Abstract
The renin angiotensin aldosterone system (RAAS) plays an important role in the pathophysiology of cardiovascular disease. Angiotensin converting enzyme inhibitors (ACEi) have proven benefit in reducing cardiovascular events in patients at high risk. Angiotensin receptor blockers (ARB) have been demonstrated to have benefit in the management of heart failure and to be non-inferior to ACEi in patients with left ventricular dysfunction after a myocardial infarction (MI). Yet until now, there has been no trial to support the use of the ARB for vascular protection. The ONTARGET study showed that the ARB telmisartan conserved 95% of the vascular protective properties of the ACEi ramipril, given at similar doses to a similar patient group as had been previously shownin the HOPE study to benefit from ACE inhibition with ramipril. The TRANSCEND study in a similar population of patients who were intolerant of ACEi despite the primary endpoint being neutral, showed a trend to a benefit for the combined secondary endpoint of cardiovascular death, MI and stroke, with excellent tolerance of the ARB. The reasons for neutral result of the TRANSCEND study result include an underpowered study, and pre-treatment with a RAAS inhibitor in a high proportion of patients. These studies indicate that an ARB can be used for vascular protection in high risk individuals in the place of an ACEi. However ACEi will probably remain the first choice due to the greater body of supportive evidence.
Introduction
Modulation of the renin angiotensin aldosterone system (RAAS) with angiotensin converting enzyme inhibitors (ACEi) reduces cardiovascular events in individuals at high risk.Citation1 Clinical trials in hypertension and heart failure suggested the angiotensin receptor blockers (ARB) might have the vascular protective benefits of the ACEi with less adverse effects. However approximately 20% of patients, especially women and Asians, are unable to take an ACEi due to adverse effects such as cough, hypotensive symptoms, and angioneurotic edema. Consequently, an angiotensin receptor blocking agent (ARB) could be an alternative treatment to ACEi for vascular protection, with better patient tolerability.
The results of the ONTARGETCitation2 and TRANSCENDCitation3 studies, the largest clinical trial program ever conducted with an angiotensin receptor blocker, were recently reported. These trials examined strategies for cardiovascular risk reduction in high risk patients aged >55 years old, with coronary, cerebrovascular disease, peripheral vascular disease or diabetes with target organ damage. ONTARGET compared the ARB telmisartan alone, or in combination with the ACEi ramipril, with ramipril treatment, for the protection against major cardiovascular events such as cardiovascular death, myocardial infarction (MI), stroke, or hospitalization for heart failure. TRANSCEND compared telmisartan to placebo in patients who were intolerant of ACEi. The aims of the ONTARGET/TRANSCEND program were to learn whether adding the ARB telmisartan to proven therapy with an ACEi would further improve cardiovascular outcomes, and to establish the benefits of the ARB in this high risk population.
Vascular protection and RAAS modulation
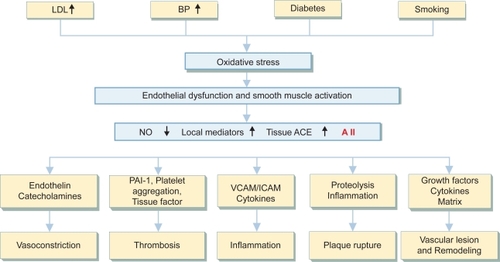
Activation of the RAAS system is implicated in a range of cardiovascular and renal pathophysiology:Citation4 the development of atherosclerosis, the complications of atherosclerosis such as acute MI, adverse myocardial remodeling and the development of heart failure, the development of systemic hypertension, and the development of progressive renal dysfunction. Angiotensin II mediated stimulation of the AT1 receptor increases arterial pressure, promotes oxidative stress, stimulates an inflammatory response, and adversely alters the balance between the thrombotic and fibrinolytic state (). Experimental evidence supports the hypothesis that both ACEi and the ARB classes of RAAS modulators have properties that may reduce the development of atherosclerosis and its complications. However differences between ACEi and ARB responses are observed, such that the ARBs might be pro-thrombotic by stimulating PAI-1 synthesisCitation5 and and encourage plaque rupture by enhancing MMP-1 activity.Citation6
Figure 1 The role of the renin angiotensin aldosterone system in vascular disease. Angiotensin II (AII) is an important mediator of vascular damage that promotes the development of atherothrombosis and the complications of atherosclerosis.
