
Abstract
Aim: To evaluate the genetic factors influencing tuberculosis (TB) clinical outcomes in HIV-infected Black African patients. Materials & methods: We systematically searched and identified eligible publications from >550 databases indexed through February 2021. Results: Eighteen studies were included in the qualitative synthesis. Only two cohorts from one study were included in quantitative synthesis of which the low expression MIF−794 CATT5,6 (5/5 + 5/6 + 6/6) genotypes were not associated with TB infectivity in HIV-infected patients (OR: 1.31, 95% CI: 0.46–3.79). Other TB clinical outcomes observed in HIV/TB co-infected patients included: drug-induced liver injury, peripheral neuropathy, mortality, lung function and TB cure. Conclusion: This review finds inconclusive evidence that genetic factors are associated with TB clinical outcomes among HIV-infected patients in sub-Saharan Africa.
Tuberculosis (TB) remains a global public health concern, with an estimated 10 million people developing active TB disease in 2019, and the WHO Africa region accounting for 25% of these estimates [Citation1]. In the same year, there were approximately 1.2 million and 208,000 global TB deaths in human immunodeficiency virus (HIV)-negative and HIV-positive people respectively [Citation1]. On the other hand, in 2017, close to 37 million people were estimated to be living with HIV, and sub-Saharan Africa had the highest prevalence [Citation2]. Despite the remarkable scale-up of antiretroviral therapy (ART), HIV/acquired immunodeficiency syndrome (AIDS)-related mortality remains unacceptable (0.95 million deaths in 2017 alone [Citation2]), with TB being the most frequent opportunistic infection and leading cause of death among HIV-infected patients [Citation3,Citation4]. To further reduce HIV/AIDS-related mortality and improve health-related quality of life, it is therefore important to identify the risk factors for developing active TB in HIV infected patients as well as those factors that contribute to poor prognosis in HIV/TB co-infected patients.
It is now recognized that host genetics, in addition to pathogen, environmental, and socioeconomic factors, play a key role in regulating both the establishment and progression of Mycobacterium tuberculosis infection [Citation5]. Previous systematic reviews and/or meta-analyses [Citation6–9] have explored several genetic variants of importance with regard to TB-related outcomes. However, these studies were neither focused on HIV-infected patients nor were they conducted in Black Africans, and as such may not be generalizable to this patient population. Consequently, there is little information on how genetic factors influence TB-related outcomes in HIV-infected Black African patients. We conducted this systematic review and meta-analysis to summarize the role of genetic factors in influencing TB-related clinical outcomes in HIV-infected Black African patients.
Methods
A predefined protocol (PROSPERO: CRD42021237551 [Citation10]) was followed, and reporting adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [Citation11] (Supplementary Table 1).
Search strategy & selection criteria
A systematic literature review search using the University of Liverpool’s DISCOVER platform was conducted on 16 February 2021. This platform links, through EBSCOhost, to sources from more than 550 databases (as of 16 February 2021) including MEDLINE, the Web of Science and the Cochrane Central Register of Controlled Trials. Studies were identified using medical subject headings (MeSH terms) and the following search strategy: ([Africa* OR Black*] AND [Tuberculosis* OR TB*] AND [HIV* OR (human AND immunodeficiency AND virus*) OR AIDS* OR (Acquired AND Immunodeficiency AND Syndrome*)] AND [Gene* OR Geno* OR Haplotyp* OR Pharmacogene* OR Pharmacogeno* OR Variant* OR Allel* OR SNP* OR Polymorphism*]). Lists of references from the identified studies and previous systematic reviews were then screened to identify additional eligible articles. For ongoing and recently completed trials, trial registries including ClinicalTrials.gov and the International Clinical Trials Registry Platform were searched. Lastly, experts in the HIV/TB field were contacted to identify any further eligible studies. Non-English studies were excluded, unless translated text was available. We did not restrict studies based on the year of publication or the publication status.
Both observational (e.g., retrospective or prospective cohort and case-control studies) and interventional (e.g., randomized controlled trials) studies, in which at least 5% of recruited HIV-infected patients were Black Africans, and which investigated the effect of at least one genetic factor on TB-related clinical outcomes were included. We did not restrict studies based on any other patient characteristics such as age or other comorbidities. The prospectively chosen clinical outcomes included, but were not to be restricted to, TB infectivity (for HIV-infected patients); and, cure, treatment completion, failure, relapse, acid-fast bacillus (AFB) smear conversion, sputum culture conversion, chest radiograph score changes from baseline, drug adverse effects, and all-cause mortality (for TB/HIV co-infected patients).
