Abstract
Cardiovascular disease is the leading cause of death worldwide. Within the treatment armamentarium, beta-blockers have demonstrated efficacy across the spectrum of cardiovascular disease – from modification of a risk factor (ie, hypertension) to treatment after an acute event (ie, myocardial infarction). Recently, the use of beta-blockers as a first-line therapy in hypertension has been called into question. Moreover, beta-blockers as a class are saddled with a misperception of having poor tolerability. However, vasodilatory beta-blockers such as carvedilol have a different hemodynamic action that provides the benefits of beta-blockade with the addition of vasodilation resulting from alpha 1-adrenergic receptor blockade. Vasodilation reduces total peripheral resistance, which may produce an overall positive effect on tolerability. Recently, a new, controlled-release carvedilol formulation has been developed that provides the clinical efficacy of carvedilol but is indicated for once-daily dosing. This review presents an overview of the clinical and pharmacologic carvedilol controlled-release data.
Beta-blockers in the treatment of cardiovascular disease
Cardiovascular disease (CVD) is the leading cause of morbidity and mortality, accounting for 30% of all deaths worldwide (CitationWorld Health Organization 2007). In the United States alone, CVD accounted for more than 36% of all deaths in 2004 or 1 of every 2.8 deaths (CitationAmerican Heart Association 2007). Blood pressure and CVD risk are directly proportional. In fact, mortality from ischemic heart disease and stroke doubles for every 20-mmHg increase in systolic blood pressure (SBP) or 10-mmHg increase in diastolic blood pressure (DBP) (CitationChobanian et al 2003). Furthermore, hypertension is often an antecedent to heart failure and myocardial infarction (MI). High blood pressure (>140/90 mmHg) has been identified in approximately 69% of Americans who have suffered a first MI and 74% of patients with chronic heart failure (CitationRosamond et al 2008). Therefore, it is not surprising that successful treatment of hypertension has been shown to reduce the risk of stroke, coronary artery disease (CAD), and congestive heart failure, as well as overall cardiovascular morbidity and mortality (CitationAugust 2003). However, optimal treatment benefits will not be observed unless patients adhere to their prescribed treatment regimens.
Adherence to prescribed medication regimens has been shown to be highest with once-daily dosing in several disease areas, and to decrease as the number of daily doses increase (CitationClaxton et al 2001; CitationFonarow 2006). In fact, decreased adherence to a medication regimen was shown to contribute to up to 64% of rehospitalizations in patients with heart failure (CitationLeventhal et al 2005; CitationFonarow 2006). However, tolerability also influences patient adherence to a medication regimen (CitationWeber et al 2006a; CitationCarter et al 2008).
Beta-blockers have a long history in the treatment of hypertension and cardiac dysfunction, with more than 40 years of clinical use (CitationFrishman 2007a). However, concerns have been raised recently from hypertension meta-analyses regarding suboptimal outcomes with use of beta-blockers, specifically atenolol, compared with outcomes for other antihypertensive drug classes (CitationLindholm et al 2005; CitationBangalore et al 2007b). Beta-blockers have also been associated with tolerability issues and concerns regarding negative effects on glucose and lipid metabolism. However, it should be noted that not all beta-blockers are identical, as differences in mechanism of action may translate into diverse efficacy and safety profiles (CitationFrishman 2003; CitationFrishman 2007a).
Carvedilol is a third-generation, vasodilatory beta-blocker that nonselectively blocks both the beta 1- and beta 2-adrenergic receptors and, in addition, has alpha 1-adrenergic receptor-blocking activity. Unlike traditional beta-blockers (eg, atenolol, metoprolol, and propranolol) that lower blood pressure by reducing cardiac output (CitationPacker 1998), vasodilatory beta-blockers can lower blood pressure by reducing systemic vascular resistance (SVR) (CitationSundberg et al 1987). As with other beta-blockers, carvedilol has been shown to reduce sympathetic nervous system (SNS)-mediated cardiac stress and myocardial hypertrophy (CitationToda 2003). These activities likely contribute to the clinical benefits observed in patients treated with carvedilol for hypertension, heart failure, and post-MI left ventricular dysfunction (LVD). Moreover, the regimen of twice-daily carvedilol has been associated with a favorable side effect and tolerability profile.
In order to improve adherence to therapy and to ease the pill burden on patients, a controlled-release formulation of carvedilol (carvedilol CR) was developed and is approved for use in the same indications (ie, hypertension, heart failure, and post-MI LVD) as immediate-release (IR) carvedilol. This review presents an overview of the clinical and pharmacologic carvedilol CR data.
Pharmacology of carvedilol
Mechanism of action
Traditional beta-blockers either selectively antagonize beta 1-adrenergic receptors (selective beta-blockade) or antagonize both beta 1- and beta 2-adrenergic receptors (nonselective beta-blockade). Although beta 1-selective agents are cardioselective, selectivity is dose dependent, and at high doses beta 1-selective agents may also antagonize beta 2-adrenergic receptors (CitationEgan et al 2005). Traditional beta-blockers reduce blood pressure primarily by decreasing cardiac output, and systemic vascular resistance is usually unchanged (CitationMesserli et al 2004). Inhibition of norepinephrine binding to beta-adrenergic receptors results in decreased heart rate and myocyte contractility (CitationPacker 1998).
Unlike traditional beta-blockers, carvedilol blocks norepinephrine binding to alpha 1-adrenegric receptors as well as beta 1- and beta 2-adrenegeric receptors (CitationPedersen et al 2007). Alpha 1-adrenergic receptors mediate vasoconstriction. Consequently, alpha 1-blockade results in vasodilation of the peripheral arteries, decreasing SVR (CitationPacker 1998; CitationFonarow 2004). In addition, preclinical evidence suggests that carvedilol can also produce nitric oxide-mediated vasodilation (CitationKozlovski et al 2006).
Carvedilol does not possess intrinsic sympathomimetic activity (CitationToda 2003). Intrinsic sympathomimetic activity induces weak stimulation of the beta-adrenergic receptors that may dampen the positive effects of beta 1-adrenergic receptor blockade (CitationEgan et al 2005; CitationFrishman 2007a). Of note, beta-blockers with intrinsic sympathomimetic activity have failed to demonstrate reductions in morbidity and mortality in patients with heart failure (CitationMaack et al 2000).
Carvedilol has also demonstrated antioxidant effects possibly attributable to stimulation of endothelial nitric oxide production or reduced nitric oxide inactivation (CitationToda 2003). Furthermore, carvedilol may protect against reactive oxygen species (ROS) through scavenging of free radicals, suppression of free radical generation, and prevention of ferric ion-induced oxidation (CitationToda 2003; CitationDandona et al 2007). The ability of carvedilol to scavenge free radicals has been correlated with improved outcomes in patients with heart failure and a recent MI (CitationGoldhammer et al 2007). In a study involving 39 patients with heart failure and a recent MI, carvedilol IR was shown to decrease oxygen free radical measurements using thiobarbituric acid reactive substances assay, thermochemoluminescence, and conjugated dienes methodologies in 29 patients (irrespective of dosage) after 6 months of treatment (CitationGoldhammer et al 2007). This decrease correlated with increased heart function (6-minute walk test; baseline, 332 m and at 6 months, 397 m; p < 0.05) compared with patients who had no evidence of reduced oxygen free radical measurements (6-minute walk test; baseline 326 m and at 6 months, 317 m; r = 0.83; p < 0.01) (CitationGoldhammer et al 2007). Moreover, patients with reduced oxygen free radical measurements had improved clinical outcomes within 1 year compared with patients who had no reduction (chronic heart failure hospital readmissions, 10% versus 50%, respectively; p < 0.01) and death rates (3% versus 20%, respectively; p < 0.01) (CitationGoldhammer et al 2007).
