Abstract
Although statins reduce cardiovascular morbidity and mortality further risk reduction is needed. In this respect low HDL-cholesterol concentrations and/or elevated triglyceride concentrations may be potential treatment targets. Niacin (nicotinic acid) is an effective drug which increases the plasma concentration of high-density lipoprotein (HDL)-cholesterol and decreases the concentration of low-density lipoprotein (LDL)-cholesterol, triglycerides and lipoprotein(a). Clinical studies indicate that niacin can significantly reduce the risk for cardiovascular events. However, niacin is not very commonly used because of significant side effects (especially flushing). Laropiprant is a potent selective antagonist of PGD2-receptor subtype-1 and can thus reduce niacin-induced flushing. Although the addition of laropiprant will reduce the frequency of flushing, it will not completely eliminate this side effect. Laropiprant does not change the effect of niacin on lipids or other side effects of niacin (ie, gastro-intestinal problems, glucose elevation). The combination of niacin with laropiprant may therefore enable use of niacin at higher doses and therefore exploit the full potential of the drug. Endpoint studies that will be published over the next few years will show whether this treatment modality also translates into clinical effect in patients treated with statins. Until publication of these studies niacin/laropiprant should be used only in high-risk patients not achieving lipid goals on statins.
Introduction
Atherosclerosis and its complications such as myocardial infarction, stroke and peripheral vascular disease remain important reasons of mortality and morbidity in industrialized and developing countries.Citation1 Therefore, it is of utmost importance to develop strategies for treating and preventing atherosclerosis. Atherosclerosis is seen as a dynamic process which is initiated and maintained by the interaction of risk factors and immunologic processes.Citation2 While many risk factors such as dyslipidemia, diabetes, smoking and hypertension are well established the mechanisms linking these risk factors with atherosclerosis are less well known.
Therefore, strategies to reduce risk factors are still our most powerful tools to prevent and treat atherosclerosis. Although many approaches have been proven successful, the treatment of dyslipidemia is probably the one which mediates the biggest benefit. Most of our current strategies with respect to lipids focus on low-density lipoprotein (LDL)-cholesterol reduction. This relates to several aspects. First, the mechanism by which elevated concentrations of LDL-particles result in atherosclerosis is relatively well understood. Especially after oxidation and/or modification LDL particles are central for inducing the immunologic processes underlying atherosclerosis. Second, the epidemiological relationship between elevated total cholesterol and atherosclerosis can be attributed to a large extent to elevated LDL-cholesterol. Finally, many studies have shown that lowering LDL-cholesterol by statins or other forms of therapy can reduce morbidity and mortality from atherosclerosis.Citation3,Citation4
The importance of treating abnormal lipid concentrations to prevent atherosclerotic events is also reflected in the guidelines of professional associations such as the American Heart Assocation, European Society of Cardiology and others.Citation5,Citation6 These guidelines have focused on LDL-cholesterol reduction although over the last decade it has been recognized that triglycerides, high-density lipoprotein (HDL)-cholesterol, and lipoprotein(a) are not only important as predictors of atherosclerotic events but are potential therapeutic targets.Citation7 This is very important since LDL-lowering strategies can obviously not prevent all atherosclerotic events. In fact, most studies report a relative risk reduction of 25% to 35%, which means that on average the majority of events cannot be prevented.Citation3,Citation4 Several strategies can be developed to improve this result. It is conceivable that more aggressive LDL-cholesterol reduction might further prevent atherosclerotic events. Another approach would be to address other lipidologic risk factors, such as triglycerides, HDL-cholesterol, lipoprotein(a), and probably also postprandial lipoproteins and specific subfractions of LDL and/or HDL.
