Abstract
Chronic periaortitis includes a variety of conditions that have similar clinical and histopathological findings, and thus probably represents different manifestations of the same disease: idiopathic retroperitoneal fibrosis, perianeurysmal retroperitoneal fibrosis, and inflammatory abdominal aortic aneurysms. We describe the clinical and imaging characteristics of the nonaneurysmal form of chronic periaortitis, recognized as isolated periaortitis, in an adult male patient presented with low back pain.
Case report
A 53-year-old hypertensive man presented with low back pain of eight months duration. The pain was of moderate intensity, unaffected by motion, and not relieved by bed-rest. He had no fever, but noted 4 kg weight loss during the preceding months. Laboratory examination revealed normocytic anemia, elevated erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) of 86 mg/Dl (normal < 5 mg/Dl). Renal function, liver, and bone profile were within normal limits. Additional investigations, including ANA, ANCA, and serological testing for syphilis were negative. Chest and lumbar spine radiographs were normal. A computerized tomography (CT) scan of the lumbar spine was undertaken to exclude any inflammatory process such as discitis or osteomyelitis. This showed retroperitoneal soft tissue thickening. Thus, CT angiography (CTA) of the aorta was performed and showed diffuse atheromatous changes in the thoracic and abdominal aorta including ulcerated plaques and an extensive aortic thickening confined to the entire abdominal aorta without any abnormal dilatation. In addition, there was a retroperitoneal concentric periaortic soft tissue mass (rind of periaortic tissue) causing luminal narrowing of the abdominal aorta and significant ostial stenosis of the celiac trunk, superior mesenteric artery (SMA), and both renal arteries (). The left renal vein was also involved and the left kidney showed a hypodense cortical area at the lower pole consistent with renal infarct. There was no ureteric obstruction or hydronephrosis. This presentation was consistent with the diagnosis of isolated periaortitis confined to abdominal aorta. He was treated with prednisone 60 mg/day, resulting in gradual improvement of signs and symptoms over several weeks. Metothrexate was added to help steroid weaning. Repeated CT scans showed progressive resolution of the periaortic rind with no evidence of abdominal aorta aneurysm.
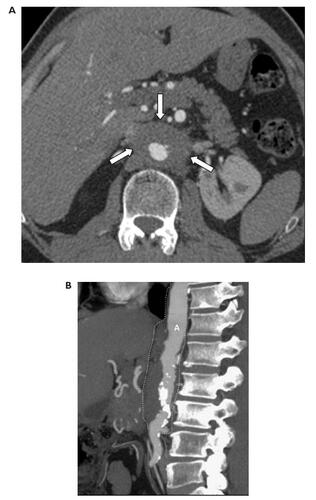
Figure 1 CT angiography of the aorta performed with 64-row MDCT. (A) Axial image at the level of the renal arteries showing narrowing of the aortic lumen, aortic wall thickening and periaortic rind (arrows). (B) Multiplanar reformat image showing periaortic thickening confined to the abdominal aorta (A) (dashed line). The thoracic aorta is spared. Numerous calcified plaques are seen mainly in the infrarenal segment of the abdominal aorta.
Discussion
Chronic periaortitis is a rare disease, occurs usually in middle-aged adult men. It includes a variety of conditions that have similar clinical and histopathological findings, and thus probably represents different manifestations of the same disease: idiopathic retroperitoneal fibrosis, perianeurysmal retroperitoneal fibrosis, and inflammatory abdominal aortic aneurysms (CitationParums 1990; CitationVaglio et al 2003; CitationMitnick et al 2004). The three entities are characterized by advanced atherosclerosis of the abdominal aorta, adventitial and periadventitial inflammation, medial thinning, and chronic retroperitoneal inflammatory process associated with a varying degree of fibrotic reaction surrounding the abdominal aorta (CitationParums 1990). Periaortitis may be the expression of a local immune response to antigens such as oxidized-low density lipoproteins and ceroid in the atherosclerotic plaques of the abdominal aorta (CitationVaglio and Buzio 2005a; CitationVaglio et al 2006). However, because most patients with periaortitis also suffer from constitutional symptoms and show elevated acute-phase reactant levels, positive autoantibodies and, in some cases, autoimmune diseases affecting other organs, periaortitis may also be considered a manifestation of a systemic autoimmune disease such as ankylosing spondylitis, rheumatoid arthritis and systemic lupus erythematosus (CitationBlockmans 2000; CitationMonev 2002; CitationCarels et al 2005). In the absence of any systemic autoimmune disease and the negative ANA, ANCA, and serological testing for syphilis, the pathogenesis of the disease in our case may be the result of a local reaction to advanced atherosclerosis. Biopsy is necessary to exclude other disease such as malignancy or infections. In our patient, biopsy was not performed because of the periaortic location of the mass.