Antioxidant activities decrease elevated oxidative stress, which, in turn, reduces lipid peroxidation. Reduced lipid peroxidation may contribute to protection from myocardial and brain cell ischemic death in patients with hypertension, heart failure, ischemic heart disease, diabetes, and renal dysfunction (CitationMaggi et al 1996; CitationGiugliano et al 1997; CitationMoreno et al 1998; CitationNakamura et al 2002; CitationPadi et al 2002). Anti-oxidant activities of carvedilol may also inhibit low-density lipoprotein (LDL) oxidation, which could decrease accumulation of oxidized LDL in vessel walls (CitationMaggi et al 1996). In patients with heart failure, free fatty acid levels become elevated (possibly from SNS hyperactivity) and the myocardial rate of fatty oxidation may increase; however, during disease progression, myocardial energy efficiency is increased through a compensatory shift from the free fatty acid substrate to glucose (CitationStanley et al 2005). Preliminary clinical evidence suggests that pharmacologic treatments facilitating the compensatory metabolic switch at an earlier stage of disease may provide mortality benefits (CitationStanley et al 2005). Indeed, carvedilol has demonstrated decreased myocardial use of free fatty acids and either increased or neutral effects on myocardial glucose use in patients with heart failure (CitationWallhaus et al 2001; CitationPodbregar et al 2002; CitationAl-Hesayen et al 2005).
Carvedilol is also known to have anti-inflammatory properties. Inflammation has been linked to the pathogenesis of heart failure and atherosclerosis (CitationYang et al 2004; CitationTatli et al 2005). In a clinical trial in patients with hypertension and diabetes, carvedilol IR (12.5 mg twice daily) reduced pro-inflammatory markers, including plasma C-reactive protein and monocyte chemotactic protein-1 (CitationDandona et al 2007). Furthermore, carvedilol has been shown to decrease serum concentrations of the inflammatory cytokines IL-6 and TNF-α in patients with ischemic and nonischemic dilated cardiomyopathy (CitationKurum et al 2007).
In addition, carvedilol has been shown to stimulate beta-arrestin signaling (CitationWisler et al 2007). Beta-arrestin is involved in the desensitization process of β-receptors in response to catecholamines and is implicated in G protein-mediated cardiac remodeling in heart failure (CitationLefkowitz et al 2006; CitationPatel et al 2008). Recent results in animal models suggest that beta-arrestin G protein-independent signaling may also occur and provide cardioprotective effects (CitationPatel et al 2008). Furthermore, work is currently underway using beta-arrestin agonists such as carvedilol to form “super” beta-blockers that can turn off G protein-mediated signaling of the beta-receptor but still maintain the benefits of continued β-arrestin-mediated signaling on cell survival systems (CitationWisler et al 2007).
Pharmacokinetics and pharmacodynamics
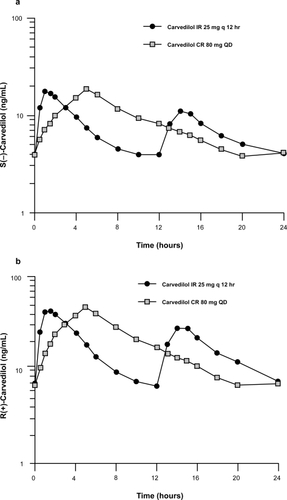
Carvedilol CR was developed to achieve sustained concentrations over a 24-hour period, allowing once-daily dosing. The pharmacokinetic and pharmacodynamic bioequivalence of carvedilol CR and IR was established through 2 clinical studies (CitationHenderson et al 2006; CitationPacker et al 2006). In a double-blind, parallel-group, crossover study, 122 patients with essential hypertension were randomized to receive either low-dose carvedilol CR (20 mg daily) or carvedilol IR (6.25 mg twice daily), high-dose carvedilol CR (80 mg once daily [initiated at 20 mg once daily and titrated to 40 mg and 80 mg once daily in 1-week intervals]) or carvedilol IR (25 mg twice daily [initiated at 6.25 mg twice daily and titrated to 12.5 mg and 25 mg twice daily in 1-week intervals]), or placebo (CitationHenderson et al 2006). After 22 days of treatment, patients were crossed over to the equivalent alternate carvedilol formulation for 8 days of treatment. Patients in the placebo treatment group continued to receive placebo throughout the study. Pharmacokinetic parameters were assessed at the end of each treatment session. The pharmacodynamic endpoint was the percentage change from baseline in exercise-induced heart rate. As carvedilol is a racemic mixture of R(+) and S(−) enantiomers (CitationNichols et al 1989), both forms were assessed in the pharmacokinetic analysis. The pharmacokinetic profiles of both enantiomers were equivalent between carvedilol CR and IR () (CitationHenderson et al 2006). In addition, both formulations maintained a reduced exercise-induced heart rate over a 24-hour period (CitationHenderson et al 2006).
Figure 1 Mean steady state concentration-time profiles for S(−) and R(+) enantiomers for carvedilol immediate-release and controlled-release. Reprinted from CitationHenderson LS, Tenero DM, Baidoo CA, et al 2006. Pharmacokinetic and pharmacodynamic comparison of controlled-release carvedilol and immediate-release carvedilol at steady state in patients with hypertension. Am J Cardiol, 98:17L–26L. Copyright © 2006, with permission from Elsevier.
In a separate 4-week study, patients with either mild to severe heart failure or with asymptomatic post-MI LVD were treated with the carvedilol IR (3.125, 6.25, 12.5, or 25 mg twice daily) for the first 2 weeks and then switched to carvedilol CR (10, 20, 40, or 80 mg once daily) for 2 weeks (CitationPacker et al 2006). Trough plasma concentration, maximum plasma concentration, and area under the curve was measured for both R(+) and S(−) enantiomers after carvedilol IR and CR treatment periods. The pharmacokinetics of carvedilol IR and CR were bioequivalent in patients with heart failure and post-MI with LVD. However, the median time to maximum observed plasma concentration for carvedilol CR lagged 3 hours behind that of carvedilol IR, in accordance with the prolonged-release characteristics expected in a once-daily formulation. The pharmacodynamics of carvedilol CR were dose proportional over the dose range tested (10 mg to 80 mg) (CitationPacker et al 2006).
Notably, the bioavailability of carvedilol CR is 85% that of carvedilol IR (CitationTenero et al 2006). Carvedilol CR is based on carvedilol phosphate, which has a higher molecular weight than carvedilol free base and contains additional carvedilol free base compared with carvedilol IR to adjust for bioavailability. This difference contributes, in part, to slightly higher milligram dosage strengths of carvedilol CR than the “equivalent” carvedilol IR doses (CitationTenero et al 2006). A model of carvedilol pharmacokinetics that takes into consideration both the IR and CR formulations has been developed and performed robustly in leverage analyses (CitationOthman et al 2007). Similar to carvedilol IR, the bioavailability and pharmacokinetics of carvedilol CR are influenced by food, and both formulations are recommended to be taken with food (CitationTenero et al 2006). However, the pharmacokinetics of carvedilol CR 40 mg were not affected by ethanol (38 g) intake from 2 hours before to 2 hours after dosing in 39 healthy volunteers (CitationHenderson et al 2007).
