Abstract
T-cell malignancies have distinct biochemical, immunologic, and clinical features which set them apart from non-T-cell malignancies. In the past, T-cell leukemia portended a worse prognosis than leukemia of B-cell origin. Cure rates have improved with intensification of therapy and advanced understanding of the molecular genetics of T-cell malignancies. Further advances in the treatment of T-cell leukemia will require the development of novel agents that can target specific malignancies without a significant increase in toxicity. Nelarabine (2-amino-9β-D-arabinosyl-6-methoxy-9H-guanine), a synthesized guanosine nucleoside prodrug of ara-G (9-β-D-arabinofuranosylguanine), recently received accelerated approval by the U.S. Food and Drug Administration (FDA) for the treatment of relapsed/refractory T-ALL and T-LBL in adults and children. Nelarabine is water soluble and rapidly converted to ara-G, which is specifically cytotoxic to T-lymphocytes and T-lymphoblastoid cells. Clinical and pharmacokinetic investigations have established that nelarabine is active as a single agent which has led to exploration of an expanded role in the treatment of T-cell hematologic malignances.
Background
The cure rate for acute lymphoblastic leukemia (ALL) has steadily increased since the 1960’s, with the first success coming in the pediatric population (CitationSmith et al 1996; CitationGaynon et al 2000; CitationConter et al 2000; CitationPui et al 2004). With contemporary therapy, the 5-year event-free survival rate (EFS) is approximately 80% for children and 40% for adults (CitationPui et al 1998, Citation2003). Advances in supportive care, precise risk assessment, intensification of therapy, and advances in understanding the molecular genetics of leukemia cells have led to an improved outcome. T-cell lymphoid malignancies have distinct biochemical, immunologic, and clinical features which set them apart from non-T-cell malignancies (CitationCrist et al 1988; CitationGarrand et al 1990; CitationBash et al 1993; CitationUckun et al 1998). For example, the observation that T-cell lineage blasts form fewer methotrexate polyglutamates than that of B-cell blasts has led to the intensification of methotrexate for optimal response (CitationPui et al 2002). Advances such as these, along with the introduction of high-dose, multi-agent pulse chemotherapy, have significantly improved the EFS of children with T-cell ALL (T-ALL) from 15%–20% three decades ago to approximately 75% on the most recent published regimens (CitationReiter et al 1994; CitationSchorin et al 1994). Despite intensification of therapy, the EFS rates seem to have plateaued, suggesting that further intensification of existing treatments is unlikely to substantially improve outcome. In addition, high dose chemotherapy leaves patients with an increased risk of treatment-related toxicity, long term sequelae, and secondary malignancies. Therefore, the development of novel agents with improved efficacy and safety profiles will be important to advance survival in patients with T-cell malignancies. With the proven efficacy of antimetabolites such as methotrexate and cytarabine in treatment regimens for T-ALL and T-cell lymphoblastic lymphoma (T-LBL), the development of purine nucleoside analogs with preferential cytotoxicity toward T-lymphocytes may be a promising strategy. Nelarabine (2-amino-9β-D-arabinosyl-6-methoxy-9H-guanine, compound GW506U78), a prodrug of ara-G (9-β-D-arabinofuranosylguanine), has been recently approved by the US Food and Drug Administration (FDA) for the treatment of relapsed/refractory T-ALL and T-LBL in adults and children (CitationCohen et al 2006). This paper will review the development of nelarabine, including the chemistry, pharmacology, and clinical data of this promising new agent.