Angiotensin converting enzyme inhibition and vascular protection
The SOLVDCitation7 and SAVECitation8,Citation9 studies were designed to test the hypothesis that RAAS modulation with an ACEi would slow the progression and development of heart failure. A surprising finding of both studies was a 20% reduction of the incidence of MI. These observations lead to the HOPE study,Citation10 in which high dose ACEi with ramipril 10 mg daily reduced the risk of MI by 20%, stroke by 32%, and cardiovascular mortality by 26% in patients at high risk for cardiovascular events but without heart failure or a low left ventricular ejection fraction. The EUROPA studyCitation11 supported the observations of the HOPE study. Perindopril 8 mg daily in patients with coronary artery disease, reduced the endpoint of cardiovascular mortality, non-fatal MI, and cardiac arrest by 20%. The PEACE studyCitation12 failed to show a benefit from treatment with trandolapril 4 mg daily in patients with coronary artery disease. The study population was at low risk of cardiovascular events and the trial underpowered to show a benefit from the ACEi treatment. Coronary revascularization was the major contributor to the combined endpoint and occurred at similar rates in both treatment arms. In contemporary North American practice, aggressive coronary revascularization is probably a non-modifiable endpoint, as it is widely used independent of ischemia driven indications.
A combined analysisCitation13 of the HOPE, EUROPA and PEACE studies showed that ACEi significantly reduced all-cause mortality (7.8 vs 8.9% p = 0.0004), cardiovascular mortality (4.3 vs 5.2% p = 0.0002), non-fatal MI (5.3 vs 6.4% p = 0.0001), stroke (2.2 vs 2.8% p = 0.0004), coronary artery bypass surgery (6.0 vs 6.9%), but not percutaneous coronary intervention (7.4 vs 7.6% p = 0.48). Similar reductions of cardiovascular mortality and MI are observed in the five trials in patients with heart failure or left ventricular systolic dysfunction.Citation14
ARBs and vascular protection: pre-ONTARGET/TRANSCEND
Unlike the ACEi studies, most of which compared the ACEi with placebo, the ARBs have been compared with an active comparator. In heart failure trials, the comparator was usually an ACEi, whereas in hypertension trials the ARB was compared with other medication strategies. Placebo-controlled clinical trials with evaluation of clinical outcomes are either in ACEi-intolerant patients (CHARM alternativeCitation15,Citation16) or in patients with diabetic nephropathy (RENAALCitation17 and IDNTCitation18).
The CHARM studyCitation19 showed that the addition of the ARB candesartan to standard treatment, that included an ACEi reduced cardiovascular deaths and hospital admissions for heart failure. The combination of candesartan with an ACEiCitation20 was associated with a 17% reduction of both cardiovascular mortality and admission to hospital for heart failure compared to those receiving only an ACEi. Patients receiving candesartan and an ACEi had a 23% (95% CI 2%–40%) reduction of non-fatal MICitation21 and a 12% (95% CI 13%–21%) reduction of cardiovascular death. Yet in the CHARM Alternative trial,Citation15,Citation16 where candesartan was compared to placebo in patients intolerant of ACEi, the incidence of MI increased by 52%, but cardiovascular death was 20% less (p = 0.02 after covariate adjustment).
ARBs are effective and well tolerated antihypertensive agents. The LIFE studyCitation22 in older patients with moderately severe hypertension and left ventricular hypertrophy, showed the ARB losartan when compared to atenolol, resulted in a greater reduction of the combined end-point of cardiovascular death, MI or stroke after equal blood pressure control. In patients with diabetes, losartan reduced cardiovascular and total mortality, but not MI. In the VALUE study,Citation23 valsartan was not as effective an antihypertensive agent as amlodipine, yet there was no difference in the primary combined endpoint of cardiovascular mortality and morbidity. Yet, the valsartan-treated patients had a 19% relative increase in MI (p = 0.02) and a 15% (p = 0.08) increase in stroke compared to individuals receiving amlodipine.