Current treatment strategies and its limitations
The current treatment strategy strongly focuses on LDL-cholesterol reduction (). Depending on the absolute risk, an LDL-cholesterol of <100 mg/dL (optional <70 mg/dL) in patients with high risk (ie, >20% event rate/10 years) or an LDL-cholesterol <130 mg/dL (intermediate risk) or an LDL-cholesterol <160 mg/dL (low risk) is set as a treatment goal.Citation5 The primary drug treatment used to achieve these goals is usually a statin. However, several other drugs are available to modify lipid levels. These drugs differ in mode of action, effect on lipids and degree of evidence with respect to reducing cardiovascular morbidity and mortality. summarizes the various lipid-modifying drugs.
Table 1 Low-density lipoprotein (LDL) goals in different patient groupsCitation5
Table 2 Effect of lipid-modifying drugs
In patients with normal triglyceride and HDL-cholesterol levels but elevated LDL-cholesterol levels despite statin therapy several approaches are possible. These include increasing the dose of the statin, switching to a more potent statin, combining the statin with a cholesterol absorption inhibitor (ezetimibe) or combining a statin with a bile acid binding compound (for example colesevelam). For patients on a statin with abnormal triglyceride and/or HDL-cholesterol concentrations combination therapy of a statin with niacin may be a treatment option. The combination of statins with either a fibrate or omega-3 fatty acids may be alternatives. In patients with isolated hypertriglyceridemia primary fibrate or niacin therapy or treatment with omega-3 fatty acids may be considered.
However, it must be acknowledged that not all treatment strategies are covered by convincing end point data and some of the suggested combination therapies are associated with considerable side effects. This is particularly true for the combination of a statin with niacin or with a fibrate.
Niacin (nicotinic acid)
Niacin was the first lipid-lowering drug developed.Citation8 Despite clear lipid-lowering effects and the proof of clinical benefit in early prevention studies, niacin is not used very often in clinical practice. There are multiple reasons, the most important being the high rate of side effects and the stronger LDL-cholesterol reduction and the better documented effects of statins.Citation4,Citation9 Although extended-release forms of niacin (ERN) have somewhat less side effects in clinical practice, niacin is rarely used.
Effect of niacin on lipids
The effects of niacin on plasma lipids depend on the dose and the underlying dyslipoproteinemia. Clinically significant changes of lipid levels are usually seen at doses of 1 g/day or higher, but doses of 1.5 g/day or 2 g/day are necessary to achieve the full effect on lipids. Generally, niacin decreases total cholesterol, triglycerides, LDL-cholesterol and lipoprotein(a), while it increases HDL-cholesterol.Citation10,Citation11 The effects of niacin are summarized in .
Table 3 Effect of nicotinic acid on lipids, lipoprotein and apoproteins
Although niacin was initially used as monotherapy or in combination with fibrates or bile acid binding compounds, nowadays it is primarily indicated in combination with statins.Citation12,Citation13 It is therefore important to evaluate whether the changes described above also hold true in patients on statin therapy. In a recent study comparing 4 treatment arms in 293 patients with dyslipidemia it was shown that rosuvastatin (40 mg/day), simvastatin with ezetimibe (40 mg/10 mg per day), rosuvastatin with niacin (20 mg/2000 mg per day), and atorvastatin with niacin (40 mg/2000 mg per day) resulted in an identical reduction of LDL-cholesterol (−50% to −55%). Therapies without niacin resulted in an increase of HDL-cholesterol of approximately 5% to 10%, while the increase in combination therapy using niacin was 22% to 25%. In addition, combinations using niacin decreased triglycerides by 40% to 50%.Citation14 This indicates that the effect of niacin on plasma lipids is independent of the underlying baseline medication.