Mechanism of action/chemistry
Nucleoside analogs, such as cytarabine, are prodrugs that are converted to their active triphosphate form by a series of enzymatic phosphorylation steps and then incorporated into DNA (CitationMomparler et al 1968; CitationRodriguez et al 2002). These agents have proven highly effective in the treatment of hematologic malignancies, including T-ALL and T-LBL. In particular, guanine nucleoside analogs generated clinical interest after the discovery that a genetic deficiency of purine nucleoside phosphorylase (PNP) results in a profound T-cell lymphopenia (CitationGiblett et al 1975). PNP is a ubiquitous enzyme that, when deficient, leads to a dysfunction of the purine salvage pathway and thus elevated plasma deoxyguanosine (dGuo) and an intracellular accumulation of its deoxyguanosine triphosphate (dGTP) (CitationGiblett et al 1975; CitationCohen et al 1978). Models of PNP deficiency further revealed that ara-G was specifically toxic to T-lymphocytes and T-lymphoblastoid cells, whereas B-lymphocytes did not accumulate high levels of dGTP and were less sensitive to deoxyguanosine (CitationMitchell et al 1978; CitationOsborne et al 1983; CitationFairbanks et al 1990). Despite this T-cell specificity, the clinical use of the deoxyguanosine analog ara-G was limited because of the poor solubility of the compound (CitationCohen 1983). However, investigators developed the 6-methoxy prodrug of ara-G, nelarabine, that is 10 times more water soluble than previous ara-G preparations (CitationLambe et al 1995). Nelarabine is a substrate for adenosine deaminase which converts the prodrug to ara-G (). Ara-G is transported into T-lymphoblastoid cells by two facilitative nucleoside transport systems that differ in their sensitivity to inhibition by nitrobezylthioinosine (CitationPrus et al 1990). However, this inhibition is not the rate-limiting step of its cellular metabolism. Rather, it is the initial conversion to its monophosphate form (ara-GMP) by both deoxycytidine kinase (dCyd) and dGuo kinase (CitationRodriguez et al 2002). Ara-GTP subsequently competes with dGTP in leukemia blasts for incorporation into DNA (CitationGandhi et al 1995). The incorporation of ara-GTP into DNA inhibits DNA synthesis, resulting in chain termination and apoptosis (CitationRodriguez et al 1999). In addition, T-cell selective cytoxicity investigations reveal that in addition to a higher accumulation of ara-GTP in T-cells, the induction of the Fas-mediated cell death pathway further enhances T-cell kill. (CitationRodriguez et al 2003). With the development of this ara-G prodrug, investigation into the T-cell cytotoxicity of this agent moved forward. Details of recent clinical investigations of nelarabine are shown in .
Figure 1 Conversion of nelarabine to ara-G by adenosine deaminase.
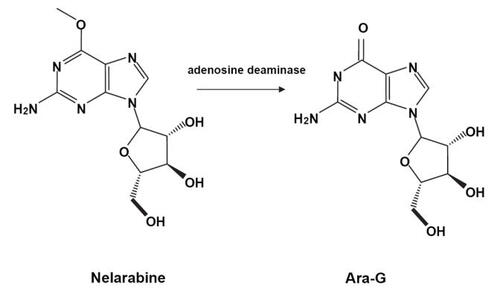
Table 1 Clinical trials of nelarabine
Clinical evaluation
Based on the favorable chemical and mechanistic properties of nelarabine, the initial Phase I clinical trial was conducted on 93 adults and children with refractory hematologic malignancies (CitationKurtzberg et al 2005). Nelarabine was administered daily as a 1-hour infusion for 5 days. Dose levels ranged from 5 mg/kg to 75 mg/kg. The maximum tolerated dose (MTD) was determined to be 40 mg/kg and 60 mg/kg daily for 5 days in adult and pediatric patients, respectively. Of the 93 patients enrolled, 39 were diagnosed with malignancies of the T lymphoid lineages (T-ALL and T-LBL). Twenty-three percent (9) of patients with T-ALL/T-LBL achieved a complete response (CR), and 31% (12) achieved a partial response (PR). Of these responders, 71% had at least 2 prior relapses and 48% had failed stem cell transplant (SCT). Consistent with preclinical investigations, the dose limiting toxicity (DLT) of nelarabine was neurotoxicity. Half the children and 85% of adults enrolled on the initial Phase I study experienced reversible neurotoxicity including weakness, ataxia, and confusion. Transient somnolence, malaise and fatigue beginning at 6–8 days after therapy were reported most frequently, mainly in adults. Coma was observed in 3 of 4 adults and 1 child at the 60 mg/kg dose level (approximately 1.8 g/m2) and 2 of 31 adults treated at the 40 mg/kg dose level. No neurotoxicity was observed in children at the 40 mg/kg dose level (approximately 1.2 g/m2). Both ataxia (2 children, 5 adults) and gait disorder (0 children, 12 adults) are neurologic events that may be reflective of cerebellar toxicity. Other cerebellar events, such as tremors or dysmetria, are not mentioned by the authors. These neurologic events are of particular interest as other purine nucleoside analogs such as fludarabine, especially when combined with cytarabine, have been associated with specific cerebellar toxicity (CitationVidarsson et al 2001). A more thorough review of the neurotoxcicity of compound 506U in both adults and children as presented to the FDA can be found in and .
