Abstract
Multidetector computed tomography has been shown to be accurate in noninvasive assessment of chest vascular disease. The motion artifacts of the thoracic aorta and the supra-aortic vessels were significantly reduced in the electrocardiogram (ECG)-gated data acquisition. This positive effect of ECG synchronization is more pronounced in the region of the ascending aorta, aortic arch, and proximal descending aorta.
Introduction
A variety of atypical imaging features, pitfalls, and artifact can occur during with computed tomography (CT) examination, which is a commonly used noninvasive imaging technique for the diagnosis of aortic dissection (CitationFisher et al 1994; CitationBatra et al 2000; CitationRaptopoulos et al 2006).
Motion artifacts caused by transmitted cardiac pulsation can frequently degrade thoracic CT studies. Some of these artifacts (eg, motion artifacts that mimic aortic dissection) are recognized as important sources of potential diagnostic errors (CitationLoubeyre et al 1997; CitationRubin 1997).
A typical diagnostic pitfall caused by such transmitted cardiac pulsation is an artifactual intimal flap, resembling dissection in the ascending aorta (CitationLoubeyre et al 1997).
Synchronization of the CT acquisition with the patient’s electrocardiogram (ECG) reduces cardiac motion artifacts and enables noninvasive visualization of the coronary arteries (CitationAchenbach et al 1998; CitationNieman et al 2001) and other cardiac anatomy (ascending aorta) (CitationWillmann et al 2002; CitationMorgan-Hughes et al 2003).
It has been shown that retrospective ECG gating can be beneficially employed for reducing transmitted cardiac pulsation also in more extensive scanning volumes in the thorax (CitationFlohr et al 2002; CitationRoos et al 2002). Retrospective ECG gating (CitationOhnesorge et al 2000) is the most commonly used strategy for ECG synchronization at multidetector row CT. Substantial effort has been invested in defining suitable time points during the cardiac cycle for reconstruction of CT data to provide optimal depiction of the coronary arteries (CitationHong et al 2001; CitationKopp et al 2001; CitationGiesler et al 2002).
Case report
A 69-year-old female with thoracic pain, left superior arm parestesia and radial pulse absence was referred to the emergency department of our institution. She had a medical history with several episodes of thoracic pain spontaneously resolved, hypertension treated with calcium blockers and hyperlipidemia with statin. Her paste medical history was free of cardiologic disease.
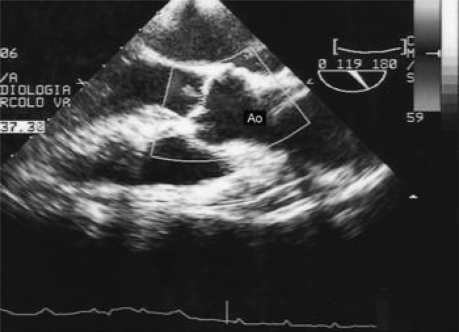
An ECG () was performed and it revealed normal findings for the heart and ascending aorta but considering clinical symptoms, a thoracic angio-CT was ordered.
Figure 1 Echocardiogram: no intimal flap is present.
An angiographic CT-scan with 64-multislice spiral scanners (Aquilion, Toshiba Europa Medical System) was performed before contrast media injection and after contrast media intravenous administration. Ninety-five milliliters (400 mg I/ml; flow 4 ml/s) (Iomeron, Bracco, Milan, Italy) were administred followed by a chaser bolus of 50 ml saline (flow 4 ml/s) using automatic dual-head injector (Stellant® D, MedRad, Indianola, Pennsylvania, USA).
Bolus chaser helps to flush the contrast bolus from the arm veins. A bolus tracking technique was used to synchronize the arrival of the contrast bolus in thoracic aorta. This technique consists of positioning a region of interest (ROI) in the ascending aorta; the scan will start when the attenuation value recorded in the ROI is higher than 100 HU, the attenuation value seen at baseline. When the attenuation value inside the ROI reaches a given threshold, the scan begins.
Cranio-caudal spiral scanning of the heart was performed after mild hyperventilation within a single breathhold at end-inspiratory suspension. CT angiography suspected an intimal flap of ascending aorta, involving aorta valve and with possible involvement coronary artery ostium (); also a possible thrombosed intimal tear of aorta arch was considered (). CT findings were conflicting with ecocardiography so a thoracic CT ECG-gated was considered and performed using the current protocol in our Institution (criteria in ).
Figure 2 CT-Angio without gating. Pulsation artifacts misappared of aortic valve (a-c) and aortic arch thrombus (MPR: b); suspected ascending aorta intimal flap (MPR: c)

Table 1 Results of thoracic CT ECG-gated examination
ECG-gated examination excluded intimal flap in the ascending aorta and showed the presence of a aorta arch dissection with a thrombus extending to innominate trunck, left common carotid artery and left subclavian artery and the presence of floating thrombus in aorta arch (, ).
Figure 3 CT-Angio ECG-gated. Excluded aortic valve dissection (a), showed thrombus of innominate trunk, left common carotid artery and left subclavian artery (b-c).