Generally it can be assumed that niacin at a dose of more than 1.5 g/day will decrease LDL-cholesterol, triglycerides and lipoprotein(a) by approximately 20%, while it will increase HDL-cholesterol also by approximately 20% (“rule of 20%”).Citation9,Citation15
Mechanism of action of niacin
The mechanism by which niacin affects plasma lipids is not completely understood.Citation16 Niacin binds to a specific G-protein receptor (GPR109A) which is expressed in adipose tissue and in epidermal cells.Citation17 The binding of niacin to the receptor results in a decreased lipolysis and thus a dose-dependent decreased release of free fatty acids into plasma. This decrease is followed by a rebound.Citation18 Despite this rebound the decreased flow of free fatty acids to the liver results in a decreased secretion of very low-density lipoprotein (VLDL) particles.Citation19 Hepatic VLDL secretion is determined by a number of regulators, of which free fatty acid concentration is probably the most important. The changes in LDL concentration and thus LDL-cholesterol are probably secondary phenomena. Since LDL are to a large extent the metabolic product of VLDL delipidation, it is evident that a decreased VLDL secretion rate will also reduce concentration of LDL particles. Niacin also affects the LDL subtype distribution, resulting in a shift from small dense LDL particles to more buoyant lipoproteins.Citation20 This results in less atherogenic LDL particles. For HDL-cholesterol, it is believed that the deceased concentration of VLDL particles will result in a decreased interaction with HDL particles leading to higher HDL-cholesterol concentrations. Whether and to what extent direct effects on HDL metabolism are important in inducing the raise in HDL-cholesterol is unknown. Furthermore, niacin also results in a shift within the HDL fraction; thus the HDL2: HDL3 ratio is increased. Again this is considered beneficial in relation to atherosclerosis. The mechanism underlying the reduction of lipoprotein(a) during therapy with niacin is unknown. However, it is an interesting observation that lipoprotein(a) concentrations can be decreased only by drugs that affect lipoprotein production, such as niacin or apo B antisense oligo-nucleotides such as mipomersen.Citation21 Drugs that primarily affect the catabolism of lipoproteins, such as statins, ezetimibe, or bile acid-binding compounds, usually have no effect on lipoprotein(a) concentration. Whether and to what extent niacin affects postprandial lipoprotein metabolism is unknown. However, it can be assumed that niacin will not only improve fasting lipids but also postprandial lipoprotein metabolism.
Clinical studies with niacin
A number of studies have shown that niacin can decrease surrogate parameters of atherosclerosis and clinical events ().Citation12,Citation22–Citation26 The HATS trial tested the hypothesis that lipid-modifying (simvastatin and niacin) and antioxidant therapy provide independent and additive benefits for patients with coronary heart disease and low HDL-cholesterol.Citation22 The study compared placebo vs simvastatin/niacin vs antioxidants vs simvastatin/niacin with antioxidants. The study showed no effect of antioxidants but proved that patients receiving simvastatin in combination with niacin had a significant reduction in cardiovascular events (60% relative risk reduction for simvastatin/niacin vs no simvastatin/niacin). However, as in previous studies it was not tested whether niacin provides an additional effect over statin monotherapy. The extent of risk reduction (60%) indicates, however, that the effect is more prominent than could be expected by simvastatin alone.
Table 4 Selected randomized controlled trials of nicotinic acidCitation12,Citation22–Citation26
The coronary drug project evaluated the effect of niacin as monotherapy in patients with established coronary heart disease.Citation11 After 6 years of treatment the clinical event rate was decreased by 27% in the niacin group. Furthermore, a secondary analysis (after 15 years) showed a decrease in total mortality of 11%.Citation23
Side effects of niacin
Despite these convincing data on lipids and clinical events, niacin is not very often used in clinical practice because of side effects. However, not all studies report high rates of discontinuation.Citation27–Citation29 Although the rate of flushing was decreased by using slow-release formulations it stills represents a hurdle for its clinical use. Furthermore, gastrointestinal symptoms such as diarrhea, nausea and reduced appetite as well as elevated glucose concentrations were reported.