Table 2 Nelarabine neurological toxicity in adult patients (n = 103) as presented to the FDA Oncology Drugs Advisory Committee
Table 3 Nelarabine neurological toxicity data in pediatric patients (n = 84) as presented to the FDA Oncology Drugs Advisory Committee
After the Phase I trial demonstrated the potential of nelarabine in T-cell malignancies, a pediatric Phase II trial of nelarabine was conducted by the Children’s Oncology Group (COG) (CitationBerg et al 2005). The trial accrued 153 patients less than 21 years of age with recurrent or refractory T-ALL and T-LBL. Patients were stratified depending on the site of relapse and number of prior relapses. The strata were as follows: stratum 1:≥25% bone marrow blasts in first relapse; stratum 2: ≥25% blasts in ≥ second relapse; stratum 3: positive CSF; stratum 4: extramedullary (non-CNS) relapse. Nelarabine was initially administered at a dose of 1.2 g/m2 IV over I hour daily for 5 days. Because of grade 4 neurotoxicity at this dose level, the dose was de-escalated twice to a final dose of 650 mg/m2/day for 5 days. In addition, because it seemed likely that the nelarabine dose would be lower in future studies in combination with other cytotoxic agents, the doses for patients in stratum 3 and stratum 4 were reduced to 400 mg/m2. Patients in stratum 1 had an overall response rate of 55%, with 16 CRs and 2 PRs. Patients in stratum 2 had an overall response rate of 27%, with 7 CRs and 1 PR. Of 21 assessable patients in stratum 3, the overall response rate was 33% with 5 CRs and 2 PRs. Patients in stratum 4 had an overall response rate of 14%, with no CR’s. Eighteen patients in this study experienced ≥ Grade 3 neurologic side effects, the most common being reversible somnolence and peripheral neuropathy manifested by weakness, numbness, and/or paresthesias, predominantly in the lower extremities. Other than lower extremity weakness, there is no specific report of cerebellar toxicity in this study. The authors of this study reason that this difference in response rate between patients in first relapse versus subsequent relapse may be due to the amount of previous therapy and resultant resistant disease, and therefore nelarabine may be even more effective in newly diagnosed patients.
A Phase II trial was conducted by The Cancer and Leukemia Group (CALGB) and Southwestern Oncology Group (SWOG) on 40 patients ages 16 to 60 years with relapsed or refractory T-ALL (22 patients) and T-LBL (18 patients) (De Angelo et al 2002). All patients were refractory to at least one prior regimen or had relapsed prior to therapy with nelarabine. An alternate day schedule of single-agent nelarabine was implemented and 1.5 gm/m2 was administered on days 1, 3, and 5 of a 21-day cycle. The rationale for this schedule was two-fold. First, it was designed to reduce the neurotoxicity which was more pronounced in adult patients on the initial Phase I study (CitationKurtzberg et al 2005). Second, the pharmacologic rationale was based on the prolonged retention of ara-GTP in leukemia cells (CitationRodriguez et al 1997; CitationGandhi et al 2001). Of the 38 patients evaluable for response, 6 patients with T-ALL achieved a CR (29%) and 2 patients achieved a PR (9%). For those with T-LBL, 4 patients achieved a CR (24%). The overall response rate for all evaluable patients on this study was 32%. Although most reported toxicities were similar to the 5-day schedule in the initial pediatric phase I and II studies, neurotoxicity was negligible on this 3-day schedule.