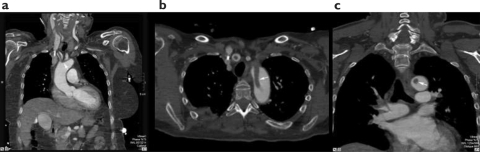
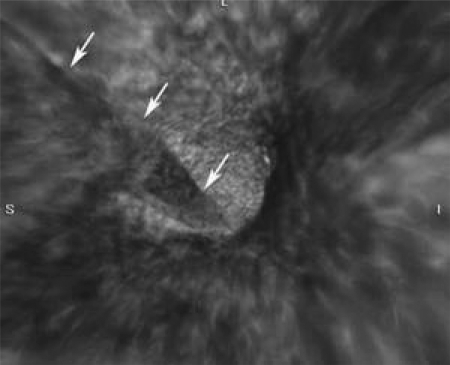
Figure 4 Virtual Endoscopy (3D EV): confirmed extension of aorta arch thrombus.
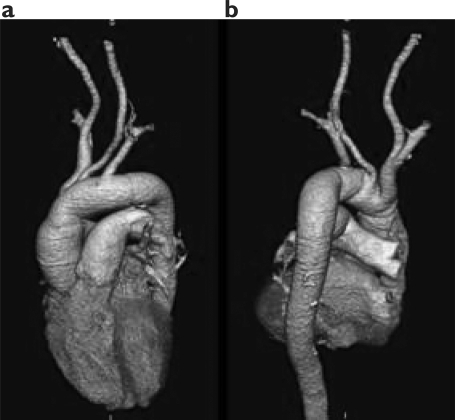
At this time, our patient underwent a surgical treatment. For the cardiopulmonary bypass, a retrograde femoral artery cannulation was used in combination with a two-stage venous cannula in the right atrium. Because of the total occlusion of the innominate artery, the right carotid artery was cannulated too. A standard median sternotomy was made. A pericardial tamponade had been found. Blood temperature was reduced to 20 °C and the circulation interrupted. The cerebral perfusion was maintained through the carotid cannula. The aortic arch was opened. No dissection was found into the ascending aorta. The intimal tear was in the transverse arch between the innominate and the subclavian artery. A red thrombus was present into the aortic arch and branched into the 3 supra-aortic vessels. The thrombus was removed and the aortic arch replaced with a 26 mm Dacron graft. The subclavian artery, the left carotid artery and the innominate artery were connected one by one to the graft ().
Figure 5 a-b Volume Rendering (3D VR): CT-Angio after sovraortic vessels debrunching.
Discussion
CT is an important tool for the evaluation of acute aortic dissection, which requires prompt and accurate diagnosis to initiate appropriate surgical intervention or medical treatment (CitationFisher et al 1994; CitationBatra et al 2000). A confident diagnosis of aortic dissection relies on the visualization of an intimal flap in the thoracic aorta and the presence of enhanced or thrombosed true and false lumens.
A variety of pitfalls were encountered that mimicked aortic dissection in CT examinations (CitationBatra et al 2000). These pitfalls were attributable to technical factors (eg, improper contrast material timing); streak artifacts generated by high attenuation materials or high contrast interfaces; aortic variations, such as congenital ductus diverticulum and acquired aortic aneurysm with thrombus; peri-aortic structures (eg, aortic arch branches); and, finally, streaks caused by cardiac pulsation and aortic wall motion. Although several of these pitfalls are easy to recognize and unlikely to present a diagnostic problem, others are potentially confusing.
In the study of CitationKo and colleagues (2005) aortic motion artifacts were frequently seen on thoracic MDCT, with an overall prevalence of 91.9%; thus, familiarity with these artifacts can help avoid false-positive interpretations, especially in patients with clinical presentations of severe chest pain.
Suppression of cardiac pulsation artifacts and aortic wall motion is not only important in the diagnosis or exclusion of aortic dissection, but also for the detection of pulmonary embolism (CitationSchoepf et al 2002).
In addition to enabling noninvasive visualization of the coronary arteries, ECG synchronization has been shown to improve CT image quality in other thoracic structures (CitationSchoepf et al 1999; CitationMontaudon et al 2001). In principle, retrospective ECG-gating enables a reduction of transmitted cardiac pulsation in more extensive scanning volumes.
A pseudodissection spiral artifact of the ascending thoracic aorta has been previously described, and segmental reconstruction has been proposed to correct this (CitationQanadli et al 1999; CitationMontaudon et al 2001). Retrospective gating eliminated this artifact on the axial images in our case, similar to the experience of CitationRoos and colleagues (2002). In our case, we observed motion artifacts both the axial and multiplanar (coronal) images (). Some authors observed more motion artifacts in multiplanar images than axial images. We ttributed these artifacts to segmental data collection during continuous table motion (CitationOhnesorge et al 2000; CitationJacobs et al 2002; CitationRoos et al 2002; CitationSchoepf et al 2004). These artifacts have been shown to be more pronounced with increasing heart rate and are also influenced by incorrect pitch or time reconstruction point in the R-R interval (CitationHong et al 2001; CitationChoi et al 2004; CitationHofmann et al 2004). For decreasing cardiac pulsation motion artifacts, the best results have been reported from studies in which prospective gating with nonhelical scanning was used (CitationSchoepf et al 1999; CitationBoehm et al 2003; CitationMarten et al 2003). Even in those studies, however, the clinical usefulness of the improved resolution was questionable.