In humans the flush following the oral intake of niacin is the result of a cutaneous vasodilatation which is mediated by prostaglandin D2 (PGD2).Citation30 In the skin niacin binds to the same receptor that mediates the lipid-modulating effects. In Langerhans cells of the epidermis this binding induces the formation of PDG2 which then binds to a specific receptor (prostaglandin-D2-receptor-1). This receptor mediates vasodilation and thus flushing.Citation31 In humans this receptor is present in the vessels of the skin, in the small intestine, in the brain and in the lung.Citation31,Citation32 Acetylsalicylic acid and other nonsteroidal anti-inflammatory drugs (NSAID)s have been found to have some efficacy suppressing niacin-induced flushing by preventing the production of prostaglandins.Citation33–Citation35 It is important to realize that the same receptor (GPR109A) is responsible for the effect on lipids and the flushing.Citation17 Strategies addressing the flushing therefore cannot act on the niacin receptor since this would also eliminate the effect on lipids.
Another important side effect of niacin therapy is the induction of elevated glucose concentrations. This was observed in earlier studies as well as in newer trials. The underlying mechanisms are not understood, but may be related to the primary effect on free fatty acid metabolism and thus reflect insulin resistance. In most patients the effect on glucose metabolism is negligible. In patients with metabolic syndrome and borderline disturbances of glucose metabolism such as impaired fasting glucose or glucose intolerance however this may be relevant. In a study in diabetic patients 16 weeks of therapy with 1500 mg/day niacin induced only minor changes of fasting glucose concentrations and HbA1c. However, during the course of the study oral anti-diabetic medication and insulin dose was adjusted.Citation36 Whether the effect of niacin on glucose metabolism is clinically relevant is questionable since in the Coronary Drug Project patients benefitted from such therapy irrespective of baseline glucose level.Citation37
Laropiprant
Since the flush induced by niacin is primarily mediated through the interaction of prostaglandin D2 with a specific receptor (prostaglandin-D2-receptor-1) a selective antagonist of this receptor was developed (MK-0524, laropiprant).Citation38,Citation39 Laropiprant was initially developed as a treatment for allergic rhinitis.Citation39,Citation40 It is eliminated primarily after glucuronidation through the liver.Citation41 A small part of laropiprant is metabolized through cytochromP450 3A4. Laropiprant is highly selective for the prostaglandin D2-receptor-1. It can be assumed that inhibition of this receptor does not reduce the production of prostaglandins, but inhibits the vasodilatation following the formation of PGD2. Although laropiprant is a potent inhibitor of prostaglandin D2-receptor-1, it does not eliminate flushing in all patients. Higher doses of laropiprant or concomitant use of aspirin or NSAIDs cannot reduce this residual flushing.Citation42,Citation43 Probably other mediators such as PGE2 and serotonin, as well as their pathways, such as the beta-arrestin1/MAP kinase signaling pathway, are involved in this residual flushing.Citation17,Citation44
Laropiprant can also bind to the thromboxan-A2-receptor, which plays an important role thrombocyte function.Citation45 However, in doses currently used to prevent flushing associated with niacin no clinical effects on bleeding or thrombocyte function were observed. The current, albeit short-term, studies indicate that laropiprant does not affect the lipid-modifying properties of niacin and has little side-effects by its own. However, long-term observations are necessary to truly confirm long-term safety. It should also be noted that preliminary data indicate that other forms of flushing cannot be prevented by laropiprant.
Niacin/laropiprant
Since niacin is associated with flushing and since laropiprant can significantly reduce this flushing, it seems obvious to combine these drugs.Citation46 Recently it was shown that the rate of moderate/severe flushing can be reduced from 50% to 24% by adding laropiprant to niacin.Citation47 The same study showed that besides severity also frequency of flushing was reduced. Furthermore, it was recently shown in abstract form in a study involving more than 4700 patients that the addition of laropiprant to ERN reduced the rate of discontinuation due to flushing from 16.6% to 7.2% and the overall discontinuation rate from 31.5% to 25.3%.Citation48 ERN/laropiprant patients use considerably less aspirin/NSAID to reduce flushing compared to ERN patients (11% vs 22%).Citation46
The addition of laropiprant does not change the effect of niacin on lipids.Citation49,Citation50 In a study evaluating more than 1300 patients, niacin with or without laropiprant decreased LDL-cholesterol by 18.4%, triglycerides by 25.8% and increased HDL-cholesterol by 20%.Citation49 For none of the lipid parameters the effect was altered by the addition of laropiprant.