Implications of mechanism of action on metabolic effects and vascular health
Poor glycemic control predicts cardiovascular events; in particular, glycosylated hemoglobin levels linearly correlate with the risk of cardiovascular complications in patients with type 2 diabetes (CitationColagiuri et al 2002; CitationManley 2003). Moreover, dyslipidemia is a common comorbid condition in patients with hypertension (CitationJohnson et al 2004). Men with a serum cholesterol level greater than 253 mg/dL have been shown to have a relative risk of CAD 3.8 times greater than men who had levels less than 181 mg/dL (CitationStamler et al 1986). Traditional, nonvasodilating beta-blockers have been associated with worsening of glycemic control and impaired lipid metabolism (CitationBakris et al 2006a). In contrast, because of its vasodilatory mechanism of action, which facilitates muscle uptake of glucose and increases the availability of lipoprotein lipase, carvedilol does not negatively affect glycemic control or lipid profile compared with metoprolol (CitationMesserli et al 2004). Carvedilol CR is currently being studied in a randomized, double-blind clinical trial comparing lipid effects of metoprolol succinate extended release with carvedilol CR in patients with hypertension and either normal lipids or mild dyslipidemia (CitationBakris et al 2006b). The primary endpoints are the change from baseline in HDL-C and in triglycerides after 6 months of treatment. Several other trials have reported on glucose and lipid metabolism parameters using carvedilol IR and results have generally demonstrated improved profiles compared with metoprolol (CitationBakris et al 2004; CitationBasat et al 2006; CitationTorp-Pedersen et al 2007).
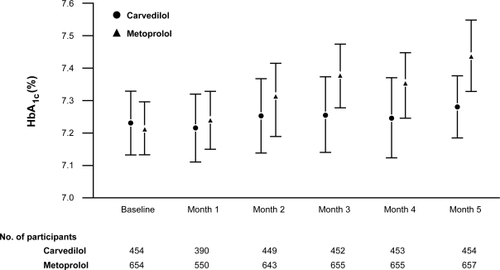
The Glycemic Effects in Diabetes Mellitus: Carvedilol-Metoprolol Comparison in Hypertensives (GEMINI) trial compared the effects of carvedilol IR (6.25 mg to 25 mg twice daily) with metoprolol (50 mg to 200 mg twice daily) on glycemic control and lipid profile in 1235 patients with diabetes and hypertension (CitationBakris et al 2004). After 5 months of treatment in this randomized, double-blind, parallel-group trial, carvedilol IR did not increase HbA1c (0.02%; p = 0.65), whereas metoprolol significantly increased HbA1c levels from baseline (0.15%; p < 0.001) (). Moreover, a greater number of patients withdrew because of worsening glycemic control in the metoprolol group (2.2%) compared with the carvedilol group (0.6%; p = 0.04). These data support the results of an earlier comparison study of metoprolol and carvedilol, which found that insulin sensitivity increased with carvedilol and decreased with metoprolol treatment (CitationJacob et al 1996).
Figure 2 Glycosylated hemoglobin (HbA1c) at baseline and each maintenance month by treatment in GEMINI. Reproduced with permission from CitationBakris GL, Fonseca V, Katholi RE, et al 2004. Metabolic effects of carvedilol vs metoprolol in patients with type 2 diabetes mellitus and hypertension: a randomized controlled trial. JAMA, 292:2227–36. Copyright © 2004, American Medical Association. All Rights Reserved.
Comparison of lipid parameters showed that carvedilol IR decreased total serum cholesterol levels to a greater extent than metoprolol (between-group difference, −2.9%; p = 0.001) in the GEMINI study (CitationBakris et al 2004). Carvedilol IR also decreased LDL cholesterol (LDL-C) compared with metoprolol (between-group difference, −1.3%; p = 0.40). In contrast with metoprolol, carvedilol did not significantly increase mean triglyceride levels. As kidney damage is a substantial concern for patients with hypertension and/or diabetes, kidney function was also measured in this study. Significant reductions in albumin secretion (16% relative reduction; p = 0.003) and progression to overt microalbuminuria were observed with carvedilol compared with metoprolol (p = 0.04).
The neutral effects of carvedilol on glycemic control and lipid metabolism have also been established in patients post-MI. Fifty-nine patients post-MI were randomized to add either metoprolol (100 mg twice daily) or carvedilol IR (25 mg twice daily) to their currently prescribed regimen for 12 weeks (CitationBasat et al 2006). After 12 weeks, patients receiving metoprolol had a significantly increased homeostasis model for insulin resistance (HOMA-IR), whereas carvedilol treatment significantly decreased HOMA-IR (p < 0.05 compared with baseline). In addition, carvedilol IR significantly decreased total cholesterol and LDL-C levels when compared with metoprolol (p = 0.043 and p = 0.021, respectively).
Treatment with carvedilol IR has been shown to reduce the incidence of diabetic events and new-onset diabetes among patients with heart failure. In the Carvedilol Or Metoprolol European Trial (COMET), 3029 patents with chronic heart failure were randomly assigned to treatment with target daily doses of carvedilol IR 50 mg or metoprolol tartrate 100 mg (CitationTorp-Pedersen et al 2007). In a cohort of 2298 patients without diabetes at trial initiation, diabetic events (adverse events of diabetic coma, peripheral gangrene, diabetic foot, decreased glucose tolerance, or hyperglycemia) and new-onset diabetes (clinical diagnosis, repeated high random glucose level, or glucose-lowering drugs) were assessed. Over a 5-year period, fewer diabetic events were reported with carvedilol IR (122 of 1151 patients; 10.6%) versus metoprolol (149 of 1147 patients; 13.0%; p = 0.039). New-onset diabetes (investigator reported) was also significantly less prevalent in the carvedilol IR treatment group (119 patients; 10.3%) compared with the metoprolol treatment group (145 patients; 12.6%; p = 0.048)
Efficacy of carvedilol in cardiovascular disease
The majority of clinical data for carvedilol come from studies with the IR formulation. However, several studies, both of bioequivalence and efficacy, have been conducted with carvedilol CR (CitationTenero et al 2006; CitationWeber et al 2006b). Carvedilol CR is indicated for the treatment of hypertension, mild to severe heart failure, and post-MI LVD – the same indications as carvedilol IR. Data presented in this section are a mixture of carvedilol IR and CR studies.