Conclusion
In our experience MDCT ECG-gated could be useful to differentiate a “true” thrombosis of the sovraortic vessels from a thrombosis of the false lume dissection. Therefore it has contributed to not only characterize the cause of the thoracic pain but it has allowed correct preoperative assessment. In conclusion from the data found in the literature, the case matched our observation that the ECG-gated examination is mandatory every time a difference is present between CT imaging and clinical symptom in thoracic aorta disease.
References
- AchenbachSMoshageWRopersDValue of electron-beam computed tomography for the noninvasive detection of high-grade coronary-artery stenoses and occlusionsN Engl J Med19983391964719869667
- BatraPBigoniBManningJPitfalls in the diagnosis of thoracic aortic dissection at CT angiographyRadio Graphics20002030920
- BoehmTWillmannJKHilfikerPRThinsection CT of the lung: does electrocardiographic triggering influence diagnosis?Radiology20032294839114512510
- ChoiHSChoiBWChoeKOPitfalls, artifacts, and remedies in multi-detector row CT coronary angiographyRadioGraphics20042478780015143228
- EngJKrishnanJASegalJBAccuracy of CT in the diagnosis of pulmonary embolism: a systematic literature reviewAm J Roentgenol200418318192715547236
- FisherERSternEJGidwingJDAcute aortic dissection: typical and atypical imaging featuresRadio Graphics199414126371
- FlohrTProkopMBeckerCA retrospectively ECG-gated multislice spiral CT scan and reconstruction technique with suppression of heart pulsation artifacts for cardio-thoracic imaging with extended volume coverageEur Radiol200212149750312042960
- GieslerTBaumURopersDNoninvasive visualization of coronary arteries using contrast-enhanced multidetector CT: influence of heart rate on image quality and stenosis detectionAm J Roentgenol20021799111612239036
- HofmannLKZooKHCostelloPElectrocardiographically gated 16-section CT of the thorax: cardiac motion suppressionRadiology20042339273315486210
- HongCBeckerCRHuberAECG gated reconstructed multi – detector row CT coronary angiography: effect of varying trigger delay on image qualityRadiology20012207121711526271
- JacobsTFBeckerCROhnesorgeBMultislice helical CT of the heart with retrospective ECG gating: reduction of radiation exposure by ECGcontrolled tube current modulationEur Radiol2002121081611976849
- KoSFHsiehMJChenMCEffects of heart rate on motion artifacts of the aorta on non-ECG assisted 0.5-sec thoracic MDCTAm J Roentgenol200518412253015788600
- KoppAFSchroederSKuettnerACoronary arteries: retrospectively ECG-gated multi-detector row CT angiography with selective optimization of the image reconstruction windowRadiology2001221683811719663
- LoubeyrePAngelieEGrozelFSpiral CT artifact that simulates aortic dissection: image reconstruction with use of 180 degrees and 360 degrees linear-interpolation algorithmsRadiology199720515379314977
- MartenKEngelkeCFunkeMECG-gated multislice spiral CT for diagnosis of acute pulmonary embolismClin Radiol200358862814581010
- MontaudonMBergerPBlachereHThin-section CT of the lung: influence of 0.5-s gantry rotation and ECG triggering on image qualityEur Radiol2001111681711511889
- Morgan-HughesGJOwensPEMarshallAJThoracic aorta at multi – detector row CT: motion artifact with various reconstruction windowsRadiology2003228583812819333
- NiemanKOudkerkMRensingBJCoronary angiography with multi-slice computed tomographyLancet200135759960311558487
- OhnesorgeBFlohrTBeckerCCardiac imaging by means of electrocardiographically gated multisection spiral CT: initial experienceRadiology20002175647111058661
- QanadliSDEl HajjamMMesurolleBMotion artifacts of the aorta simulating aortic dissection on spiral CTJ Comput Assist Tomogr1999231610050797
- RaptopoulosVDBoisellePBMichailidisNMDCT angiography of acute chest pain: evaluation of ecg-gated and nongated techniquesAm J Roentgenol2006186S3465616714608
- RoosJWillmannJWeishauptDThoracic aorta: motion artifact reduction with retrospective and prospective electrocardiographyassisted multi–detector row CTRadiology2002222271711756736
- RubinGHelical CT angiography of the thoracic aortaJ Thorac Imaging199712128499179826
- SchoepfUJBeckerCRBrueningRDElectrocardiographically gated thinsection CT of the lungRadiology19992126495410478227
- SchoepfUJHolzknechtNHelmbergerTKSubsegmental pulmonary emboli: improved detection with thin-collimation multi-detector row spiral CTRadiology20022224839011818617
- SchoepfUJBeckerCROhnesorgeBNCT of coronary artery diseaseRadiology2004232183715220491
- WillmannJWeishauptDLachatMElectrocardiographically gated multi-detector row CT for assessment of valvular morphology and calcification in aortic stenosisRadiology2002225120812354994