In studies evaluating the combination of niacin with laropiprant on flushing it was shown that the rate of flushing was significantly decreased compared to patients on niacin without laropiprant.Citation46–Citation49,Citation51 In the group using additional laropiprant the rate of flushing was decreased to placebo level after approximately 3 months while it remained elevated in patients using niacin without laropiprant.
In a recent post hoc analysis it was also shown that niacin alone or in combination with laropiprant was associated with significant placebo-adjusted reductions from baseline in blood pressure in hypertensive or normotensive subjects with dyslipidemia.Citation52 This may be important since it would indicate that niacin not only addresses dyslipidemia as an important cardiovascular risk factor, but has a more general beneficial effect on risk factors. Acute administration of niacin may lower blood pressure because of acute vasodilatory effects. From a chronic perspective, larger studies, such as the coronary drug project, suggest that niacin may lower blood pressure when administered over a longer period of time. Post hoc analyses of some of the more recent trials support a chronic, dose-dependent, blood pressure-lowering effect of niacin. Since, however, laropiprant does not attenuate niacin’s blood pressure-lowering effects, it is unlikely that the chronic lowering of blood pressure is due to dilation of skin vessels through activation of the prostaglandin receptor.Citation53
Clinical use of niacin/laropiprant
This combination may be used in patients who are considered candidates for niacin therapy. The addition of laropiprant does not alter the lipid effects but may allow using the doses necessary to achieve the full effect of niacin.
Primary candidates are patients with high risk (ie, >20% over 10 years) who for multiple reasons do not reach lipid goals. Thus, this combination should be considered in patients who despite statin therapy have elevated LDL-cholesterol in combination with elevated triglycerides and/or low HDL-cholesterol. Many of the potential candidates will have suboptimal LDL-cholesterol, triglycerides and HDL-cholesterol despite established vascular disease. Furthermore, many potential patients may be diabetic or suffer from metabolic syndrome. Niacin/laropiprant may also be a treatment option in patients who are at goal with LDL-cholesterol but have abnormal HDL-cholesterol and triglyceride concentrations ().
Figure 1 The figure describes a possible algorithm for treating patients with different forms of dyslipidemia.
Abbreviations: ω-3-FA, omega-3 fatty acids; ERN/LRPT, extended release niacin/laropiprant.
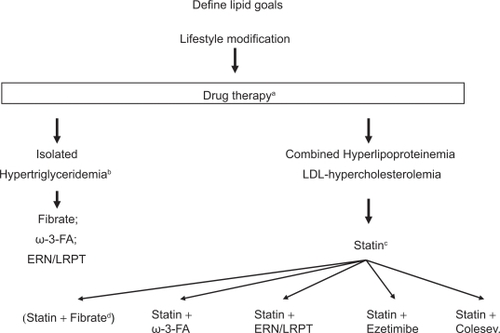
The role of nicotinic acid/laropiprant is probably less clear in patients with isolated severe hypertriglyceridemia or patients with isolated LDL hypercholesterolemia. In those patients other treatment modalities are possible. Thus, in patients with isolated severe hypertriglyceridemia, lifestyle changes, which are of utmost importance, may be combined with fibrates, niacin/laropiprant, omega-3 fatty acids or rarely statins. In selected patients combinations of these drugs may be necessary. Similarly in patients with isolated LDL hypercholesterolemia despite statin therapy a number of different approaches is possible. Niacin/laropiprant, ezetimibe or a bile acid binding compound can be added, since all provide further LDL-cholesterol reduction by approximately 20% (which may vary considerably in individual patients). While niacin and bile acid-binding substances have been proven to reduce CHD events, no such data are available for ezetimibe. On the other hand, ezetimibe is associated with fewer side effects compared to niacin and bile acid-binding substances.