The German Multicenter ALL study group (GMALL) reported favorable results in a Phase II study of 53 patients studied with relapsed/refractory T-ALL and T-LBL (CitationGeokbuget et al 2005). The median age of patients enrolled was 31 years. Thirty-six patients were in first relapse (68%), 7 were in second relapse (13%), 7 patients had relapsed after SCT (13%), and 3 patients were refractory to their initial induction regimen (6%). Similar to the CALGB study, nelarabine was administered on days 1, 3, and 5 at a dose of 1.5 g/m2. Overall, 25 patients achieved a CR (47%), and 7 patients achieved a PR (13%), for an overall response rate of 60%. Patients with T-ALL had the most favorable response with 76% achieving a CR. Importantly, 75% of patients achieving a CR went on to receive a stem cell transplant (SCT).
Investigators at MD Anderson Cancer Center completed a Phase II study which evaluated therapy in patients with non-Hodgkin’s lymphoma (CitationGoy et al 2003). Thirteen patients with peripheral T-cell lymphoma (PTCL) and 10 patients with low-grade B-cell lymphoma were eligible. The age range for patients on this trial was 33–81 years. All patients had failed 1–3 previous chemotherapy regimens. An alternating day schedule of nelarabine at 1.5 g/m2 was administered on days 1, 3, and 5. In this study, the course of therapy was repeated every 28 days, whereas the previous adult studies repeated every 21 days. Of the 17 evaluable patients, 2 patients achieved a CR (11%), and 6 achieved a PR (36%). Included in these responses were 4 patients with PTCL (2CR and 2PR for a response rate of 50%) and 4 patients with low-grade B-cell lymphoma (4PR for a response rate of 44%).
The first study combining nelarabine with another cytotoxic agent was performed by investigators at MD Anderson Cancer Center (CitationGandhi et al 2001). Thirteen patients were enrolled on the pilot protocol, most of whom had indolent leukemia, to receive a combination of fludarabine and nelarabine. Nelarabine, dosed at 1.5 g/m2 was administered on days 1, 3, and 5, in combination with 30 mg/m2 of fludarabine on days 3 and 5. Patient diagnoses included 9 with indolent leukemia, 2 had T-ALL, 1 CML, and 1 with mycosis fungoides. The fludarabine was administered 4 hours prior to nelarabine to enhance biochemical modulation. It was postulated that fludarabine, by inhibiting ribonucleotide reductase, would increase ara-GTP accumulation in leukemic cells. This hypothesis was supported by investigations reporting that higher intracellular concentrations of ara-GTP were achieved when human leukemia cells were incubated with both ara-G and fludarabine compared with ara-G alone (CitationRodriguez et al 1997). The overall response rate for patients entered in this trial was 46%, with 15% achieving a CR and 31% achieving a PR. Two patients with T-ALL and 1 patient with T-prolymphocytic leukemia (T-PLL) achieved a CR. Three patients with B-lineage chronic lymphocytic leukemia (B-CLL) achieved a PR. Of particular interest, 4 patients with either T-PLL or B-CLL were refractory to previous treatment with fludarabine (2 B-CLL and 1 T-PLL) or cladribine (1 T-PLL) alone. The authors suggest these responses are due to the superior pharmacokinetics of nelarabine and that these nucleoside analogs may not be cross-resistant.