Data extraction & quality assessment
For title/abstract screening of identified records, a random selection of 10% of the papers were initially chosen to be screened by the first reviewer (IGA). These were then independently screened by two other reviewers (DK or SW) to check for consistency. The first reviewer was consistent with regard to following eligibility criteria and therefore continued title/abstract screening for the rest of the records. For full-text screening of potentially eligible studies, all studies were independently screened by two reviewers (IGA and DK/SW), with any disagreements resolved through discussion or adjudication of a third reviewer.
A data extraction form was developed and piloted in a subset of ten randomly selected studies included in the review (the sample function in R version 3.5.1 [Citation12] was used to pick the random studies). This was then used to extract relevant information related to study design, patient characteristics, study quality and TB-related clinical outcomes for the rest of the included studies. Data from all eligible studies were extracted and summarized by two independent reviewers (IGA and DK/SW) with any disagreements resolved through discussion or adjudication of a third reviewer. For quality assessment of included studies, two reviewers (IGA and DK/SW) used the criteria in the quality assessment tool by Jorgensen and Williamson [Citation13] which has previously been developed to aid the assessment of the methodological quality of pharmacogenetic studies included in systematic reviews. Again, disagreements were resolved through discussion or adjudication of a third reviewer.
Data synthesis & analysis
Data synthesis
Meta-analyses were conducted for each genetic variant and outcome combination where two or more studies/cohorts were present. To avoid assuming a particular genetic model when three genotype groups were reported (wild-type homozygotes, heterozygotes and variant-type homozygotes), we planned to employ a genetic model-free approach [Citation14] as previously detailed [Citation15]. However only two genotype groups were reported for the study we included in the meta-analysis and we therefore performed standard meta-analysis using R version 3.5.1 [Citation12] (R meta package [Citation16]). Usually meta-analyses are conducted by results from separate studies, but two cohorts reported by the same study can still be quantitatively synthesized as previously conducted [Citation17,Citation18]. Pooled odds ratios (ORS) with 95% CIs was generated and a Forest plot was prepared for the genetic variant-outcome combination analyzed. The other studies that could not be pooled for reasons such as reporting unique genetic variants and clinical outcomes, were only included in the qualitative synthesis (described narratively and in structured tables).
Heterogeneity measures
Heterogeneity in the study results was evaluated through visual assessment of the Forest plots and consideration of the I2 statistic [Citation19]. Arbitrary-defined heterogeneity categories included: I2 <30%, low; I2 30–70%, moderate; and I2 >70%, high. Potential sources of heterogeneity were not explored because we could not conduct subgroup analyses (see below). A random effects model was used because of the high heterogeneity in the two included cohorts.
Publication bias & selective reporting
Publication bias was not explored because there were less than ten studies for each of the genetic variant clinical outcome exposure combinations while selective reporting was evaluated as part of the methodological quality assessment.
Sensitivity & subgroup analyses
We did not conduct any sensitivity/subgroup analyses because only two patient cohorts were pooled in the meta-analysis that we conducted.
Confidence in cumulative evidence
Two independent reviewers (IGA and DK/SW) used the Venice interim criteria [Citation20] to assess the strength of the body of evidence and the quality/strength of the recommendations. Any disagreements were resolved through discussion or adjudication of a third reviewer.
Results
Study selection, characteristics & quality assessment
Of 5929 Endnote deduplicated records, 18 studies were included in the qualitative synthesis while only one study that reported two distinct cohorts comprising of 192 and 164 adult HIV-infected South African patients was included in the quantitative synthesis (). Details of individual study characteristics are provided in . Half (50%) of the studies (n = 9) reported a prospective cohort design while others reported case-control (n = 4, 22%) and cross-sectional (n = 5, 28%) designs. Fifteen (83%) studies employed a candidate-gene approach, with the rest (n = 3, 17%) being genome-wide association studies. The median number of Black African HIV-infected patients in the included studies was 288 (range: 94–1067). The key reported genetic factors and outcomes investigated by each of the included studies are also summarized in .
TB: Tuberculosis.