Whether or not niacin/laropiprant is a treatment option for patients with elevated lipoprotein(a) remains to be determined. Although niacin may decrease lipoprotein(a) by up to 30%, it is unclear whether such a modification mediates a clinical benefit. However, in patients with elevated lipoprotein(a) and recurrent cardiovascular events despite optimal treatment of all other risk factors niacin/laropiprant may be a treatment option.
Although niacin has been shown to mediate beneficial effects on cardiovascular outcome if given in monotherapy or in combination with other lipid-altering drugs, including statins, no published study has used high-dose statin mono-therapy as a comparator. Thus, strictly speaking the additional benefit of niacin has not been shown in patients on statin therapy. Therefore its use should be restricted to patients at high-risk until further data are available.
Several large outcome studies will evaluate whether niacin therapy can reduce cardiovascular events. These studies will be published in 2011 or 2012. The hypothesis of AIM-HIGH is that combination antidyslipidemic therapy (niacin with simvastatin) will be superior to statin monotherapy (simvastatin) when used as secondary prevention in reducing long-term clinical events in patients with documented vascular disease and atherogenic dyslipidemia. About 3300 patients will be randomized to receive simvastatin monotherapy or simvastatin with niacin.
In another study (HPS2-THRIVE) it will be evaluated whether the combination of niacin and laropiprant prevents myocardial infarctions, stroke or revascularization procedures in patients with existing vascular disease. Approximately 25,000 patients will be evaluated, including more than 7000 diabetic patients.
Disclosures
KGP has received travel rants, speaking fees or research support form AstraZeneca, Bayer, Genzyme, MSD, Novartis, Sanofi-Aventis, and Schering-Plough.
References
- StegPGBhattDLWilsonPWOne-year cardiovascular event rates in outpatients with atherothrombosisJAMA20072971197120617374814
- HanssonGKInflammation, atherosclerosis and coronary artery diseaseN Engl J Med20053521685169515843671
- BaigentCKeechAKearneyPMCholesterol Treatment Trialists’ (CTT) CollaboratorsEfficacy and safety of cholesterol-lowering treatment:prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statinsLancet20053661267127816214597
- Cholesterol Treatment Trialists’ (CTT) CollaboratorsKearneyPMBlackwellLCollinsREfficacy of cholesterol-lowering therapy in 18,686 people with diabetes in 14 randomised trials of statins:a meta-analysisLancet200837111712518191683
- GrundySMCleemanJIMerzCNImplications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelinesCirculation200411022723915249516
- GrahamIAtarDBorch-JohnsenKEuropean guidelines on cardiovascular disease prevention in clinical practice: executive summary: Fourth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical PracticeEur Heart J2007282375241417726041
- American Diabetes AssociationStandards of Medical Care in Diabetes – 2009Diab Care200932S1S13S61
- AltschulRHofferAStephenJDInfluence of nicotinic acid on serum cholesterol in manArch Biochem19555455855914350806
- VogtAKassnerUHostalekUEvaluations of safety and tolerability of prolonged-release nicotinic acid in a usual care setting: the NAUTILUS StudyCurr Med Res Opin20062241742516466614
- ShepherdJPackardDJPatschJREffects of nicotinic acid therapy on plasma high density lipoprotein subfraction distribution and composition and on apolipoptotein A metabolismJ Clin Invest197963858867221531
- KnoppRHDrug treatment of lipid disordersN Engl J Med199934149851110441607
- Coronary Drug Project Research GroupClofibrate and niacin in coronary heart diseaseJAMA19752313601088963