To assess the feasibility and safety of adding nelarabine to an intensive Berlin-Frankfurt-Munster (BFM) regimen in children with newly diagnosed T-ALL, COG initiated a 2-stage pilot study (CitationReiter et al 1994; CitationDunsmore et al 2006). The end-point of this randomized pilot was toxicity. Eighty-seven evaluable patients were accrued. In stage I, only slow early responders, defined as ≥1000 peripheral blood blasts on day 8 of prednisone treatment or ≥1% minimal residual disease (MRD) at day 36 of induction therapy, were included. They were randomized either to receive (11 evaluable patients) or not to receive (16 evaluable patients) nelarabine 400 mg/m2/day for 5 days. No significant differences in toxicity between the two groups were noted. Stage II of the trial was limited to 61 evaluable patients with high risk T-ALL by National Cancer Institute (NCI) criteria. Patients were randomized to receive five courses of nelarabine at the Phase II MTD of 650 mg/m2/day (10 patients) or 400 mg/m2/day (51 patients) in combination with BFM chemotherapy. Toxicities were compared between the regimens with nelarabine (71 evaluable patients) and without nelarabine (16 evaluable patients). There were no differences in the incidence of peripheral neuropathy (5/71 with nelarabine vs 1/16 without nelarabine p = 1.0) or central neurotoxicity (2/71 with nelarabine vs 2/16 without nelarabine). The only difference in toxicities between regimens was a decrease in neutropenia and infection in the nelarabine arms (27/71 with nelarabine vs 13/16 without nelarabine p = 0.0021). There were no differences in toxicities between the two dose levels (650 mg/m2/day vs 400 mg/m2/day). Efficacy data from this study have not been published. The authors concluded that the addition of nelarabine to intensive chemotherapy for children with T-ALL was feasible with acceptable toxicity.
Pharmacology
The initial Phase I study of nelarabine published by Kurtz-berg et al included pharmacokinetic and pharmacodynamic analysis on 78 of the 93 patients enrolled on the trial (CitationGandhi et al 1998; CitationKisor et al 2000). When administered by IV infusion over 1 hour, the maximum plasma concentration (Cmax) is reached near the end of infusion and is directly proportional to the dose administered in the range of 5–75 mg/kg. Although there was wide patient variability, the volume of distribution and systemic clearance of nelarabine did not significantly differ between children and adults. Ninety-four percent of the administered dose of nelarabine is converted to ara-G in approximately 1 hour. The elimination half-life of nelarabine is less than 20 minutes and is similar in children and in adults. This short half-life is predominately explained by the mole to mole conversion of nelarabine to ara-G via adenosine deaminase (CitationKisor et al 2000).
After the rapid formation of ara-G from nelarabine, ara-G is then eliminated via phosphorylytic cleavage of the glycosidic bond by PNP to form guanine. Guanine is then deaminated to form xanthine, which is subsequently oxidized to uric acid. The elimination half life of ara-G is approximately 3 hours in adults and 2.1 hours in children. This difference in half-life can be attributed to a 30% higher clearance of ara-G in children compared with adults (CitationKisor et al 2000).
The intracellular pharmacokinetics of ara-GTP were investigated in patients enrolled in the initial Phase I clinical trial (CitationGandhi et al 1998). Although there was intrapatient variability, there was a dose dependent, linear increase in the accumulation of intracellular ara-GTP. Ara-GTP in malignant B and T lymphocytes is retained for a median duration of greater than 24 hours. In general, however, retention of ara-GTP was longer in T lymphoblastoid cells than in other leukemic blasts. Furthermore, malignant cells from patients who achieved a CR or PR had higher accumulation of ara-GTP than those who failed to respond (ara-GTP 150 μmol/L in responders and 44 μmol/L in non-responders).