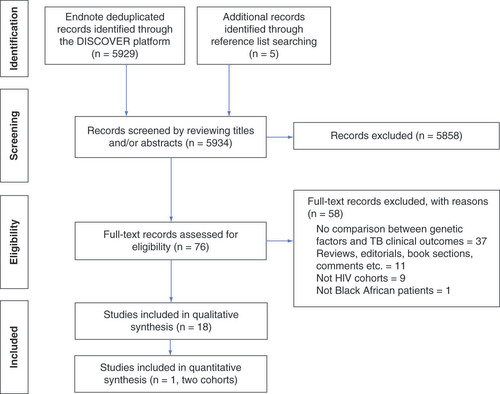
Table 1. Characteristics of included studies.
We qualitatively assessed the methodological rigor of included studies as previously recommended [Citation13] (details in Supplementary Table 2). All 18 studies included literature reviews to support the choice of investigated genetic factors, although none of these were structured. Although these studies investigated multiple genetic variants, only four (22%) reported adjusting for multiple testing. Only two (11%) studies justified their sample sizes through sample size calculations. Based on sample size calculations for a hypothetical pharmacogenetic study [Citation13], most included studies were likely underpowered. All studies reported genotyping procedures, although only 9 (50%) and 2 (11%) respectively reported genotype quality control procedures or whether genotyping staff were blinded to outcome status. All studies summarized the extent of missing data, although for those with missing data (n = 16, 89%), none described checks for missingness at random. Four (22%) and 10 (56%) studies respectively undertook cryptic population stratification and Hardy-Weinberg equilibrium (HWE) tests. HWE results for selected variants (together with minor allele frequencies) are reported in Supplementary Table 3. Only 7 (38%) studies reported details on the assumed modes of inheritance while all studies defined and justified investigated outcomes (definitions shown in ). We did not explore compliance to treatment as enrolling patients on specific anti-HIV/TB drugs was not part of our study inclusion criteria. Last, and despite several issues of concern in the methodological rigor of included studies, there were no outliers in terms of being of particularly low or high quality overall.
TB infectivity
Eleven studies [Citation21,Citation22,Citation26,Citation28,Citation31–35,Citation42,Citation47] recruited HIV-infected patients and reported count data and/or odds ratios (OR) for the association between selected genetic variants and TB infectivity/having active TB disease ( & Supplementary Table 3). Only four studies reported statistically significant associations. The first, Sobota and colleagues [Citation34], conducted a genome-wide association study in 581 Tanzanian and Ugandan patients and reported that only one SNP rs4921437 passed genome-wide significance (adjusted odds of having active TB = 0.374, 95% CI: 0.266–0.528, p = 2.11E-08). A later study [Citation35] by the same group (469 Tanzanians and Ugandans) reported that the SNP rs877356 was significantly associated with having a positive tuberculin skin test (adjusted OR = 0.267, 95% CI: 0.170–0.422, p = 1.22E-08). In a candidate-gene association study, Reid et al. [Citation42] reported that the low expression MIF−794 CATT5,6 (5/5 + 5/6 + 6/6) genotypes were significantly higher in South African Durban patients (n = 196) with active TB when compared with controls (OR = 2.23, 95% CI 1.08–4.71, p = 0.019), although this was not seen in a cohort comprising 165 patients from Tugela Ferry and Greytown (OR = 0.76, 95% CI: 0.36–1.59, p = 0.46). When these two cohorts were pooled, statistical significance was lost (OR = 1.31, 95% CI: 0.46–3.79, p = 0.61, ). Last, Seedat et al. [Citation47] reported several human leukocyte antigen alleles that were statistically significantly associated with TB infection/immune conversion and TB disease in both univariate and multivariate analyses ().
X represents any allele, so 7/X is equivalent to ‘7-containing’.
![Figure 2. Forest plot for association between MIF CATT-794 genotypes and active-tuberculosis disease in the Reid [Citation42] cohorts. X represents any allele, so 7/X is equivalent to ‘7-containing’.](/cms/asset/89307afa-908b-43db-bbe8-c9e935932a8b/ipgs_a_12349033_f0002.jpg)
TB clinical outcomes
Of the seven studies [Citation24,Citation29,Citation36,Citation38,Citation40,Citation43,Citation46] that recruited HIV/TB co-infected and reported associations between selected genetic variants and TB treatment-related clinical outcomes, four studies reported on hepatic related outcomes as a TB clinical outcome in which SLCO1B1 (032 T >C, rs4149032 [OR = 2.306, 95% CI 1.075–4.948, p = 0.029]) and PXR (63396 C >T, rs2472677 [p = 0.021]) were observed to be associated with elevated ALT as candidate gene-studies [Citation40]. Notably, one GWAS study observed rs4842407 to be associated with drug induced liver injury (OR = 5.4 [95% CI 2.8–10.3], p = 5.3E-07) as a top hit despite the fact that it failed to achieve GWAS p-value significance threshold [Citation36].