Hypertension
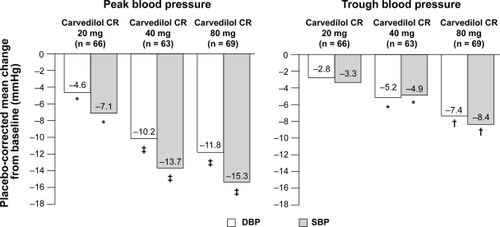
The efficacy of carvedilol CR in the treatment of hypertension was established in a double-blind, parallel-group trial in which patients with essential hypertension (N = 338) were randomized to receive carvedilol 20, 40, or 80 mg or placebo once daily after a 4-week washout period (CitationWeber et al 2006a; CitationWeber et al 2006b). Change from baseline in DBP measured by 24-hour ambulatory blood pressure monitoring after 6 weeks of treatment was the primary endpoint (CitationWeber et al 2006a). The patient population consisted of a mixture of patients, including those who were not receiving antihypertensive treatment, those with controlled hypertension (DBP < 90 mmHg) who were receiving antihypertensive treatment at baseline, and those with uncontrolled hypertension (DBP ≥ 90 mmHg) despite treatment with ≤2 non-beta-blocker antihypertensive agents at baseline. Mean sitting SBP and DBP at baseline were 150 mmHg and 99 mmHg, respectively, indicating a population with stage 1 hypertension (CitationChobanian et al 2003). Placebo-adjusted change from baseline in 24-hour DBP was −4.03, −7.56, and −9.19 mmHg, respectively, with carvedilol CR 20, 40, and 80 mg (p ≤ 0.001) (CitationWeber et al 2006a). Significant reductions in placebo-adjusted 24-hour SBP were also observed (−6.12, −9.43, and −11.85 mmHg, respectively) (CitationWeber et al 2006b). Carvedilol CR treatment resulted in significant, dose-dependent reductions in peak and trough blood pressure measurements (). Blood pressure control, defined as DBP < 90 mmHg, was achieved by 45% to 53% of patients treated with carvedilol compared with only 15% of patients who received placebo. Pulse pressure was assessed via an ad hoc analysis and was significantly reduced with carvedilol versus placebo (p < 0.05).
Figure 3 Controlled-release carvedilol in hypertension. Adapted from Weber MA, Sica DA, Tarka EA, et al Controlled-release carvedilol in the treatment of essential hypertension. Am J Cardiol, 98:32L–38L. Copyright © 2006, with permission from Elsevier.
Note: Data are change from baseline in model-adjusted peak (3 to 7 hours) diastolic blood pressure and systolic blood pressure measured by ambulatory blood pressure monitoring. *p < 0.05, †p < 0.001, ‡p < 0.0001, based on pair-wise comparison of change from baseline with placebo.
These data build on the established safety and efficacy of carvedilol IR in the treatment of hypertension demonstrated in several US and international placebo-controlled trials. In patients with hypertension, carvedilol IR has been shown to reduce blood pressure and exercise and resting heart rates (CitationPedersen et al 2007). Blood pressure reductions are likely linked to reductions in SVR in addition to the other BP-lowering properties of all beta-blockers, which have been demonstrated in healthy volunteers treated with carvedilol IR (CitationSundberg et al 1987).
The antihypertensive efficacy of carvedilol has been reported in patients with hypertension and comorbid conditions, such as diabetes, which make hypertension more difficult to treat (CitationBakris et al 2004; CitationWright et al 2007). In the previously described GEMINI trial, carvedilol IR lowered SBP by 18.1 mmHg and DBP by 9.9 mmHg, which was consistent with the 16.9 mmHg and 9.5 mmHg decreases in SBP and DBP, respectively, observed with metoprolol (CitationBakris et al 2004). At the end of the beta-blocker titration period, 37% and 36% of patients treated with carvedilol IR and metoprolol, respectively, achieved blood pressure goals (<130/80 mmHg for patients with diabetes) (CitationWright et al 2007). It should be noted that patients enrolled in this study were already receiving a stable regimen of antihypertensive therapy with an angiotensin-converting enzyme (ACE) inhibitor or an angiotensin-receptor blocker.
Carvedilol CR has demonstrated efficacy in the treatment of hypertension providing blood pressure control in up to 53% of the clinical patient population, which included patients with uncontrolled hypertension already receiving other classes of antihypertensive agents (CitationWeber et al 2006a). Additionally, based on the results of trials conducted with carvedilol IR, carvedilol CR may provide an equivalent extent of efficacy in more difficult to treat patients such as those patients with hypertension and diabetes.
Heart failure
Along the cardiovascular continuum, heart failure is a natural progression of uncontrolled hypertension. A recently completed trial in patients with heart failure compared the effects of carvedilol CR with those of carvedilol IR. Coreg: A Multicenter, Randomized, Double-Blind, Double-Dummy, Parallel-Group Study to Compare Effects of Coreg CR and Coreg IR on Ejection Fraction in Subjects With Stable Heart Failure (COMPARE) trial randomized patients with mild to severe heart failure and a left ventricular ejection fraction of 40% (N = 253) to either carvedilol CR (from 10 to 80 mg once daily) or carvedilol IR (from 3.125 to 25 mg twice daily) for up to 8 months (CitationGreenberg et al 2006). The primary efficacy endpoint was the change from baseline in left ventricular end-systolic volume index at 6 months. Secondary endpoints included change from baseline in left ventricular remodeling and serum B-type natriuretic peptide, hospitalization for heart failure and all other causes, death from all causes, compliance, and safety and tolerability of carvedilol CR. Full results are not yet published.
The beneficial effects of carvedilol IR have been demonstrated along the spectrum of severity from mild to severe heart failure (CitationFrishman 1998). The Australia/New Zealand (ANZ) double-blind trial randomized 415 patients with chronic, stable, mild heart failure to receive either carvedilol IR (from 3.125 mg to 25 mg, as tolerated) or placebo twice daily for 12 months (CitationAustralia/New Zealand Heart Failure Research Collaborative Group 1997). Carvedilol IR increased left ventricular ejection fraction from baseline by 5.1% at 12 months and decreased left-ventricular and end-systolic dimensions by 1.7 mm and 3.2 mm, respectively, compared with placebo. After a mean follow-up of 19 months, carvedilol IR decreased the combined risk of death or hospitalization in patients with heart failure risk by 26% versus placebo.
The US Carvedilol Heart Failure Study Group enrolled 1094 patients with mild to severe heart failure in a double-blind, stratified program, assigning patients to 1 of 4 treatment protocols on the basis of their exercise capacity (CitationPacker et al 1996). The mortality and hospitalization data from these 4 trials were analyzed together and considered together by the Data and Safety Monitoring Board for the trial. Patients were randomized to receive carvedilol IR (from 6.25 to 50 mg, if tolerated) or placebo twice daily and were followed for 6 months (12 months for the mild heart failure group). Compared with placebo, carvedilol IR significantly reduced mortality rates (3.2% versus 7.8%; p < 0.001), risk of hospitalization for cardiovascular causes (14.1% versus 19.6%; p = 0.036), and the combined endpoint of hospitalization or death (15.8% versus 24.6%; p < 0.001). The program was stopped early based on the significant improvements in survival with carvedilol IR compared with placebo. This finding is notable as the patients were only followed for an average of 6.5 months, which is a treatment period usually considered too short in duration to observe an effect on mortality and morbidity rates.
The Carvedilol Prospective Randomized Cumulative Survival (COPERNICUS) study randomized 2289 patients with symptoms of heart failure at rest or on minimal exertion with a left ventricular ejection fraction of <25% (ie, severe heart failure) to receive either placebo or carvedilol IR, (from 3.125 mg to 25 mg, as tolerated) (CitationPacker et al 2002). Treatment with carvedilol IR resulted in a 27% reduction of the combined endpoint of death or hospitalization for a cardiovascular reason (p < 0.0001 versus placebo), as well as a 31% reduction in the combined endpoint of death or hospitalization for heart failure (p < 0.001 versus placebo). Carvedilol IR treatment also significantly reduced the frequency of serious adverse events, including worsening heart failure, sudden death, cardiogenic shock, and ventricular tachycardia (p = 0.002 versus placebo).