- CarlsonLARosenhamerGReduction of mortality in the Stockholm Ischaemic Heart Disease Secondary Prevention Study by combined treatment with clofibrate and nicotinic acidActa Med Scand19882234053287837
- McKenneyJMJonesPHBaysHEComparative effects on lipid levels of combination therapy with a statin and extended-release niacin or ezetimibe versus a statin alone (the COMPELL study)Atherosclerosis200719243243717239888
- CapuzziDMGuytonJRMorganJMEfficacy and safety of an extended-release niacin (Niaspan):a long-term studyAm J Cardiol19988274U81U
- KamannaVSGanjiSHKashyapMLNiacin:an old drug rejuvenatedCurr Atheroscler Rep200911455119080727
- BenyoZGilleAKeroJGPR109A (PUMA-G/HM74A) mediates nicotinic acid-induced flushingJ Clin Invest20051153634264016322797
- CarlsonLAOröLThe effect of nicotinic acid on the plasma free fatty acidsActa Med Scand196217264164514018702
- CarlsonLANicotinic acid: the broad spectrum lipid drug. A 50th anniversary reviewJ Intern Med20052589411416018787
- VanJTPanJWastyTComparison of extended-release niacin and atorvastatin monotherapies and combination treatment of the atherogenic lipid profile in diabetes mellitusAm J Cardiol200289130612031735
- DavidsonMHNovel nonstatin strategies to lower low-density lipoprotein cholesterolCurr Atheroscler Rep200911677019080731
- BrownBGZhaoXQChaitASimvastatin and niacin, antioxidant vitamins, or the combination for the prevention of coronary diseaseN Engl J Med20013451583159211757504
- CannerPLBergeKHWengerNKFifteen year mortality in coronary drug project patients: long-term benefit with niacinJ Am Coll Cardiol1986812453782631
- BlankenhornDHNessimSAJohnsonRLBeneficial effects of combined colestipol-niacin therapy on coronary atherosclerosis and coronary venous bypass graftsJAMA1987257323332403295315
- TaylorAJSullenbergerLELeeHJArterial Biology for the Investigation of the Treatment Effects of Reducing Cholesterol (ARBITER) 2: a double-blind, placebo-controlled study of extended-release niacin on atherosclerosis progression in secondary prevention patients treated with statinsCirculation20041103512351715537681
- TaylorAJLeeHJSullenbergerLEThe effect of 24 months of combination statin and extended-release niacin on carotid intima-media thickness: ARBITER 3Curr Med Res Opin2006112243225017076985
- SinghIMShishehborMHAnsellBJHigh-density lipoprotein as a therapeutic target:a systematic reviewJAMA200729878679817699012
- ZhaoXQMorseJSDowdyAASafety and tolerability of simvastatin plus niacin in patients with coronary artery disease and low high-density lipoprotein cholesterol (The HDL Atherosclerosis Treatment Study)Am J Cardiol20049330731214759379
- Rubenfire M Safety and compliance with once-daily niacin extended-release/lovastatin as initial therapy in the Impact of Medical Subspeciality on Patient Compliance to Treatment (IMPACT) StudyAm J Cardiol20049430631115276093
- MorrowJDAwadJAOatesJAIdentification of skin as a major site of prostaglandin D2 release following oral administration of niacin in humansJ Invest Dermatol1992988128151373750
- IshidaHMasuhioYFukushimaAIdentification and characterization of novel isoforms of human DP-1:DP-1 (alpha) regulates the transcriptional activity of E2F1 as well as cell cycle progression in a dominant-negative mannerJ Biol Chem2005280246422464815863509
- ChengKWuTJWuKKAntagonism of the prostaglandin D2 receptor 1 suppresses nicotinic acid-induced vasodilation in mice and humansProc Natl Acad Sci U S A20061036682668716617107
- JungnickelPWMaloleyPAVander TuinELPeddicordTECampbellJREffect of two aspirin pretreatment regimens on niacininduced cutaneous reactionsJ Gen Intern Med1997125915969346454