The modulatory effect of fludarabine on intracellular ara-GTP concentration has also been evaluated (CitationGandhi et al 2001). Nelarabine (1.2 g/m2) was given on days 1, 3, and 5, and was preceded 4 hours earlier on days 3 and 5 by intravenous administration of 30 mg/m2 of fludarabine. Plasma pharmacokinetics revealed that fludarabine infusion on days 3 and 5 did not significantly effect the linear accumulation and elimination of nelarabine or ara-G. The elimination half-life of nelarabine in this combination trial did not differ significantly from that found in the single-agent Phase I trial. Although it was postulated that administration of fludarabine prior to nelarabine would increase the intracellular concentration of ara-GTP, intracellular pharmacokinetic evaluation revealed there was no difference in the overall AUC (0→∞) before and after fludarabine administration. The median peak intracellular ara-GTP concentrations were significantly different between the responders versus the non-responders (890 μmol/L vs 30 μmol/L). These data suggest that the accumulation of ara-GTP may not only predict the efficacy of nelarabine given alone, but also in combination with other chemotherapeutic agents.
Conclusion
The rates of response and overall survival of patients with T-ALL and T-LBL have improved with intensification of therapy and with our understanding of the molecular basis of the disease. In addition, advances in risk stratification have led to intensification of therapy for patients at higher risk of relapse. Despite these advances, the outcomes for patients who relapse is dismal, as salvage rates are modestly effective and remissions are not durable (CitationChessels 2003). Therefore, the development of new agents that have T-cell specificity is an important strategy in improving the survival of these patients. Nelarabine serves as an effective prodrug to generate ara-G in the plasma and intracellular GTP in leukemic blasts and is specifically toxic to T-lymphocytes and T-lymphoblasts. Further, accumulation of intracellular GTP correlates with response. (CitationGandhi et al 1998; CitationKisor et al 2000) Clinical and pharmacokinetic studies have established that nelarabine is active as a single agent in the treatment of T-cell malignancies (CitationBerg et al 2005). Based on the favorable pharmacokinetic profile and encouraging clinical data, nelarabine received accelerated approved for the treatment of relapsed or refractory T-ALL and T-LBL.
To convert to full approval, investigators need to demonstrate subsequent confirmation of clinical benefit. To this end, the COG plans to initiate a Phase III trial testing the efficacy of nelarabine 650 mg/m2/day in combination with augmented BFM chemotherapy in patients with intermediate risk T-cell ALL. This protocol is based on pilot data demonstrating that this combination is feasible with acceptable toxicity (CitationDunsmore et al 2006). To re-address concerns about neurotoxicity, there will be an initial safety phase of therapy open only to those at high risk for relapse (eg, M2 marrow and/or minimal residual disease >1% at end of induction). If the therapy is tolerated, all patients with intermediate and high risk for relapse will be included, thereby increasing the amount of patients that may benefit from this T-cell specific agent. As there is evidence that T-lymphoblasts are more sensitive to higher doses of methotrexate, a randomization between standard and high doses of methotrexate will be evaluated for low, intermediate, and high risk patients with T-ALL (William Carroll, pers comm).
To maximize its potential, the development of nelarabine should include rationally designed combinations based on its mechanism of action, selective cytotoxicity, and metabolic activation. Future trials may study an expanded role of nelarabine in stem cell transplant by evaluating it as a T-cell specific bone marrow purging agent (CitationGravatt et al 1993). Also, the dosing schedule differs for children and adults. Currently, pediatric patients receive 5 consecutive days of nelarabine while adults receive doses on days 1, 3, and 5. The alternate day dosing is based on the long retention time of ara-GTP in T-lymphoblasts and is supported by the decreased incidence of neurotoxicity in adult clinical trials (CitationGandhi et al 1998; CitationDeAngelo et al 2002). Future clinical studies in pediatric patients may choose to explore alternative doses and schedules of nelarabine administration.