In studies (n = 2) that looked at peripheral neuropathy as a clinical end point [Citation29,Citation40], only one observed PXR (63396 C >T, rs2472677) to be associated with peripheral neuropathy (OR = 2.944, 95% CI 1.164–7.443, p = 0.018) [Citation40].
Two studies investigated mortality [Citation38,Citation40]; one observed that the PXR gene SNP (rs2472677) was associated with a higher mortality (OR = 4.575, 95% CI 1.388–15.083, p = 0.007) while in the other the statistically significant SNP was in the NLRP3 gene (rs10754558, OR = 4.1, 95% CI 1.04–16.5, p = 0.043). The only study that considered lung function as a clinical end point observed NLRC4 (rs385076) to be associated with improved lung function (p = 0.034) [Citation46]. Lastly, Calgano et al. [Citation40] investigated TB cure (PXRrs2472677) but no statistical significance was observed (p = 0.342). Detailed descriptions of the association of host genetic factors and TB clinical outcomes are summarized in & Supplementary Table 3.
Discussion
We have summarized the role of genetic factors in influencing TB-related clinical outcomes in HIV-infected Black African patients. The most explored clinical outcome was TB infectivity and/or having active TB disease, reported by 11 studies. However, we were only able to pool two cohorts from one study because all studies explored different genetic variants. Although most studies did not find significant associations between the explored genetic variants and TB infectivity/having active TB disease, it is possible that these studies were underpowered [Citation13]. Some studies including two genome-wide association studies reported significant findings. However, these results should be cautiously interpreted since they are yet to be replicated. The only pooled estimate that we report (migration inhibitory factor genotypes not being significantly associated with active TB) may also be unreliable due to the few patients (n = 356) included.
Five other clinical outcomes (drug-induced liver injury, peripheral neuropathy, mortality, cure and lung function) were investigated but no meta-analyses could be conducted and the results should be cautiously interpreted. Indeed, and mainly driven by the lack of association/independent replication [Citation20], all presented evidence should be considered weak. This resonates with the Pharmacogenomics Knowledge Base (PharmGKB) clinical annotations for tuberculosis (27 out of 29 annotations at level 3/4 – no clear evidence of genetic variant-drug combination associations) [Citation48,Citation49]. Including few eligible studies in this article is also consistent with previous reports. For example, the number of studies conducted in sub-Saharan Africa were only 0 (0% of 15) [Citation50], 0 (0% of 12) [Citation51], 3 (16% of 19) [Citation52], 4 (33% of 12) [Citation8], and 5 (16% of 32) [Citation6] in previous TB-related genetic reviews (these reviews focused on specific variants).
Despite not conducting structured reviews, all studies provided literature to support the choice of investigated genetic factors. For example, genes including β-Defensins, CR1, CXCR2, FCGR, HLA, ILs, MIF, SLC11A1, TNF and VDR were investigated for TB infectivity because they are involved in host defense mechanisms [Citation21,Citation22,Citation26,Citation28,Citation31–33,Citation42]. On the other hand, genes involved in the absorption, distribution, metabolism and excretion of anti-TB drugs (such as ABCB1, CYP3A5, CYP2B6, NAT2, PXR, SLCO1B1 and UGT2B7) were investigated for efficacy (cure or mortality) and toxicity (drug-induced liver injury and peripheral neuropathy) [Citation24,Citation29,Citation40,Citation43].