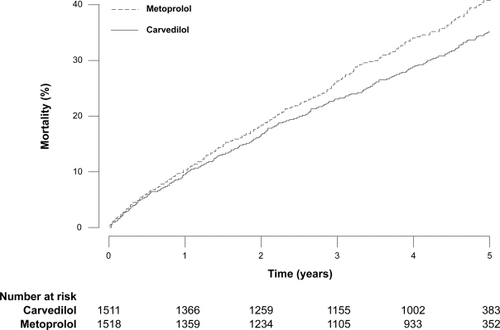
Additionally, over a mean duration of 58 months in the COMET study, significantly fewer deaths occurred in the carvedilol group (512 of 1511 patients; 34%) compared with the metoprolol group (600 of 1518 patients; 40%; p = 0.0017) () (CitationPoole-Wilson et al 2003). Cardiovascular death was less prevalent in the carvedilol group than in the metoprolol group (438 versus 534 patients; p = 0.0004), as were sudden death, circulatory failure, and stroke (CitationPoole-Wilson et al 2003; CitationTorp-Pedersen et al 2005). Results for the combined endpoint of all-cause mortality or all-cause admissions were similar in both groups (74% and 76% of patients for carvedilol IR and metoprolol, respectively). It should be noted that metoprolol tartrate at 50 mg twice daily has not been shown in clinical trials to provide a mortality benefit. However, of note in the metoprolol succinate heart failure trial (MERIT-HF), the mean daily dose was 159 mg daily, which is equivalent to 106 mg daily of metoprolol tartrate (CitationPoole-Wilson et al 2003).
Figure 4 Kaplan-Meier estimates of all-cause mortality in COMET. Reprinted from Poole-Wilson PA, Swedberg K, Cleland JG, et al Comparison of carvedilol and metoprolol on clinical outcomes in patients with chronic heart failure in the Carvedilol Or Metoprolol European Trial (COMET): randomised controlled trial. Lancet, 362:7–13. Copyright © 2003, with permission from Elsevier.
Another long-term study that compared carvedilol IR (49 mg daily) with metoprolol tartrate (124 mg daily) in patients with chronic heart failure (N = 150) demonstrated a greater decrease in exercise heart rate with carvedilol than with metoprolol after 13 to 15 months of treatment (p = 0.006) (CitationMetra et al 2000). In contrast, a recent trial comparing carvedilol IR (32 mg daily) and metoprolol succinate (96 mg daily) in a similar patient population (N = 37) observed a significant increase in exercise heart rate with carvedilol versus metoprolol (135 ± 4 versus 117 ± 6 beats/minute, respectively; p = 0.02), although peak exercise norepinephrine levels were similar (2736 ± 320 versus 2403 ± 372 pg/mL, respectively) (CitationVittorio et al 2008). These findings are of note because attenuation of exercise-induced heart rate is used as a surrogate for the extent of beta 1-adrenergic blockade and possibly to evaluate dosing equivalency. Many reasons may contribute to the results of these trials, including nonequivalent doses or different formulations or durations of treatment.
Post-MI LVD
Carvedilol is currently the only beta-blocker approved for use in patients with post-MI LVD. The only clinical data available in this patient population is with carvedilol IR. The Carvedilol Post-Infarct Survival Control in LV Dysfunction (CAPRICORN) study investigated the benefits of a beta-blocker (carvedilol IR) in patients with post-MI LVD who were receiving standard therapy. In this double-blind trial, 1959 patients who had experienced an MI and had a left ventricular ejection fraction ≤40% were randomized to receive either carvedilol IR (from 6.25 mg up to 25 mg as tolerated) or placebo twice daily (CitationDargie 2001). The mean follow-up duration was 1.3 years, and 74% of patients achieved the maximum dose of carvedilol IR (25 mg twice daily). In this study, carvedilol IR decreased all-cause mortality by 23% versus placebo (). However, there was no significant difference between groups in the composite endpoint of all-cause mortality or cardiovascular hospital admission. Data from CAPRICORN showed that carvedilol IR has antiar-rhythmic effects post-MI (CitationMcMurray et al 2005). Moreover, a substudy from CAPRICORN reported positive effects of carvedilol IR on ventricular remodeling (CitationDoughty et al 2004). The authors speculate that the influence on ventricular remodeling may be a substantial contributing factor to the clinical efficacy observed in patients with post-MI LVD. More recently, Fonarow and colleagues assessed the 30-day outcomes from CAPRICORN. Reductions with carvedilol IR versus placebo were observed in mortality, fatal or nonfatal MI; the composite endpoint of death, nonfatal MI, or cardiac arrest; and the composite endpoint of all-cause mortality or nonfatal MI (CitationFonarow et al 2007).
Figure 5 Kaplan-Meier estimates of event-free survival in CAPRICORN. Reprinted from Dargie HJ, for the CAPRICORN Investigators. Effect of carvedilol on outcome after myocardial infarction in patients with left-ventricular dysfunction: the CAPRICORN randomised trial. Lancet, 357:1385–90. Copyright © 2001, with permission from Elsevier.
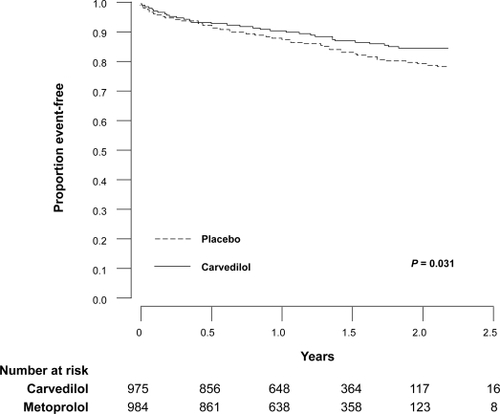
Based on the CAPRICORN data, the number needed to treat to prevent 1 death for 1 year was 43 (CitationOtterstad et al 2002). This compares favorably with data from the atenolol Beta-Blocker Heart Attack Trial (BHAT) showing that 80 patients would need treatment for 1 year to prevent 1 death (CitationOtterstad et al 2002). In contrast, the Norwegian Timolol Trial reported that 25 patients needed treatment for 1 year to prevent 1 death (CitationOtterstad et al 2002).
Safety and tolerability of carvedilol CR
The clinical utility of traditional beta-blockers has been limited by concerns regarding negative effects on glucose and lipid metabolism (CitationBakris et al 2006a; CitationBangalore et al 2007b) and a high incidence of side effects, including fatigue, erectile dysfunction, and weight gain (CitationBangalore et al 2007b). Unlike traditional beta-blockers, the alpha 1-blocking vasodilatory activity with carvedilol does not interfere with glucose and lipid metabolism (discussed previously) and has a positive influence on its tolerability profile.
Carvedilol CR is generally well tolerated across its therapeutic indications (CitationHenderson et al 2006; CitationPacker et al 2006; CitationWeber et al 2006a). Adverse events reported in clinical trials were consistent with the mechanism of action of carvedilol and the health status of the patient population under evaluation. In the bioequivalence study in patients with hypertension (N = 122), the proportion of patients who experienced an adverse event was lower with carvedilol CR compared with carvedilol IR (CitationHenderson et al 2006). Moreover, headache, orthostatic hypotension, diarrhea, and dizziness occurred more frequently with carvedilol IR than with carvedilol CR () (CitationHenderson et al 2006). It must be acknowledged, however, that this was a small study (122 patients) of short duration (approximately 5 weeks). The adverse event profile was comparable between carvedilol IR and carvedilol CR among patients with heart failure or post-MI enrolled in a pharmacokinetics study, with no notable increase in events when patients were switched from carvedilol IR to CR (CitationPacker et al 2006). In the carvedilol CR hypertension efficacy study, the occurrences of fatigue, dizziness, and headache were comparable between the combined carvedilol dose groups and the placebo group (CitationWeber et al 2006a).