ACEi in patients following MI reduce the risk of death by 26%, heart failure admissions by 27%, and recurrent MI by 20%.Citation24 The ARB valsartan in the VALIANT studyCitation25 was shown to be non-inferior to captopril for the reduction of all-cause mortality in patients with heart failure or left ventricular ejection fraction <40%. In this study MI occurred as frequently in valsartan as in captopril treated patients. Yet a discussion paperCitation26 based on a meta-analysis of over 50, 000 patients, suggested that ARBs might increase the incidence of MI. An alternative explanation to this hypothesis is that the comparators in these trials (including ACEi and beta-adrenergic blockers) were more effective than an ARB for the reduction of coronary events.
The nephropathy studies RENAALCitation17 and IDNTCitation18 showed that ARBs compared to placebo successfully slowed the progression of renal disease. Yet in these high risk patients, it is surprising that ARBs did not reduce vascular endpoints. It is likely these trials, primarily designed to examine renal endpoints, were underpowered to answer questions about cardiovascular events.
ONTARGET/TRANSCEND study designCitation27
The Ongoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial (ONTARGET)Citation2 and Telmisartan Randomized Assessment Study in ACE Intolerant Subjects with Cardiovascular Disease (TRANSCEND)Citation3 studies examined the role of ARBs when used alone or in combination with an ACEi in high risk individuals with controlled hypertension (). The design of the ONTARGET/TRANSCEND studies closely resembled that of the HOPE study, knowing that ramipril in this population was beneficial and to allow comparisons of the outcomes of the two trials. The primary objective of ONTARGET was to determine whether the combination of telmisartan and ramipril was more effective than ramipril alone and to assess whether telmisartan alone was at least as effective as ramipril. TRANSCEND was a placebo-controlled study to determine whether telmisartan reduces vascular endpoints compared to placebo in patients intolerant of ACEi.
Figure 2 Study design and outcomes of ONTARGET and TRANSCEND studies.
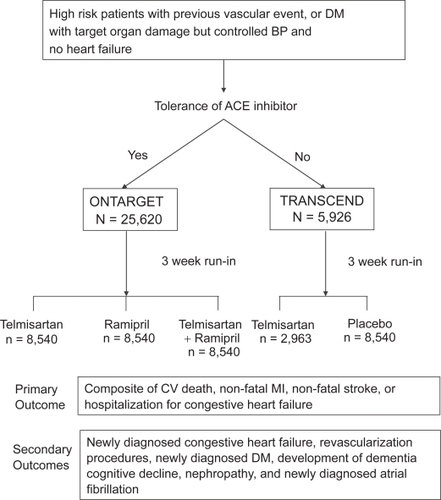
The primary endpoint for both ONTARGET and TRANSCEND was the combination of cardiovascular death, non-fatal MI, stroke, or hospitalization for heart failure. Both studies included patients at high risk of coronary, peripheral or cerebrovascular events. Recruitment from 730 centers in 40 countries for ONTARGET (n = 25,620) was completed in July 2003, and TRANSCEND (n = 6000) in May 2004. The planned follow-up period was 3.5 to 5.5 years. The study was designed to have a 93% power of showing a 13% superiority of telmisartan plus ramipril vs ramipril alone. In addition the study had an 89% power of showing the non inferiority of telmisartan compared to captopril whilst ensuring telmisartan has at least 50% of the ramipril effect at the upper 95th% confidence limit. In TRANSCEND with 3000 patients in each group, the study had a 94% power to show a 19% superiority of telmisartan over placebo, assuming an event rate of 5.1%/year, a recruitment period of 2 years and a maximum follow-up of 5.5 years.
