studies is limited, but the available data reveal that: 1) zolpidem (Ambien) may be better than temazepam (Restoril) in terms of sleep latency and quality; and 2) zaleplon (Sonata) may lead to a shorter sleep latency than zolpidem (Ambien), but the latter has longer sleep duration.Citation34
BzRAs include estazolam, flurazepam, quazepam, temazepam, and triazolam. Though BzRAs decrease sleep latency and increase total sleep time, they also have adverse side effects such as anterograde amnesia, daytime sedation, cognitive impairment, poor motor coordination, dependence, tolerance, and rebound insomnia.Citation6 Due to these side effects, BzRAs should be limited to generally healthy, young (eg, <45 years old) patients with initial insomnia and who are expected to have brief medication trials. BzRAs should be avoided in patients with a history of substance abuse, elderly patients, and others with a particularly high risk for falls or delirium (eg, traumatic brain injuries, strokes, multiple new medications).
Non-BzRAs seem to have a superior side effect profile when compared to BzRAs. Non-BzRAs include eszopiclone (Lunesta), zaleplon (Sonata), zolpidem (Ambien), and zolpidem extended-release. They have less next-day sedation, psychomotor dysfunction, or tolerance/withdrawal; less REM rebound; and lower abuse potential than BzRAs.Citation34 Studies have included short-term effects for insomnia,Citation34–Citation36 short-term effect in comorbid medical and psychiatric disorders (eszopiclone)Citation37* and long-term effects (eszopiclone;Citation38 zolpidem extended-releaseCitation39)***. The sole melatonin-receptor agonist, ramelteon (Rozerem), also reduces time to fall asleep without next-day psychomotor and memory effects*.Citation40 Ramelteon is believed to target receptors melatonin 1 and 2 receptors located in the brain’s suprachiasmatic nucleus to stabilize circadian rhythms and stabilize the sleep-wake cycle.Citation41
Limited data exist on the efficacy of non-FDA approved medications such as ADs and APs for insomnia.Citation42 Sedating antidepressants that may be useful for some hospitalized patients, include trazodone (Desyrel) and mirtazapine (Remeron). Trazodone and mirtazepine are used most noticeably, though the former is associated with priapism in approximately 1:10,000 males. They may be an acceptable short-term alternative to BzRAs, but data are limited on them and recommended duration of use is unclear. Short-term studies have shown that low-dose trazodone (50 mg) is less efficacious than zolpidem. Mirtazapine, which promotes both sleep and appetite, may be particularly helpful for patients with cancer, AIDS and other conditions in which the trio of poor sleep, anorexia, and depression are common. Although sedating, tricyclic antidepressants (TCAs) are not recommended to such patients because they increase the risk of cardiac conduction abnormalities, reduce the seizure threshold, and have significant anticholinergic effects.
Antipsychotics are not routinely used first-line for the treatment of insomnia, except in patients who are in the midst of acute manic or psychotic episodes.Citation43 They typically increase sleep continuity and do not affect sleep architecture much. Sedating APs include risperidone (Risperdal; 0.5–2 mg HS), olanzapine (Zyprexa; 2.5–10 mg HS), quetiapine (Seroquel 12.5–300 mg HS); ziprasidone (Geodon) and aripiprazole (Abilify) are not usually sedating. Delirious patients or elderly patients with dementia who have nightly episodes of confusion, agitation, and cognitive decline (“sun-downing”) may benefit from a low dose of a sedating AP to promote sleep and to prevent or treat these episodes. Common side effects include sedation, weight gain and metabolic changes (glucose, cholesterol, lipids). Rare, but important side effects, include neuroleptic malignant syndrome (a triad of mental status changes, increased muscle tone and autonomic hyperactivity), tardive dyskinesia, and akithisia (restlessness or inability to sit still).
The administration of antihistamines, barbiturates, chloral hydrate, and alternative/herbal therapies has been discouraged in recent years, since the benefits rarely outweigh the risks associated with their use. In the US, antihistamines such as diphenhydramine are the most commonly used over the counter agent for chronic insomnia.Citation2 However, anticholinergic action of antihistamines may lead to orthostatic hypotension, and induce delirium in vulnerable patients, especially the elderly, and should be avoided if possible.
Conclusion
Sleep, medical and psychiatric disorders significantly affect sleep in primary care patients, as do some medical treatments. More research is needed to evaluate if/how screening, education, and good habits help patients, with or without medication. Medications have strengths and weaknesses that need to be considered in the process of selection. Algorithms for diagnosis and management may serve as practical guides for primary care providers. More research is needed on the treatment of insomnia in primary care practice.
Disclosure
The authors report no conflicts of interest in this work.