References
- BashROCristWMShusterJJClinical features and outcome of T-cell acute lymphoblastic leukemia in childhood with respect to alterations at the TAL1 locus: a Pediatric Oncology Group studyBlood199381211078471769
- BergSLBlaneySMDevidasMPhase II study of nelarabine (compound 506U78) in children and young adults with refractory T-cell malignancies: a report from the Children’s Oncology GroupJ Clin Oncol20052333768215908649
- ChessellsJMVeysPKempskiHLong-term follow-up of relapsed childhood acute lymphoblastic leukaemiaBr J Haematol200312339640514616997
- CohenAGudasLJAmmannAJDeoxyguanosine triphos-phate as a possible toxic metabolite in the immunodeficiency associated with purine nucleoside phosphorylase deficiencyJ Clin Invest1978611405996138
- CohenALeeJWGelfandEWSelective toxicity of deoxyguanosine and arabinosyl guanine for T-leukemic cellsBlood19836166066600944
- CohenMHJohnsonJRMassieTApproval summary: nelarabine for the treatment of T-cell lymphoblastic leukemia/lymphomaClin Cancer Res20061253293517000665
- ConterVAricoMValsecchiMGLong-term results of the Italian Association of Pediatric Hematology and Oncology (AIEOP) acute lymphoblastic leukemia studies, 1982–1995Leukemia200014219620411187911
- CristWMShusterJJFallettaJClinical features and outcome in childhood T-cell leukemia-lymphoma according to stage of thymocyte differentiation: a Pediatric Oncology Group StudyBlood198872189173058229
- DeAngeloDJYuDDodgeRKA Phase II study of 2-amino-9β-D-arabinosyl-6-methoxy-9H-purine(506U78) in patients with relapse or refractory T-lineage acute lymphoblastic leukemias (ALL) or lymphoblastic lymphoma (abstract): CALGB Study 19801Blood2002100742
- DunsmoreKDevidasMBorowitzMJNelarabine can be safely incorporated into an intensive, multiagent chemotherapy regimen for the treatment of T-cell acute-lymphocytic leukemia (ALL) in children: A report of the Children’s Oncology Group (COG) AALL00P2 protocol for T-cell leukemiaBlood (ASH Annual Meeting Abstracts)20061081864
- FairbanksLDTaddeoADuleyJAMechanisms of deoxyguanosine lymphotoxicity. Human thymocytes, but not peripheral blood lymphocytes accumulate deoxy-GTP in conditions simulating purine nucleoside phosphorylase deficiencyJ Immunol1990144485912104895
- GandhiVMineishiSHuangPCytotoxicity, metabolism, and mechanisms of action of 2′, 2′-difluorodeoxyguanosine in Chinese hamster ovary cellsCancer Res1995551517247533664
- GandhiVPlunkettWRodriquezCOCompound GW506U78 in refractory hematologic malignancies: relationship between cellular pharmacokinetics and clinical responseJ Clin Oncol1998163607159817282
- GandhiVPlunkettWWellerSEvaluation of the combination of nelarabine and fludarabine in leukemias: clinical response, pharmacokinetics, and pharmacodynamics in leukemia cellsJ Clin Oncol20011921425211304766
- GarandRVannierJPBeneMCComparison of outcome, clinical, laboratory, and immunological features in 164 children and adults with T-ALL. The Groupe d’Etude Immunologique des LeucemiesLeukemia19904739442232884
- GaynonPSTriggMEHeeremaNAChildren’s Cancer Group trials in childhood acute lymphoblastic leukemia: 1983–1995Leukemia20001422233311187913
- GiblettERAmmannAJWaraDWNucleoside-phosphorylase deficiency in a child with severely defective T-cell immunity and normal B-cell immunityLancet197511010348676
- GoekbugetNArnoldRAttaJCompound GW506U78 has high single-drug activity and good feasibility in heavily preatreated relapsed T-lymphoblastic leukemia (T-ALL) and T-lymphoblastic lymphoma (T-LBL) and offers the option for cure with stem cell transplantation (SCT) [abstract]Blood2005106S1 Abstract 150
- GoyABleyerAHagemeisterFPhase II study of compound GW506U78 (araG) for patients with indolent B-cell or peripheral T-cell lymphoma previously treated with chemotherapyPresented at 45th Annual Meeting; American Society of Hematology2003