Table 1 Treatment-related adverse events with IR and CR carvedilolTable Footnotea
Potential for improving patient adherence to therapy
Reducing pill burden
Use of multiple concomitant medications in the treatment of hypertension, heart failure, and MI contributes to the polypharmacy that is common among patients receiving carvedilol. Combinations of diuretics, ACE inhibitors, digitalis, glycosides, and beta-blockers are common in the treatment regimen for patients with heart failure. After an MI, guidelines recommend treatment with multiple evidence-based medications, including aspirin, clopidogrel, a statin, an ACE inhibitor, and a beta-blocker. In the field of hypertension, few patients achieve adequate blood pressure control on monotherapy (CitationBangalore et al 2007a). In fact, in ALLHAT, a mean of 2 drugs was required to reach blood pressure targets (CitationCushman et al 2002). Couple these findings with the treatment regimens for common comorbidities (eg, diabetes, coronary artery disease), and the pill burden can become quite substantial.
Both the number of pills taken daily and frequency of dosing affect patient adherence to prescribed therapies, and adherence, in turn, influences clinical outcomes (CitationClaxton et al 2001). In patients with hypertension, lack of adherence has been shown to reduce treatment benefit and increase the risk of poor treatment outcome (CitationFrishman 2007b). Among patients post-MI, lack of adherence to statins, calcium channel blockers, and beta-blockers significantly increased mortality risk (p = 0.001) (CitationRasmussen et al 2007).
One method for reducing pill burden is to design drugs that can be dosed less frequently. One such example is carvedilol CR. Once-daily dosing has been shown to improve adherence (CitationFrishman 2007b). Data compiled from 76 studies covering a range of therapeutic areas demonstrated that once-daily dosing is associated with the highest adherence rate among various dosing regimens (CitationClaxton et al 2001).The levels of adherence declined as the number of daily doses increased (79% for once daily, 69% for twice daily, 65% for 3 times daily, and 51% for 4 times daily). Moreover, the adherence benefit of once-daily dosing has been specifically observed with a beta-blocker (metoprolol) used for the treatment of hypertension (CitationBaird et al 1984).
The Compliance and Quality of Life Study Comparing Once-Daily Controlled-Release Carvedilol CR and Twice-Daily Immediate-Release Carvedilol IR in Patients with Heart Failure (CASPER) trial was based on the assumptions that adherence to the medication regimen would be 75% with twice-daily medication and 90% with once-daily medication (CitationHauptman et al 2006). Patients with mild to severe heart failure and a left ventricular ejection fraction of 40% or less were randomized to either a double-blind arm (morning carvedilol CR plus an evening placebo versus morning and evening carvedilol IR) or to an open-label arm (carvedilol CR). However, preliminary results demonstrated no difference in patient adherence between once-daily and twice-daily regimens (88% versus 89%) (CitationUdelson et al 2007; CitationCarter et al 2008). These results may be explained, in part, by the consideration that patient adherence may be higher in clinical trials than in the community setting. Indeed, the carvedilol IR recipients in this trial had a higher than anticipated compliance rate.
Another option for reducing pill burden is to reduce the number of individual pills through use of a fixed-dose combination (FDC). Fixed-dose combinations have become increasingly common in the field of hypertension because of the frequent need for multiple concomitant antihypertensives to control blood pressure. Fixed-dose combinations may also work synergistically, resulting in a lower total dose of each individual drug (CitationRao et al 1998). The ability to reduce drug doses can also reduce the risk of side effects. Use of an FDC may also have positive effects on patient adherence. In a study comparing adherence between patients treated with an FDC (n = 11,925) and patients treated with a free-drug regimen (n = 8317), those receiving an FDC had a significantly decreased risk of nonadherence (p < 0.0001) (CitationBangalore et al 2007a).
An FDC consisting of carvedilol and the ACE inhibitor lisinopril is currently in development. The Coreg and Lisinopril Combination Therapy in Hypertensive Subjects (COSMOS) trial is assessing the efficacy and safety of a carvedilol/lisinopril FDC (ClinicalTrials.gov Identifier: NCT00347360). COSMOS is a randomized, double-blind, double-dummy, parallel-group trial employing a 4 × 4 factorial design that will evaluate carvedilol (20, 40, or 80 mg daily) alone, lisinopril (10, 20, or 40 mg daily) alone, and all permutations of the combined drugs in patients with hypertension.
Quality of life and patient satisfaction
Quality of life is more difficult to assess than concrete measures such as blood pressure or mortality. If improved tolerability and reduced risk for side effects were considered, one would anticipate an improvement in this category with carvedilol as appraised relative to traditional beta-blockers.
Some clinical trials have revealed improvements in patient-reported quality-of-life assessments. The effects of carvedilol IR on patient global assessment were reported in patients with heart failure (CitationPacker et al 2002). In a study of 2289 patients with heart failure, patients receiving treatment with carvedilol were more likely to show moderate or marked improvement and less likely to show moderate or marked worsening versus placebo. In the previously described COMET study, a patient-completed, self-assessment scoring system that was evaluated every 4 months of treatment demonstrated a significantly improved self-score for patients treated with carvedilol (p < 0.0068) (CitationCleland et al 2006).
A prespecified secondary analysis of the GEMINI study used the Diabetes Symptom Checklist to record patient-reported occurrences of diabetes-related symptoms in 8 domains, namely psychology (fatigue), psychology (cognitive), neuropathy (pain), neuropathy (sensory), cardiology, ophthalmology, hyperglycemia, and hypoglycemia (CitationMcGill et al 2007). After 5 months of treatment, the results significantly favored carvedilol over metoprolol tartrate in overall maintenance score (p = 0.02), hypoglycemia symptoms (p = 0.02), and hyperglycemia symptoms (p = 0.005).
Conclusions
The varied mechanisms of action of carvedilol allow it to be an effective treatment of hypertension, heart failure, and post-MI LVD, with less of the metabolic and tolerability concerns associated with traditional beta-blockers. The key difference from the majority of beta-blockers appears to be vasodilation mediated by alpha 1-adrenergic receptor blockade, which decreases total peripheral resistance (CitationPedersen et al 2007). Furthermore, carvedilol’s antioxidant and anti-inflammatory effects may provide additional car-dioprotective effects beyond that of traditional beta-blockers (CitationDandona et al 2007). Carvedilol has a long history and a proven track record in the treatment of hypertension and cardiac dysfunction. The once-daily formulation of carvedilol provides a more convenient option and may confer an adherence benefit over the twice-daily formulation in conditions traditionally prone to noncompliance such as hypertension and post-MI LVD.
Acknowledgements
The authors would like to thank Tamalette Loh, PhD, ProEd Communications, Inc.®, for her medical editorial assistance with this manuscript.
Disclosures
The authors have no conflicts of interest to disclose.