Isolated periaortitis typified by the present case represents the nonaneurysmal form of chronic periaortitis. CitationMitnick et al (2004) reported four patients with isolated periaortitis who did not develop an aortic aneurysm or retroperitoneal fibrosis during the follow-up period. In this form of chronic periaortitis, the abdominal aorta (particularly the infra-renal portion) has normal or decreased diameter and is surrounded by a mantle of soft-tissue density (). Furthermore, the disease tends primarily to involve the vascular structures causing stenosis of the major branches of the abdominal aorta (eg, celiac trunk, SMA, renal arteries) as reported in the present case, rather than entrapment of the ureters, and consequently obstructive hydro-uretronephrosis as in the idiopathic retroperitoneal fibrosis manifestation.
The classical presentation of isolated periaortitis is with pain, fever, fatigue, weight loss, and anemia. Abdominal pain, diarrhea, and gastrointestinal hemorrhage may result from mesenteric artery ischemia, but this is uncommon. Renovascular hypertension may result from renal artery stenosis. Depending on what other vessels are involved, claudication, and other manifestations of vascular impairment may accompany this disorder.
Contrast-enhanced CT, magnetic resonance imaging (MRI), and positron emission tomography (PET) scan are the noninvasive diagnostic modalities of choice for isolated periaortitis. PET scan with 18F-fluorodeoxyglucose is a reliable tool in assessing the metabolic activity of the mass, detecting other sites of inflammation and disclosing infectious or neoplastic lesions to which periaortitis can be secondary or with which it can be associated (CitationSalvarani et al 2005; CitationVaglio et al 2005b). Furthermore, this technique is valuable for patients follow-up since abnormal fluorodeoxyglucose uptake can also be seen at disease relapse.
Nonenhanced CT scan reveals a low density soft tissue mass surrounding the abdominal aorta. The periaortic mass usually shows varying degree of enhancement after administration of contrast agent. In addition, the abdominal aorta and its major branches appear to be narrowed. At MR imaging, periaortitis is hypointense on T1-weighted images and usually hyperintense on T2-weighted images. The periaortic soft tissue mass typically shows intense enhancement after administration of gadolinium (CitationVaglio et al 2003; CitationMitnick et al 2004). While CT and MR images are quite similar, advantages of MRI include repeat studies without radiation exposure and contrast administration with reduced risk of nephrotoxicity. Nephrogenic systemic fibrosis or nephrogenic fibrosing dermopathy has been reported as a rare complication after administration of gadolinium based contrast agent in patients with kidney disease, particularly in the presence of a proinflammatory process such as major surgery, infection, or a vascular thromboembolic event (CitationSadowski et al 2007).
Regarding management, steroids are usually effective and induce remission of the clinical symptoms, normalization of the acute-phase reaction, reduction in size of the retroperitoneal mass and also resolution of the obstructive complications (CitationDemko et al 1997; CitationKardar et al 2002; CitationJois et al 2004). Nevertheless, the duration of treatment, the effectiveness and the persistence of the results are still uncertain because few cases have been reported in the literature. A number of immunosuppressive drugs, such as azathioprine, cyclophosphamide, and methotrexate, have been used as steroid-sparing agents or in patients not responding to steroids alone or when steroids cannot be tapered (CitationHarreby et al 1994; CitationScavalli et al 1995; CitationGrotz et al 1998; CitationMarcolongo et al 2004). Recently, based on its utility in drug-eluting stents to prevent restenosis, rapamycin (sirolimus) has been suggested as treatment to prevent connective tissue proliferation about the injured aorta (CitationKanko et al 2006). In our case the patient responded to therapy with steroids without developing retroperitoneal fibrosis and abdominal aorta aneurysm during the follow-up period of 24 months.