Baseline characteristics in ONTARGET and TRANSCEND
The age of the patients in ONTARGET (66.4 years) and TRANSCEND (66.9 years) was slightly greater than in HOPE (65.9 years). Diabetes was present with a similar prevalence in ONTARGET (37.3%) and TRANSCEND (35.4%) as in HOPE (38.3%). ACEi (57.5%) and statin (61%) usage prior to enrollment was considerably greater than reported in HOPE (ACEi 11.6%, statins 28.9%). It is notable that there was a baseline 56% ACEi usage in TRANSCEND, in patients supposedly intolerant to ACEi. The TRANSCEND population had several baseline differences from both ONTARGET and HOPE. In TRANSCEND there were a higher proportion of female patients (42.9%) than in ONTARGET (26.7%) or HOPE (26.7%).
Results of ONTARGET
Differences in blood pressure between the treatment groups during the trial were modest. The average difference of blood pressure for the telmisartan-treated groups (compared to ramipril) was 0.9/0.6 mmHg, and for telmisartan + ramipril 2.4/1.4 mmHg.
After a median follow-up of 56 months the incidence of the primary outcome of cardiovascular death, non-fatal MI, stroke, or the development of heart failure did not differ significantly between either the telmisartan + ramipril or the telmisartan groups compared to the ramipril group. The confidence intervals of the relative risk of the telmisartan vs ramipril comparison were within the pre-specified boundaries to show that telmisartan was not inferior to ramipril, and had conserved 95% of the efficacy of ramipril (). Consequently ONTARGET shows that telmisartan was as effective as ramipril, and well tolerated.
Figure 3 Relative risk for primary outcome (cardiovascular death, MI, stroke and hospitalization for heart failure) and secondary HOPE study outcome (cardiovascular death, MI or stroke). The confidence interval is well within the predefined boundary for non-inferiority of telmisartan compared with ramipril.
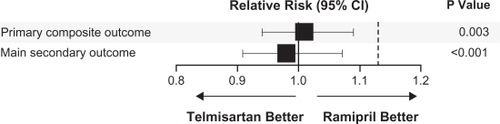
Figure 4 TRANSCEND study comparing telmisartan 80 mg daily with placebo in high risk patients. Kaplan-Meier Curves for the secondary outcome of cardiovascular death, MI or stroke (HOPE study outcome). After statistical correction for multiple comparisons and overlap with the primary endpoint, the difference was not statistically significant (p = 0.68).
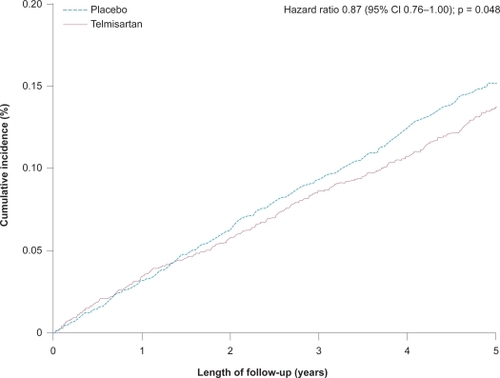
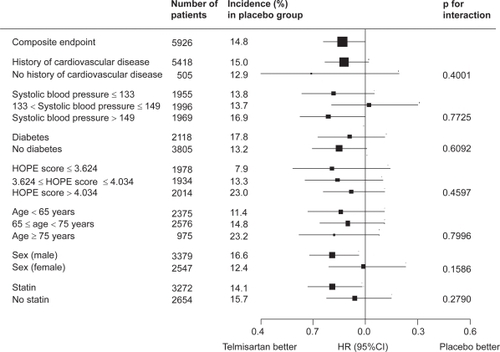
Figure 5 Relative risks for secondary HOPE study endpoint of cardiovascular death, MI and stroke in the TRANSCEND study.