References
- Al-HesayenAAzevedoERFlorasJS2005Selective versus non-selective beta-adrenergic receptor blockade in chronic heart failure: differential effects on myocardial energy substrate utilizationEur J Heart Fail76182315921803
- American Heart Association2007Heart Disease and Stroke Statistics – 2007 UpdateDallas, TexasAmerican Heart Association
- AugustP2003Initial treatment of hypertensionN Engl J Med348610712584370
- Australia/New Zealand Heart Failure Research Collaborative Group1997Randomised, placebo-controlled trial of carvedilol in patients with congestive heart failure due to ischaemic heart disease. Australia/New Zealand Heart Failure Research Collaborative GroupLancet349375809033462
- BairdMGBentley-TaylorMMCarruthersSG1984A study of efficacy, tolerance and compliance of once-daily versus twice-daily metoprolol (Betaloc) in hypertension. Betaloc Compliance Canadian Cooperative Study GroupClin Invest Med7951026380858
- BakrisGLFonsecaVKatholiRE2004Metabolic effects of carvedilol vs metoprolol in patients with type 2 diabetes mellitus and hypertension: a randomized controlled trialJAMA29222273615536109
- BakrisGLHartPRitzE2006aBeta blockers in the management of chronic kidney diseaseKidney Int7019051317021610
- BakrisGLTarkaEAWaterhouseB2006bCardiovascular risk factors in hypertension: rationale and design of studies to investigate the effects of controlled-release carvedilol on regression of left ventricular hypertrophy and lipid profileAm J Cardiol9846L52L
- BangaloreSKamalakkannanGParkarS2007aFixed-dose combinations improve medication compliance: a meta-analysisAm J Med120713917679131
- BangaloreSMesserliFHKostisJB2007bCardiovascular protection using beta-blockers: a critical review of the evidenceJ Am Coll Cardiol505637217692739
- BasatOUcakSSeberS2006After myocardial infarction carvedilol improves insulin resistance compared to metoprololClin Res Cardiol959910416598518
- CarterNJKeatingGM2008Controlled-release carvedilolAm J Cardiovasc Drugs82718218690761
- ChobanianAVBakrisGLBlackHR2003Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood PressureHypertension4212065214656957
- ClaxtonAJCramerJPierceC2001A systematic review of the associations between dose regimens and medication complianceClin Ther23129631011558866
- ClelandJGCharlesworthALubsenJ2006A comparison of the effects of carvedilol and metoprolol on well-being, morbidity, and mortality (the “patient journey”) in patients with heart failure: a report from the Carvedilol Or Metoprolol European Trial (COMET)J Am Coll Cardiol4716031116630997
- ColagiuriSCullCAHolmanRR2002Are lower fasting plasma glucose levels at diagnosis of type 2 diabetes associated with improved outcomes? UK prospective diabetes study 61Diabetes Care251410712145243
- CushmanWCFordCECutlerJA2002Success and predictors of blood pressure control in diverse North American settings: the anti-hypertensive and lipid-lowering treatment to prevent heart attack trial (ALLHAT)J Clin Hypertens (Greenwich)439340412461301
- DandonaPGhanimHBrooksDP2007Antioxidant activity of carvedilol in cardiovascular diseaseJ Hypertens257314117351362
- DargieHJ2001Effect of carvedilol on outcome after myocardial infarction in patients with left-ventricular dysfunction: the CAPRICORN randomised trialLancet35713859011356434
- DoughtyRNWhalleyGAWalshHA2004Effects of carvedilol on left ventricular remodeling after acute myocardial infarction: the CAPRICORN Echo SubstudyCirculation109201614707020
- EganBMBasileJChiltonRJ2005Cardioprotection: the role of beta-blocker therapyJ Clin Hypertens (Greenwich)74091616015051
- FonarowGC2004Managing the patient with diabetes mellitus and heart failure: issues and considerationsAm J Med116Suppl 5A76S88S15019865
- FonarowGC2006Profile of carvedilol controlled-release: a new once-daily formulation of carvedilolExpert Opin Pharmacother725334617150007
- FonarowGCLukasMARobertsonM2007Effects of carvedilol early after myocardial infarction: analysis of the first 30 days in Carvedilol Post-Infarct Survival Control in Left Ventricular Dysfunction (CAPRICORN)Am Heart J1546374417892984
- FrishmanWH1998CarvedilolN Engl J Med3391759659845712
- FrishmanWH2003Alpha- and beta-adrenergic blocking drugsFrishmanWHSonnenblickEHSicaDACardiovascular pharmacotherapeutics2nd edNew YorkMcGraw Hill6797
- FrishmanWH2007aA historical perspective on the development of beta-adrenergic blockersJ Clin Hypertens94 Suppl 31927
- FrishmanWH2007bImportance of medication adherence in cardiovascular disease and the value of once-daily treatment regimensCardiol Rev152576317700384
- GiuglianoDAcamporaRMarfellaR1997Metabolic and cardiovascular effects of carvedilol and atenolol in non-insulin-dependent diabetes mellitus and hypertension. A randomized, controlled trialAnn Intern Med12695599182472
- GoldhammerEMaorIShnitzerS2007The early anti-oxidant effect of carvedilol predicts the clinical course in congestive heart failure patientsJ Cardiovasc Med (Hagerstown)8453617502762
- GreenbergBHMehraMTeerlinkJR2006COMPARE: comparison of the effects of carvedilol CR and carvedilol IR on left ventricular ejection fraction in patients with heart failureAm J Cardiol9853L9L
- HauptmanPJPresslerSJSackner-BernsteinJ2006Rationale and design of CASPER: compliance and quality of life study comparing once-daily carvedilol CR and twice-daily carvedilol IR in patients with heart failureAm J Cardiol9860L6L16784921
- HendersonLSTeneroDMBaidooCA2006Pharmacokinetic and pharmacodynamic comparison of controlled-release carvedilol and immediate-release carvedilol at steady state in patients with hypertensionAm J Cardiol9817L26L
- HendersonLSTeneroDMCampanileAM2007Ethanol does not alter the pharmacokinetic profile of the controlled-release formulation of carvedilolJ Clin Pharmacol4713586517962424
- JacobSRettKWicklmayrM1996Differential effect of chronic treatment with two beta-blocking agents on insulin sensitivity: the carvedilol-metoprolol studyJ Hypertens14489948761899
- JohnsonMLPietzKBattlemanDS2004Prevalence of comorbid hypertension and dyslipidemia and associated cardiovascular diseaseAm J Manag Care109263215617368
- KozlovskiVILomnickaMChlopickiS2006Nebivovol and carvedilol induce NO-dependent coronary vasodilatation that is unlikely to be mediated by extracellular ATP in the isolated guinea pig heartPharmacol Rep58Suppl1031017332679
- KurumTTatliEYukselM2007Effects of carvedilol on plasma levels of pro-inflammatory cytokines in patients with ischemic and nonischemic dilated cardiomyopathyTex Heart Inst J3452917420794
- LefkowitzRJRajagopalKWhalenEJ2006New roles for beta-arrestins in cell signaling: not just for seven-transmembrane receptorsMol Cell246435217157248
- LeventhalMJRiegelBCarlsonB2005Negotiating compliance in heart failure: remaining issues and questionsEur J Cardiovasc Nurs429830715893959
- LindholmLHCarlbergBSamuelssonO2005Should beta blockers remain first choice in the treatment of primary hypertension? A meta-analysisLancet36615455316257341
- MaackCCremersBFleschM2000Different intrinsic activities of bucindolol, carvedilol and metoprolol in human failing myocardiumBr J Pharmacol1301131910882399