Whereas we focused on HIV-positive patients, other reviews also included HIV-negative patients with a plan to adjust for HIV infection status [Citation6]. Our exclusion of HIV-negative patients implies we included fewer studies and possibly missed out on important genetic variants. However, an approach that includes several studies and adjusts for co-variates such as HIV status (meta-regression) would require very many studies to be included for adequate power (ten studies per co variate parameter [Citation53]). It is also possible that there are important associations in HIV-negative patients which our study did not explore. However, our decision to restrict the review to only HIV-positive patients is justified by the fact that these patients are highly vulnerable to TB [Citation3,Citation4] (as compared with those not infected with HIV). Another key limitation of this review is that we did not contact study authors to include the genetic factors whose results were not available in the primary reports. This can contribute to biased pooled estimates if the excluded results are not statistically significant, which however should have little impact on this review since only one genetic variant was pooled by way of meta-analysis. In the future, and as more studies get published, authors will be contacted for any non-published estimates to ensure that any pooled estimates are reliable.
Conclusion
In conclusion, this review finds limited evidence supporting the role of genetic factors in influencing TB-related clinical outcomes in HIV-infected Black African patients. This is mainly attributed to the few TB-related genetic studies which is worrisome given that sub-Saharan Africa, and in particular HIV-infected patients, bear the greatest burden of TB disease [Citation54,Citation55].
Future perspective
To improve health-related quality of life in HIV and HIV/TB-co-infected patients, it is important that high quality genetic studies be urgently conducted to identify the clinically-actionable genetic factors that influence TB-related outcomes. More collaborations such as the Collaborative African Genomics Network (CAfGEN, includes among its objectives the identification of host genetic factors associated with TB disease progression in HIV-positive children [Citation56]) are also required.
In this systematic review and meta-analysis, a total of 7960 patients from 18 studies were included in qualitative analysis. However, only one study provided two cohorts for quantitative synthesis that showed that low expression MIF−794 CATT5,6 genotypes were not associated with tuberculosis (TB) infectivity (OR = 1.31, 95% CI: 0.46–3.79). This genetic polymorphism is known to affect expression of pro-inflammatory cytokines which are key in defense against TB infection.
The most explored clinical outcome was TB infectivity (11 studies) alongside; drug induced liver disease, peripheral neuropathy, mortality, cure and lung function. However, different genetic variants were explored which limited the extent to which quantitative synthesis could be performed.
Most of the studies included in the review lacked the methodological rigor appropriate for genetic studies; hence, individual study findings should be interpreted with caution.
Little evidence was found to support the role of genetic factors in influencing TB clinical outcomes in HIV-infected Black African patients, highlighting the need for more high-quality genetic research in sub-Saharan Africa.
Author contributions
All authors participated in the conception and design of the work. IG Asiimwe was responsible for literature retrieval and screening, data extraction analysis and first drafting of the manuscript; D Kiiza and S Walimbwa were responsible for quality control aspects related to literature retrieval, screening, data extraction and analysis and revisions to the draft manuscript; CW Sekaggya was responsible for overall supervision, final review and approval of the final version of the manuscript.
Supplemental Material 1
Download MS Word (172.6 KB)Acknowledgments
The authors would like to thank all the authors whose articles are referenced in our study.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: www.futuremedicine.com/doi/suppl/10.2217/pgs-2021-0096
Financial & competing interests disclosure
The authors have no financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
- Chakaya J , KhanM , NtoumiFet al. Global Tuberculosis Report 2020 – reflections on the global TB burden, treatment and prevention efforts. Int. J. Infect. Dis.10.1016/j.ijid.2021.02.107 (2021).
- Frank TD , CarterA , JahagirdarDet al. Global, regional, and national incidence, prevalence, and mortality of HIV, 1980–2017, and forecasts to 2030, for 195 countries and territories: a systematic analysis for the Global Burden of Diseases, Injuries, and Risk Factors Study 2017. Lancet HIV6(12), e831–e859 (2019).
- Tuberculosis . https://www.unaids.org/en/topic/tuberculosis
- Ford N , MatteelliA , ShubberZet al. TB as a cause of hospitalization and in-hospital mortality among people living with HIV worldwide: a systematic review and meta-analysis. J. Int. AIDS Soc.19(1), 20714 (2016).
- Van Tong H , VelavanTP , ThyeT , MeyerCG. Human genetic factors in tuberculosis: an update. Trop. Med. Int. Health22(9), 1063–1071 (2017).
- Huang L , LiuC , LiaoG , YangX , TangX , ChenJ. Vitamin D receptor gene FOKI polymorphism contributes to increasing the risk of tuberculosis: an update meta-analysis. Medicine94(51), e2256 (2015).
- Xu C , TangP , DingCet al. Vitamin D receptor gene FOKI polymorphism contributes to increasing the risk of HIV-negative tuberculosis: evidence from a meta-analysis. 10(10), e0140634 (2015).