The combination of telmisartan and ramipril did not result in any improved outcome beyond that achieved by ramipril alone. Yet the combined treatment resulted in more hypotension, syncope, renal dysfunction, hyperkalemia, and a trend towards a greater risk of renal dysfunction requiring dialysis. A subsequent analysisCitation28 of the renal outcomes of ONTARGET showed that the combination of telmisartan and ramipril increased the renal endpoints of dialysis and doubling of creatinine and death compared to treatment with the individual agents: ramipril 13.4%, telmisartan 13.5%, ramipril + telmisartan 14.5% RR 1.09 (p = 0.037) and dialysis and doubling of creatinine ramipril 2.03%, telmisartan 2.21%, ramipril + telmisartan 2.49% RR 1.24, (p = 0.038). Many of the dialysis events were for acute dialysis, probably resulting from acute renal failure due to excessive blood pressure reduction in patients with atherosclerotic renal artery disease. For the 700 patients with diabetic nephropathy, the combined telmisartan + ramipril treatment resulted in a non-significant 8% reduction of the combined endpoint of death, doubling of creatinine, or need for dialysis. Consequently, there is no benefit of ACEi + ARB combination therapy in any group of patients included in the ONTARGET study, beyond a reduction of albuminuria.
TRANSCEND
The TRANSCEND studyCitation3 comparing telmisartan and placebo in high risk patients intolerant of ACEi failed to show a clear benefit of ARB therapy. Blood pressure was reduced 4/2 mmHg by telmisartan. The primary end-point of death, MI, stroke or admission to hospital with heart failure occurred in 15.7% of patients receiving telmisartan and 17.0% receiving placebo (HR 0.92, p = 0.216). The secondary HOPE endpoint of death, MI, stroke () appeared to be reduced (13% vs 14.8%, HR 0.87, p = 0.048). However after adjustment for multiple comparisons, the difference was non-significant (p = 0.068). Telmisartan was well tolerated in patients reported to be previously intolerant of ACEi, and fewer patients discontinued telmisartan than discontinued placebo treatment. Hypotensive symptoms were the commonest, yet very infrequent adverse event (telmisartan 0.98% vs placebo 0.54%) resulting in permanent discontinuation of treatment. In addition the safety of telmisartan was good in the 377 patients who had previously had severe reactions to an ACEi.
The Prevention Regimen for Effectively Avoiding Second Strokes (PRoFESS) StudyCitation29 of more than 20, 000 patients, compared the effect of telmisartan 80 mg daily with placebo in the secondary prevention of cardiovascular events including a further stroke. Despite a blood pressure reduction of 3.8/2.0 mmHg there was no reduction of the incidence of subsequent stroke or major cardiovascular events. Outcomes appeared to be improved for events that occurred after 6 months of treatment. In a pre-specified combined analysis of TRANSCEND and PRoFESS with more than 26,000 patients, benefit from telmisartan was seen after 6 months treatment (cardiovascular death, MI, stroke, hospitalization for heart failure OR 0.86 (95% CI 0.80–0.94). However there was little or no benefit in the first 6 months after randomization (OR 1.12 95% CI 0.99–1.27). It is therefore possible that more prolonged treatment with telmisartan could have resulted in a greater benefit. In TRANSCEND, the mean duration of treatment to the occurrence of a vascular event is only 2 ½ years: a short time frame by comparison of the time taken for blood pressure lowering or lipid-lowering agents to show significant benefit.
Discussion
ARB = ACEi?
The vascular protective property of ACEi has been shown in clinical trials and subsequent meta-analyses. Studies with ARBs in patients with hypertension, heart failure and renal disease have yielded conflicting results. The ONTARGET study in patients at high risk of cardiovascular events showed that telmisartan was non-inferior, as defined by pre-specified boundaries, to the ACEi ramipril given at the same dose as had been proven to be beneficial in the HOPE study. The study showed that telmisartan conserved 95% (95% CI 83.2–106.3) of the benefits of ramipril assessed by the primary composite outcome and 105% (95% CI 91.6–119.0) of the benefits assessed by the secondary outcome of cardiovascular death, MI and stroke. These benefits were observed in a high risk population with Death/MI/Stroke event rates similar to those observed in the index HOPE study (cardiovascular/year rates: ONTARGET 3.0%/year, HOPE 2.8%/year). Consequently the equivalence of telmisartan to the ACEi ramipril for clinical application has been conclusively demonstrated. The ONTARGET study has raised several questions about the generalizabilty of the findings. Can we assume that all ARBs can be used to replace an ACEi? Does telmisartan have any special properties? Telmisartan has a long biological half-life, and has PPAR agonist properties in addition to those of an AT1 receptor blocker. Whether PPAR agonist activity is beneficial or harmful in this situation is unknown. Other ARBs in heart failure trials have shown equal vascular protection when added to treatment that included an ACEi (CHARM overall,Citation20 or compared to an ACEi (VALIANTCitation25). Yet the same ARBs in other situations when compared to placebo have been associated with an increased risk for MI (CHARM alternativeCitation15,Citation16 in ACE intolerant patients and VALUECitation23 in high vascular risk patients with hypertension. So there is some uncertainty whether other ARBs would have been non-inferior to ramipril if they had been tested in an ONTARGET-like trial. Furthermore we do not know the optimal dose of other agents. However, the dose of telmisartan for ONTARGET was chosen as that known to have an effective antihypertensive action: the same reasoning could be applied to select the dose of other ARBs for vascular protection.