- GravattLCChaffeeSHebertMEEfficacy and toxicity of 9-beta-D-arabinofuranosylguanine (araG) as an agent to purge malignant T cells from murine bone marrow: application to an in vivo T-leukemia modelLeukemia19937126178350627
- KisorDFPlunkettWKurtzbergJPharmacokinetics of nelarabine and 9-beta-D-arabinofuranosyl guanine in pediatric and adult patients during a phase I study of nelarabine for the treatment of refractory hematologic malignanciesJ Clin Oncol200018995100310694549
- KurtzbergJErnstTJKeatingMJPhase I study of 506U78 administered on a consecutive 5-day schedule in children and adults with refractory hematologic malignanciesJ Clin Oncol200523339640315908652
- LambeCUAverettDRPaffMT2-Amino-6-methoxy-purine arabinoside: an agent for T-cell malignanciesCancer Res199555335267614470
- MitchellBSMejiasEDaddonaPEPurinogenic immunodeficiency diseases: selective toxicity of deoxyribonucleosides for T-cellsProc Natl Acad Sci USA19787550114311004
- MomparlerRLFisherGAMammalian deoxynucleoside kinase. I. Deoxycytidine kinase: purification, properties, and kinetic studies with cytosine arabinosideJ Biol Chem196824342983045684726
- OsborneWRScottCRThe metabolism of deoxyguanosine and guanosine in human B and T-lymphoblasts. A role for deoxyguanosine kinase activity in the selective T-cell defect associated with purine nucleoside phosphorylase deficiencyBiochem J198321471186312962
- PrusKLAverettDRZimmermanTPTransport and metabolism of 9-beta-D-arabinofuranosylguanine in a human T-lymphoblastoid cell line: nitrobenzylthioinosine-sensitive and -insensitive influxCancer Res1990501817212306735
- PuiCHEvansWEAcute lymphoblastic leukemiaN Engl J Med1998339605159718381
- PuiCHRellingMVEvansWERole of pharmacogenomics and pharmacodynamics in the treatment of acute lymphoblastic leukaemiaBest Pract Res Clin Haematol2002157415612617874
- PuiCHChengCLeungWExtended follow-up of long-term survivors of childhood acute lymphoblastic leukemiaN Engl J Med2003349640912917300
- PuiCHRellingMVDowningJRAcute lymphoblastic leukemiaN Engl J Med200435015354815071128
- ReiterASchrappeMLudwigWDChemotherapy in 998 unselected childhood acute lymphoblastic leukemia patients. Results and conclusions of the multicenter trial ALL-BFM 86Blood1994843122337949185
- RodriquezCOLeghaJKEsteyEPharmacological and biochemical strategies to increase the accumulation of arabinofuranosyl-guanine triphosphate in primary human leukemia cellsClin Cancer Res199732107139815603
- RodriguezCOGandhiVArabinosylguanine-induced apoptosis of T-lymphoblastic cells: incorporation into DNA is a necessary stepCancer Res19995949374310519407
- RodriquezCOMitchellBSAyresMArabinosylguanine is phosphorylated by both cytoplasmic deoxycytidine kinase and mitochondrial deoxyguanosine kinaseCancer Res2002623100512036920
- RodriquezCOStellrechtCMGandhiVMechanisms for T-cell selective cytotoxicity of arabinosylguanineBlood20031021842812750168
- SchorinMABlattnerSGelberRDTreatment of childhood acute lymphoblastic leukemia: results of Dana-Farber Cancer Institute/Children’s Hospital Acute Lymphoblastic Leukemia Consortium Protocol 85-01J Clin Oncol19941274078151317
- SmithMArthurDCamittaBUniform approach to risk classification and treatment assignment for children with acute lymphoblastic leukemiaJ Clin Oncol19961418248558195
- UckunFMSenselMGSunLBiology and treatment of childhood T-lineage acute lymphoblastic leukemiaBlood199891735469446631
- VidarssonBAbonourRWilliamsECFludarabine and cytarabine as a sequential infusion regimen for treatment of adults with recurrent, refractory, or poor prognosis acute leukemiaLeuk Lymphoma2001413213111378544