- Zhao L , LiuK , KongX , TaoZ , WangY , LiuY. Association of polymorphisms in Toll-like receptors 4 and 9 with risk of pulmonary tuberculosis: a meta-analysis. Med. Sci. Monit.21, 1097–1106 (2015).
- Yi YX , HanJB , ZhaoL , FangY , ZhangYF , ZhouGY. Tumor necrosis factor alpha gene polymorphism contributes to pulmonary tuberculosis susceptibility: evidence from a meta-analysis. Int. J. Clin. Exp. Med8(11), 20690–20700 (2015).
- Asiimwe IG , KiizaD , WalimbwaS , Sekaggya-WiltshireC. Genetic factors associated with tuberculosis-related outcomes in HIV-infected Black-African patients: a systematic review and meta-analysis protocol. Prospero (2021). www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021237551
- Moher D , LiberatiA , TetzlaffJ , AltmanDG. Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med.6(7), e1000097 (2009).
- R Core Team . R: a language and environment for statistical computing (2018). https://www.R-project.org
- Jorgensen AL , WilliamsonPR. Methodological quality of pharmacogenetic studies: issues of concern. Stat. Med.27(30), 6547–6569 (2008).
- Minelli C , ThompsonJR , AbramsKR , ThakkinstianA , AttiaJ. The choice of a genetic model in the meta-analysis of molecular association studies. Int. J. Epidemiol.34(6), 1319–1328 (2005).
- Asiimwe IG , ZhangEJ , OsanlouRet al. Genetic factors influencing warfarin dose in Black-African patients: a systematic review and meta-analysis. Clin. Pharmacol. Ther.107(6), 1420–1433 (2020).
- Schwarzer G . Meta: an R package for meta-analysis. R. News7(3), 40–45 (2007).
- Asiimwe IG , PushpakomS , TurnerRM , Kolamunnage-DonaR , JorgensenAL , PirmohamedM. Cardiovascular drugs and COVID-19 clinical outcomes: a living systematic review and meta-analysis. Br. J. Clin. Pharmacol. doi:10.1111/bcp.14927 (2021) ( Epub ahead of print).
- Morales DR , ConoverMM , YouSCet al. Renin-angiotensin system blockers and susceptibility to COVID-19: an international, open science, cohort analysis. Lancet Digit Health3(2), e98–e114 (2021).
- Higgins J , GreenSE. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011] (2011).
- Ioannidis JP , BoffettaP , LittleJet al. Assessment of cumulative evidence on genetic associations: interim guidelines. Int. J. Epidemiol.37(1), 120–132 (2008).
- Fitness J , FloydS , WarndorffDKet al. Large-scale candidate gene study of tuberculosis susceptibility in the Karonga district of northern Malawi. Am. J. Tropical Med. Hygiene71(3), 341–349 (2004).
- Søborg C , AndersenAB , RangeNet al. Influence of candidate susceptibility genes on tuberculosis in a high endemic region. Mol. Immunol.44(9), 2213–2220 (2007).
- Range N , AndersenAB , MagnussenP , MugomelaA , FriisH. The effect of micronutrient supplementation on treatment outcome in patients with pulmonary tuberculosis: a randomized controlled trial in Mwanza, Tanzania. Trop. Med. Int. Health10(9), 826–832 (2005).
- Yimer G , UedaN , HabtewoldAet al. Pharmacogenetic & pharmacokinetic biomarker for efavirenz based ARV and rifampicin based anti-TB drug induced liver injury in TB-HIV infected patients. PLoS ONE6(12), e27810 (2011).
- Benichou C . Criteria of drug-induced liver disorders. Report of an international consensus meeting. J. Hepatol.11(2), 272–276 (1990).
- Hardwick RJ , AmogneW , MugusiSet al. β-defensin genomic copy number is associated with HIV load and immune reconstitution in sub-saharan Africans. J. Infect. Dis.206(7), 1012–1019 (2012).
- Mugusi SF , NgaimisiE , JanabiMYet al. Risk factors for mortality among HIV-positive patients with and without active tuberculosis in Dar es Salaam, Tanzania. Antivir Ther17(2), 265–274 (2012).
- Machado LR , BowdreyJ , NgaimisiEet al. Copy number variation of Fc gamma receptor genes in HIV-infected and HIV-tuberculosis co-infected individuals in sub-Saharan Africa. PloS ONE8(11), e78165 (2013).