Why no additional benefit from ACEi + ARB?
The combination of ramipril and telmisartan resulted in no additional benefit beyond that achieved with either drug alone. Furthermore the combination therapy was associated with an increased incidence of adverse effects including those related to symptomatic hypotension, a deterioration of renal function, and hyperkalemia. The ACEi/ARB combination did reduce blood pressure more than the single agent. As a part of the vascular protective benefit of ACEi had previously been attributed to blood pressure reduction, it was surprising to see no additional benefit with average BP 2.4/1.4 mmHg lower in the combined arm compared to ramipril treated patients. Perhaps maximal vascular protection had been achieved with ACEi or ARB alone, and a further reduction of BP and RAAS activity had no additional benefit.
Is there an indication for combined ACEi + ARB?
The combination of ACEi and ARB has not been proven to be an effective antihypertensive strategy and is not recommended by the Canadian Hypertensive Education Program (CHEP) unless there are other compelling reasons for combination therapy such as with heart failure or renal disease. The ONTARGET study shows that in the population studied there is no reason to combine ACEi and ARB. For patients with severe heart failure the CHARM OverallCitation20 study with candesartan appears to support combined therapy. However the choice and dose of ACEi was not specified and similar risk reductions were seen whether or not the patient was taking an ACEi. When the ACEi and dose were determined by the trial design as in VALIANTCitation25 and ONTARGET, there was no additional benefit from the combination of ACEi and ARB beyond that of the single agent.
Combined ACEi and ARB treatment appears to reduce proteinuria more than the individual agents. Whether this is a blood pressure lowering effect is uncertain. The only evidence to show that combined ACEi and ARB treatment slows the progression of renal disease comes from the COOPERATE study;Citation30 the results of which have recently been discredited and considered to be unreliable.Citation31
Was telmisartan better than placebo?
The results of the TRANSCEND study showed that there was no significant difference in either the primary or secondary outcomes in patients receiving either telmisartan or placebo. The secondary HOPE endpoint of death/MI/stroke appeared to be reduced by telmisartan, yet the difference did not remain statistically significant after adjustments for multiple comparisons. Does this mean telmisartan is no better than placebo, despite being shown to retain almost all the vascular protective properties of ramipril in the ONTARGET study? There are several possible reasons for this apparent discrepancy. Firstly that the TRANSCEND study was underpowered, with too low event rates and an inadequate follow-up period to show an ambitious 19% relative risk reduction. For the secondary HOPE endpoint the event rate in the placebo group of the TRANSCEND study was 3.2%/year but in the HOPE study the event rate was 4.4%/year. Yet in the EUROPA study, perindopril did show a 20% reduction of the combined endpoint of cardiovascular death/MI and cardiac arrest with lower event rates than were observed in the HOPE study and over a 4.2-year observation period.
A second possible explanation is the legacy effect of pre-treatment with either ACEi or ARB. The design and baseline characteristics paperCitation27 indicates that 58.1% of patients were receiving an ACEi and 29.9% an ARB at the time of randomization. In the HOPE-TOO study,Citation32 there were persistent benefits from the 5-year period of ramipril treatment, that remained for at least 3 (median 2.6 years) after the randomization period ended. A similar persistent legacy of treatment was observed in the AIREX study of post-myocardial heart failure.Citation33 Hence it is possible that the benefits of telmisartan were reduced because of the persistent legacy of pre-treatment with either ACEi or ARB in the placebo group.