- WilkinJKWilkinOKappRDonachieRChernoskyMEBucknerJAspirin blocks nicotinic acid-induced flushingClin Pharmacol Ther1982314784827060328
- DunnRTForMARindoneJPKwiecinskiFALow-dose aspirin and ibuprofen reduce the cutaneous reactions following niacin administrationAm J Ther1995247848011850694
- GrundySMVegaGLMcGovernMEEfficacy, safety, and tolerability of once-daily niacin for the treatment of dyslipidemia associated with type 2 diabetes: results of the assessment of diabetes control and evaluation of the efficacy of niaspan trialArch Intern Med2002162156812123399
- CannerPLFurbergCDTerrinMLMcGovernMEBenefits of niacin by glycemic status in patients with healed myocardial infarction (from the Coronary Drug Project)Am J Cardiol20059525425715642562
- DeanBJChangSSilva ElipeMVMetabolism of MK-0524, a prostaglandin D2 receptor 1 antagonist, in microsomes and hepatocytes from preclinical species and humansDrug Metab Dispos20073528329217132765
- SturinoCFO’NeillGLachanceNDiscovery of a potent and selective PGD2 receptor antagonist [(3R)-4-(4-chlorobenzyl)-7-fluoro-5-(methylsulfonyl)-1,2,3,4-tetrahydrocyclopentaindol-3-yl]-acetic acid (MK-0524)J Med Chem20075079480617300164
- Van HeckenADepréMDe LepeleireIThe effect of MK-0524, a prostaglandin D(2) receptor antagonist, on prostaglandin D (2)-induced nasal airway obstruction in healthy volunteersEur J Clin Pharmacol20076313514117200838
- BindhuKMariaMScottBAbsorption, metabolism, and excretion of [14C]MK-0524, a prostaglandin D2 receptor antagonist, in humansDrug Metab Dispos200735119617431030
- LaiEWenningLACrumleyTMPharmacokinetics, pharmacodynamics, and safety of a prostaglandin D2 receptor antagonistClin Pharmacol Ther20088384084717882161
- DishyVLiuFEbelDLAtieeGJEffects of aspirin when added to the prostaglandin D2 receptor antagonist laropiprant on niacin-induced flushing symptomsJ Clin Pharmacol20094941642219246721
- PapaliodisDBoucherWKempurajDNiacin-induced “flush” involves release of prostaglandin D2 from mast cells and serotonin from platelets: evidence from human cells in vitro and an animal modelJ Pharm Exp Ther2008327665672
- FeltsASMolecule of the month. TREDAPTIVE (nicotinic acid/laropiprant): a new lipid-modifying therapy for the treatment of LDL-C, HDL-C and triglyceridesCurr Top Med Chem200814131018928015
- MaccubbinDKorenMJDavidsonMFlushing profile of extended-release niacin/laropiprant versus gradually titrated niacin extended-release in patients with dyslipidemia with and without ischemic cardiovascular diseaseAm J Cardiol2009104748119576324
- KushDHuDYYePFlushing profile of extended-release niacin/laropiprant at initiation of therapy in Asian lipid clinic patientsCardiology200911419219819602880
- McKenneyJBaysHKorenMSafety profile of extended-release niacin/laropiprant in patients with dyslipidemia. Abstracts 77th Congress of the European Atherosclerosis SocietyAtherosclerosis Suppl200891194195
- MaccubbinDBaysHEOlssonAgLipid-modifying efficacy and tolerability of extended-release niacin/laropiprant in patients with primary hypercholesterolaemia or mixed dyslipidaemiaInt J Clin Pract2008621959197019166443
- GleimGBallantyneCMLiuNEfficacy and safety profile of co-administered ER niacin/laropiprant and simvastatin in dyslipidaemiaBr J Cardiol2009169097
- PaoliniJFMitchelYBReyesREffects of laropiprant on nicotinic acid-induced flushing in patients with dyslipidemiaAm J Cardiol200810162563018308010
- BaysHEMaccubbinDMeehanAGBlood pressure-lowering effects of extended-release niacin alone and extended-release niacin/laropiprant combination: a post hoc analysis of a 24-week, placebo-controlled trial in dyslipidemic patientsClin Ther20093111512219243712
- BaysHERaderDJDoes nicotinic acid (niacin) lower blood pressureInt J Clin Pract20096315115919054161