- MaggiEMarchesiECoviniD1996Protective effects of carvedilol, a vasodilating beta-adrenoceptor blocker, against in vivo low density lipoprotein oxidation in essential hypertensionJ Cardiovasc Pharmacol2753288847870
- ManleyS2003Haemoglobin A1c – a marker for complications of type 2 diabetes: the experience from the UK Prospective Diabetes Study (UKPDS)Clin Chem Lab Med4111829014598868
- McGillJBBakrisGLFonsecaV2007beta-Blocker use and diabetes symptom score: results from the GEMINI studyDiabetes Obes Metab94081717391169
- McMurrayJKoberLRobertsonM2005Antiarrhythmic effect of carvedilol after acute myocardial infarction: results of the Carvedilol Post-Infarct Survival Control in Left Ventricular Dysfunction (CAPRICORN) trialJ Am Coll Cardiol455253015708698
- MesserliFHGrossmanE2004beta-Blockers in hypertension: is carvedilol different?Am J Cardiol937B12B
- MetraMGiubbiniRNodariS2000Differential effects of beta-blockers in patients with heart failure: A prospective, randomized, double-blind comparison of the long-term effects of metoprolol versus carvedilolCirculation1025465110920067
- MorenoAJSantosDJPalmeiraCM1998Ischemic heart disease: the role of mitochondria – carvedilol prevents lipid peroxidation of mitochondrial membranesRev Port Cardiol17Suppl 2II63779835783
- NakamuraKKusanoKNakamuraY2002Carvedilol decreases elevated oxidative stress in human failing myocardiumCirculation10528677112070115
- NicholsAJSulpizioACAshtonDJ1989The interaction of the enantiomers of carvedilol with alpha 1- and beta 1-adrenoceptorsChirality1265702577144
- OthmanAATeneroDMBoyleDA2007Population pharmacokinetics of S(−)-carvedilol in healthy volunteers after administration of the immediate-release (IR) and the new controlled-release (CR) dosage forms of the racemateAaps J9E2081817614362
- OtterstadJEFordI2002The effect of carvedilol in patients with impaired left ventricular systolic function following an acute myocardial infarction. How do the treatment effects on total mortality and recurrent myocardial infarction in CAPRICORN compare with previous beta-blocker trials?Eur J Heart Fail4501612167391
- PackerMBristowMRCohnJN1996The effect of carvedilol on morbidity and mortality in patients with chronic heart failure. US Carvedilol Heart Failure Study GroupN Engl J Med3341349558614419
- PackerM1998Beta-adrenergic blockade in chronic heart failure: principles, progress, and practiceProg Cardiovasc Dis4139529715822
- PackerMFowlerMBRoeckerEB2002Effect of carvedilol on the morbidity of patients with severe chronic heart failure: results of the carvedilol prospective randomized cumulative survival (COPERNICUS) studyCirculation1062194912390947
- PackerMLukasMATeneroDM2006Pharmacokinetic profile of controlled-release carvedilol in patients with left ventricular dysfunction associated with chronic heart failure or after myocardial infarctionAm J Cardiol9839L45L
- PadiSSChopraK2002Salvage of cyclosporine A-induced oxidative stress and renal dysfunction by carvedilolNephron926859212372956
- PatelPATilleyDGRockmanHA2008Beta-Arrestin-Mediated Signaling in the HeartCirc J721725918838825
- PedersenMECockcroftJR2007The vasodilatory beta-blockersCurr Hypertens Rep92697717686376
- PodbregarMVogaG2002Effect of selective and nonselective beta-blockers on resting energy production rate and total body substrate utilization in chronic heart failureJ Card Fail83697812528088
- Poole-WilsonPASwedbergKClelandJG2003Comparison of carvedilol and metoprolol on clinical outcomes in patients with chronic heart failure in the Carvedilol Or Metoprolol European Trial (COMET): randomised controlled trialLancet36271312853193
- RaoRBGoldfrankLR1998Fixed-dose combination therapy: panacea or poison?Intensive Care Med2428359609404
- RasmussenJNGislasonGHRasmussenS2007Use of statins and beta-blockers after acute myocardial infarction according to income and educationJ Epidemiol Community Health611091718000133
- RosamondWFlegalKFurieK2008Heart disease and stroke statistics – 2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics SubcommitteeCirculation117e2514618086926
- StamlerJWentworthDNeatonJD1986Prevalence and prognostic significance of hypercholesterolemia in men with hypertension. Prospective data on the primary screenees of the Multiple Risk Factor Intervention TrialAm J Med803393946459
- StanleyWCRecchiaFALopaschukGD2005Myocardial substrate metabolism in the normal and failing heartPhysiol Rev85109312915987803
- SundbergSTiihonenKGordinA1987Vasodilatory effects of carvedilol and pindololJ Cardiovasc Pharmacol10Suppl 11S76802454373
- TatliEKurumT2005A controlled study of the effects of carvedilol on clinical events, left ventricular function and proinflammatory cytokines levels in patients with dilated cardiomyopathyCan J Cardiol21344815838561
- TeneroDMHendersonLSBaidooCA2006Pharmacokinetic properties of a new controlled-release formulation of carvedilolAm J Cardiol985L16L
- TodaN2003Vasodilating beta-adrenoceptor blockers as cardiovascular therapeuticsPharmacol Ther1002153414652111
- Torp-PedersenCPoole-WilsonPASwedbergK2005Effects of metoprolol and carvedilol on cause-specific mortality and morbidity in patients with chronic heart failure – COMETAm Heart J149370615846279
- Torp-PedersenCMetraMCharlesworthA2007Effects of metoprolol and carvedilol on pre-existing and new onset diabetes in patients with chronic heart failure: data from the Carvedilol Or Metoprolol European Trial (COMET)Heart939687317237130
- UdelsonJEPresslerSJSackner-BernsteinJ2007Compliance with Once Daily Controlled Release vs Twice Daily Immediate Release Carvedilol in Patients with Heart Failure: The CASPER TrialJ Card Fail13S135
- VittorioTJZoltyRKasperME2008Differential effects of carvedilol and metoprolol succinate on plasma norepinephrine release and peak exercise heart rate in subjects with chronic heart failureJ Cardiovasc Pharmacol Ther1351718287590
- WallhausTRTaylorMDeGradoTR2001Myocardial free fatty acid and glucose use after carvedilol treatment in patients with congestive heart failureCirculation1032441611369683
- WeberMABakrisGLTarkaEA2006aEfficacy of a once-daily formulation of carvedilol for the treatment of hypertensionJ Clin Hypertens (Greenwich)8840917170609
- WeberMASicaDATarkaEA2006bControlled-release carvedilol in the treatment of essential hypertensionAm J Cardiol9832L8L
- WislerJWDeWireSMWhalenEJ2007A unique mechanism of beta-blocker action: carvedilol stimulates beta-arrestin signalingProc Natl Acad Sci U S A104166576217925438
- World Health Organization2007Cardiovascular diseases Fact sheet no. 317 [online]. Accessed August 4, 2008. URL: http://www.who.int/mediacentre/factsheets/fs317/en/index.html.
- WrightJTJrBakrisGLBellDS2007Lowering blood pressure with beta-blockers in combination with other renin-angiotensin system blockers in patients with hypertension and type 2 diabetes: results from the GEMINI TrialJ Clin Hypertens (Greenwich)9842917978591
- YangSPHoLJChengSM2004Carvedilol differentially regulates cytokine production from activated human peripheral blood mononuclear cellsCardiovasc Drugs Ther18183815229385