Application of ONTARGET and TRANSCEND
The results of these two important trials indicate that for patients at high risk for vascular events, either ramipril or telmisartan can be used to reduce event rates. Whether a physician uses an ACEi or ARB for vascular protection will depend upon many factors, including habit, cost and adverse effects of treatment. Yet telmisartan was shown to be safe in ACEi intolerant patients and from the ONTARGET study preserved almost all the vasculoprotective benefits of ramipril. Telmisartan was well tolerated with less patients discontinuing treatment due to cough (telmisartan 93 vs ramipril 360) or angio-edema (10 vs 25). Although hypotension was more frequent with telmisartan (229 vs 149), the incidence of syncope was very similar (19 vs 15). Therefore it would not be unreasonable, despite the results of TRANSCEND, to recommend ARB usage in ACEi intolerant individuals. Guidelines have started to recommend ACEi and ARBs as alternative choices for vascular protection especially in high risk individuals with diabetes.Citation34
Disclosures
The author has no conflicts of interest to disclose.
References
- WagenaarLJVoorsAABuikemaHvan GilstWHAngiotensin receptors in the cardiovascular systemCan J Cardiol20021813311339
- YusufSTeoKKPogueJDyalLCoplandISchumacherHDagenaisGSleightPAndersonCTelmisartan, ramipril, or both in patients at high risk for vascular eventsN Engl J Med2008358151547155918378520
- The Telmisartan Randomised AssessmeNt Study in ACE iNtolerant subjects with cardiovascular Disease (TRANSCEND) Investigators. Effects of the angiotensin-receptor blocker telmisartan on cardiovascular events in high-risk patients intolerant to angiotensin-converting enzyme inhibitors: a randomised controlled trial. Lancet. Published on-line 29 August 2008, DOI:10.1016/S0140-6736(08)61242–1248
- DzauVJMechanism of protective effects of ACE inhibition on coronary artery diseaseEur Heart J199819Suppl JJ2J69796834
- BrownNJKumarSPainterCAVaughanDEACE inhibition versus angiotensin type 1 receptor antagonism: differential effects on PAI-1 over timeHypertension200240685986512468570
- KimMPZhouMWahlLMAngiotensin II increases human monocyte matrix metalloproteinase-1 through the AT2 receptor and prostaglandin E2: Implications for atherosclerotic plaque ruptureJ Leukoc Biol20057819520115817699
- The SOLVD investigatorsEffect of enalapril on survival in patients with reduced ejection fraction and congestive heart failureN Engl J Med19913252933022057034
- PfefferMABraunwaldEMoyeLAEffect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. Results of the survival and ventricular enlargement trial. The SAVE InvestigatorsN Engl J Med1992327106696771386652
- RutherfordJDPfefferMAMoyeLAEffects of captopril on ischemic events after myocardial infarction. Results of the Survival and Ventricular Enlargement trial. SAVE InvestigatorsCirculation1994904173117387923656
- YusufSSleightPPogueJBoschJDaviesRDagenaisGEffects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. The Heart Outcomes Prevention Evaluation Study Investigators (see comments)N Engl J Med2000342314515310639539
- The EURopean trial On reduction of cardiac events with Perindopril in stable coronary Artery disease InvestigatorsEfficacy of perindopril in reduction of cardiovascular events among patients with stable coronary artery disease: randomised double-blind, placebo-controlled, multicentre trial (the EUROPA study)Lancet200336278278813678872
- The PEACE InvestigatorsAngiotensin-Converting–Enzyme Inhibitionin Stable Coronary Artery DiseaseN Engl J Med20043512058206815531767
- DagenaisGRPogueJFoxKSimoonsMLYusufSAngiotensin-converting-enzyme inhibitors in stable vascular disease without left ventricular systolic dysfunction or heart failure: a combined analysis of three trialsLancet2006368953558158816905022