References
- International Classification of Sleep DisordersAmerican Academy of Sleep Medicine, One Westbrook Corporate CenterWestchester, IL, 60154, 2001
- National Institute of HealthNIH state-of-the-science conference statement on manifestations and management of chronic insomnia in adultsNIH Consens Stat Sci Statements200522130
- KatzDAMcHorneyCAThe relationship between insomnia and health-related quality of life in patients with chronic illnessJ Fam Pract20025122923511978233
- National Sleep Foundation2005Cited Oct 6, 2008. Available from: http://www.sleepfoundation.org
- BliwiseDLReview: Sleep in normal aging and dementiaSleep19931640818456235
- FordDEKamerowDBEpidmiologic study of sleep disturbances and psychiatric disorders: An opportunity for preventionJAMA1989262147914842769898
- ZorickFJEvaluation and management of insomnia: An overviewKrygerMHRothTDementWCPrinciples and Practice of Sleep Medicine3rd EdPhiladephiaW.B. Saunders Company2000615616
- RichardsonGUpdate on the science, diagnosis and management of insomniaLondonRoyal Society of Medicine Press Ltd, International Congress and Symposium Series; 2006262
- BaHammanASleep in acute care unitsSleep Breath20061061516435158
- BallardRDSleep and medical disordersPrim Care Clin Office Pract200535511533
- BerryRBHardingSMSleep and medical disordersMed Clin N Am20048867970315087211
- MohseninVSleep in chronic obstructive pulmonary diseaseSleep Med Clin2007218
- HanlyPSleep disorders and end-stage renal diseaseSleep Med Clin200725966
- GislasonTAlmqvistMSomatic diseases and sleep complaints: An epidemiologic study of 3,201 Swedish menActa Med Scand19872214754813496735
- LamondNTiggermannMDawsonDFactors predicting sleep disruption in type II diabetesSleep20002341541610811386
- YaggiHKAraujoABMcKinlayJBSleep duration as a risk factor for the development of type 2 diabetesDiabetes Care20062965766116505522
- HoytBDSleep in patients with neurologic and psychiatric disordersPrim Care Clin Off Pract200532535548
- FichtenbergNLZafonteRDPutnamSMannNRMillardAEInsomnia in a post-acute brain injury sampleBrain Inj20021619720611874613
- BarcziSRJuergensTM2006Comorbidities: Psychiatric, medical, medications, and substancesSleep Med Clin20061231245
- LinebergerMDMeansJKEdingerJDSleep disturbance and fibromyalgiaSleep Med Clin200723139
- RaymondIAncoli-IsraelSChoiniereMSleep disturbances, pain and analgesia in adults hospitalized for burn injuriesSleep Med2004555155915511701
- United States Health and Human ServicesFrequently asked questions. 2008. Cited Oct 6, 2008. Available from: http://www.4woman.gov/FAQ/insomnia.htm
- KalleinenNPolo-KantolaPHimanenSLSleep and the menopause - do postmenopausal women experience worse sleep than premenopausal women?Menopause Int2008149710418714074
- RochaFLHaraCRodriguezCVIs insomnia a marker for psychiatric disorders in general hospitalsSleep Med2005654955315994126
- WeissmanMMGreenwaldSNino-MurciaGThe morbidity of insomnia uncomplicated by psychiatric disordersGen Hosp Psych199719245250
- PetersonMJBencaRMSleep in mood disordersPsychiatr Clin N Am20062910091032
- BassiriAGGuilleminaultCClinical features and evaluation of obstructive sleep apnea-hypopnea syndromeKrygerMHRothTDementWCPrinciples and Practice of Sleep Medicine3rd EdPhiladephiaW.B. Saunders Company2000869872
- WattanakitEBolandLPunjabiNMRelation of sleep-disordered breathing to carotid plaque and intima-media thicknessAtherosclerosisIn press.
- EdingerJDWohlgemuthWKRadtkeRADose-response effects of cognitive-behavioral insomnia therapy: a randomized clinical trialSleep20073020321217326546
- ZavesickaLBrunovskyMMatousekMDiscontinuation of hypnotics during cognitive behavioural therapy for insomniaBMC Psychiatry200888018801160
- EspieCAMacMahonKMKellyHLRandomized clinical effectiveness trial of nurse-administered small-group cognitive behavior therapy for persistent insomnia in general practiceSleep20073057458417552372
- GreenBTBroughtonWAO’ConnorJBMarked improvement in nocturnal gastroesophageal reflux in a large cohort of patients with obstructive sleep apneaArch Intern Med2003163414512523915
- NeubauerDBState-of-the-art sleep management. Awakening insomnia managementProceedings from a satellite symposium at SLEEP 2006: 20th Anniversary Meeting of the Associated Professional Sleep SocietiesSalt Lake City, UTJune 20. 2006612
- DundarYBolandAStroblJNewer hypnotic drugs for the short-term management of insomnia: A systematic review and economic evaluationHealth Tech Ass200419305322
- PagelJFMedications and their effect on sleepPrim Care Clin Off Pract200532401509
- ErmanMKZammitGRubensRA polysomnographic placebo-controlled evaluation of the efficacy and safety of eszopiclone relative to placebo and zolpidem in the treatment of primary insomniaJ Clin Sleep Med2008422923418595435
- PollackMKinrysGKrystalAEszopiclone coadministered with escitalopram in patients with insomnia and comorbid generalized anxiety disorderArch Gen Psychiatry20086555156218458207
- WalshJKKrystalADAmatoDANightly treatment of primary insomnia with eszopiclone for six months: effect on sleep, quality of life, and work limitationsSleep20073095996817702264
- KrystalADErmanMZammitGKLong-term efficacy and safety of zolpidem extended-release 12.5 mg, administered 3 to 7 nights per week for 24 weeks, in patients with chronic primary insomnia: a 6-month, randomized, double-blind, placebo-controlled, parallel-group, multicenter studySleep200831799018220081
- ErmanMSeidenDZammitGAn efficacy, safety, and dose-response study of Ramelteon in patients with chronic primary insomniaSleep Med20067172416309958
- TurekFWGilletteMUMelatonin, sleep, and circadian rhythms: Rationale for development of specific melatonin agonistsSleep Med2004552353215511698
- InfanteMBencaRTreatment of insomniaPrimary Psychiatry2005124756
- HiltyDMLeamonMLLimRFDiagnosis and treatment of bipolar disorder in the primary care settingPrimary Psychiatry2006137785