Isolated periaortitis corresponds to the nonaneurysmal form of chronic periaortitis. Treatment of periaortitis with steroids and immunosuppressants leads to resolution of clinical symptoms and periaortic soft tissue mass. Awareness and recognition of imaging findings associated with isolated periaortitis are crucial for early diagnosis and institution of adequate therapy in order to avoid further complications such as luminal narrowing of the aorta and its major branches.
Disclosures
All authors state that no financial relationship to disclose. All the authors state that there is no conflict of interest regarding this work.
References
- BlockmansDBaeyensHVan LoonRPeriaortitis and aortic dissection due to Wegener’s granulomatosisClin Rheumatol200019161410791632
- CarelsTVerbekenEBlockmansDP-ANCA-associated periaortitis with histological proof of Wegener’s granulomatosisClin Rheumatol20052483615565392
- DemkoTMDiamondJRGroffJObstructive nephropathy as a result of retroperitoneal fibrosis: a review of its pathogenesis and associationsJ Am Soc Nephrol19978684810495799
- GrotzWvon ZedtwitzIAndreMTreatment of retroperitoneal fibrosis by mycophenolate mofetil and corticosteroidsLancet199835211959777843
- HarrebyMBildeTHelinPRetroperitoneal fibrosis treated with methylprednisolone pulse and disease-modifying antirheumatic drugsScand J Urol Nephrol199428237427817165
- JoisRNGaffneyKMarshallTChronic periaortitisRheumatology2004431441615266064
- KankoMOzbudakEOzerdemAEffect of sirolimus in the prevention of adhesions around intraabdominal prosthetic graftWorld J Surg20063016485216847710
- KardarAHKattanSLindstedtESteroid therapy for idiopathic retroperitoneal fibrosis: dose and durationJ Urol2002168550512131307
- MarcolongoRTavoliniIMLavederFImmunosuppressive therapy for idiopathic retroperitoneal fibrosis: a retrospective analysis of 26 casesAm J Med2004116194714749165
- MitnickHJacobowitzGKrinskyGPeriaortitis: Gadolinium-enhanced Magnetic Resonance Imaging and Response to Therapy in Four PatientsAnn Vasc Surg200418100714712373
- MonevSIdiopathic retroperitoneal fibrosis: prompt diagnosis preserves organ functionCleveland Clin J Med2002691606
- ParumsDVThe spectrum of chronic periaortitisHistopathology199016423312193863
- SadowskiEABennettLKChanMRNephrogenic systemic fibrosis: risk factors and incidence estimationRadiology20072431485717267695
- SalvaraniCPipitoneNVersariAPositron emission tomography (PET): evaluation of chronic periaortitisArthritis Rheum20055329830315818649
- ScavalliASSpadaroAARiccieriVLong-term follow-up of low-dose methotrexate therapy in one case of idiopathic retroperitoneal fibrosisClin Rheumatol1995448147586991
- VaglioACorradiDManentiLEvidence of autoimmunity in chronic periaortitis: a prospective studyAm J Med20031144546212727578
- VaglioABuzioCChronic periaortitis: a spectrum of diseaseCurr Opin Rheumatol2005a17344015604902
- VaglioAGrecoPVersariAPost-treatment residual tissue in idiopathic retroperitoneal fibrosis: active residual disease or silent scar? A study using 18F-fluorodeoxyglucose positron emission tomographyClin Exp Rheumatol2005b23231415895895
- VaglioAGrecoPCorradiDAutoimmune aspects of chronic periaortitisAutoimmun Rev200654586416920572