- DanchinNCucheratMThuillezCDurandEKadriZStegPGAngiotensin-converting enzyme inhibitors in patients with coronary artery disease and absence of heart failure or left ventricular systolic dysfunction: an overview of long-term randomized controlled trialsArch Intern Med2006166778779616606817
- GrangerCBErtlGKuchJRandomized trial of candesartan cilexetil in the treatment of patients with congestive heart failure and a history of intolerance to angiotensin-converting enzyme inhibitorsAm Heart J2000139460961710740141
- GrangerCBMcMurrayJJYusufSEffects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function intolerant to angiotensin-converting-enzyme inhibitors: the CHARM-Alternative trialLancet2003362938677277613678870
- BrennerBMCooperMEdeZEffects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathyN Engl J Med20013451286186911565518
- ParvingHHLehnertHBrochnerMGomisRAndersenSArnerPThe effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetesN Engl J Med20013451287087811565519
- PfefferMASwedbergKGrangerCBEffects of candesartan on mortality and morbidity in patients with chronic heart failure: the CHARM-Overall programmeLancet2003362938675976613678868
- McMurrayJJOstergrenJSwedbergKEffects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function taking angiotensin-converting-enzyme inhibitors: the CHARM-Added trialLancet2003362938676777113678869
- DemersCMcMurrayJJSvedbergKImpact of candesartan in preventing myocardial infarction: results of the Candesartan in Heart failure Assessment of Reduction in Mortality and Morbidity (CHARM) ProgrammeCirculation1102004Suppl IIIIII514
- DahlofBDevereuxRBKjeldsenSECardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenololLancet20023599311995100311937178
- JuliusSKjeldsenSEWeberMOutcomes in patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: the VALUE randomised trialLancet20043632022203115207952
- FlatherMDYusufSKoberLLong-term ACE-inhibitor therapy in patients with heart failure or left-ventricular dysfunction: a systematic overview of data from individual patients. ACE-Inhibitor Myocardial Infarction Collaborative Group (see comments)Lancet200035592151575158110821360
- PfefferMAMcMurrayJJVelazquezEJValsartan, captopril, or both in myocardial infarction complicated by heart failure, left ventricular dysfunction, or bothN Engl J Med2003349201893190614610160
- StraussMHHallASAngiotensin receptor blockers may increase risk of myocardial infarction: unraveling the ARB-MI paradoxCirculation2006114883885416923768
- TeoKKBurtonJRBullerCPlanteSYokoyamaSMontagueTJRationale and design features of a clinical trial examining the effects of cholesterol lowering and angiotensin-converting enzyme inhibition on coronary atherosclerosis: Simvastatin/Enalapril Coronary Atherosclerosis Trial (SCAT). SCAT InvestigatorsCan J Cardiol19971365915999215232
- MannJFSchmiederREMcQueenMRenal outcomes with telmisartan, ramipril, or both, in people at high vascular risk (the ONTARGET study): a multicentre, randomised, double-blind, controlled trialLancet2008372963854755318707986
- YusufSDienerHCSaccoRLTelmisartan to prevent recurrent stroke and cardiovascular eventsN Engl J Med2008
- NakaoNYoshimuraAMoritaHTakadaMKayanoTIdeuraTCombination treatment of angiotensin-II receptor blocker and angiotensin-converting-enzyme inhibitor in non-diabetic renal disease (COOPERATE): a randomised controlled trialLancet2003361935211712412531578
- KunzRWolbersMGlassTMannJThe COOPERATE trial: a letter of concernLancet20083711575157618468534
- HOPE/HOPE-TOO Study InvestigatorsResults of the HOPE study extension. long-term effects of ramipril on cardiovascular events and on diabetesCirculation20051121339134616129815
- HallASMurrayGDBallSGFollow-up study of patients randomly allocated ramipril or placebo for heart failure after acute myocardial infarction: AIRE Extension (AIREX) StudyLancet1997349149314979167457
- Canadian Diabetes Association Clinical Practice Guidelines Expert CommitteeCanadian Diabetes Association 2008 clinical practice guidelines for the prevention and management of diabetes in CanadaCan J Diabetes200832suppl 1S1S201