- Dhoro M , NgaraB , KadzirangeG , NhachiC , MasimirembwaC. Genetic variants of drug metabolizing enzymes and drug transporter (ABCB1) as possible biomarkers for adverse drug reactions in an HIV/AIDS cohort in Zimbabwe. Curr. HIV Res.11(6), 481–490 (2013).
- Nemaura T , DhoroM , NhachiC , KadzirangeG , ChonziP , MasimirembwaC. Evaluation of the prevalence, progression and severity of common adverse reactions (lipodystrophy, cns, peripheral neuropathy, and hypersensitivity reactions) associated with anti-retroviral therapy (ART) and anti-tuberculosis treatment in outpatients in Zimbabwe. J. AIDS. Clin. Res.4(4), 1–7 (2013).
- Samie A , DzhivhuhoGA , NangammbiTC. Distribution of CXCR2 +1208 T/C gene polymorphisms in relation to opportunistic infections among HIV-infected patients in Limpopo Province, South Africa. Genet. Mol. Res.13(3), 7470–7479 (2014).
- Samie A , MoloroGT , NangammbiTC. Interleukin-7 receptor gene polymorphism at +1237 locus and its effect on susceptibility to opportunistic infections among HIV and AIDS patients in Limpopo Province, South Africa. Genet. Mol. Res.13, 8757–8766 (2014).
- Dzhivhuho GA , NangammbiTC , SamieA. Association of interleukin-8 gene polymorphisms in HIV patients with opportunistic infections in Limpopo Province, South Africa. Genet. Mol. Res.15(1), 15017466 (2016).
- Sobota RS , SteinCM , KodamanNet al. A locus at 5q33.3 confers resistance to tuberculosis in highly susceptible individuals. Am. J. Hum. Genet.98(3), 514 (2016).
- Sobota RS , SteinCM , KodamanNet al. A chromosome 5q31.1 locus associates with tuberculin skin test reactivity in HIV-positive individuals from tuberculosis hyper-endemic regions in east Africa. PLoS Genet.13(6), e1006710 (2017).
- Petros Z , LeeMTM , TakahashiAet al. Genome-wide association and replication study of hepatotoxicity induced by antiretrovirals alone or with concomitant anti-tuberculosis drugs. OMICS21(4), 207–216 (2017).
- Aithal GP , WatkinsPB , AndradeRJet al. Case definition and phenotype standardization in drug-induced liver injury. Clin. Pharmacol. Ther.89(6), 806–815 (2011).
- Ravimohan S , NfanyanaK , TamuhlaN , TiemessenCT , WeissmanD , BissonGP. Common variation in NLRP3 is associated with early death and elevated inflammasome biomarkers among advanced HIV/TB co-infected patients in Botswana. Open Forum Infectious Dis.5(5), ofy075 (2018).
- Ravimohan S , TamuhlaN , SteenhoffAPet al. Early immunologic failure is associated with early mortality among advanced HIV-infected adults initiating antiretroviral therapy with active tuberculosis. J. Infect. Dis.20811(1784), 1793 (2013).
- Calcagno A , CusatoJ , Sekaggya-WiltshireCet al. The influence of pharmacogenetic variants in HIV/tuberculosis coinfected patients in Uganda in the SOUTH study. Clin. Pharmacol. Ther.106(2), 450–457 (2019).
- Sekaggya-Wiltshire C , Von BraunA , LamordeMet al. Delayed sputum culture conversion in tuberculosis-human immunodeficiency virus-coinfected patients with low isoniazid and rifampicin concentrations. Clin. Infect. Dis.67(5), 708–716 (2018).
- Reid D , ShenoiS , LengLet al. Low expression macrophage migration inhibitory factor (MIF) alleles and tuberculosis in HIV infected South Africans. Cytokine: X1(1), 100004(2019).
- Mthiyane T , RustomjeeR , PymASet al. N-acetyltransferase 2 genotypes among Zulu-speaking South Africans and isoniazid and N-acetyl-isoniazid pharmacokinetics during antituberculosis treatment. Antimicrob. Agents Chemother.64(4), (2020).
- Mcilleron H , RustomjeeR , VahediMet al. Reduced antituberculosis drug concentrations in HIV-infected patients who are men or have low weight: implications for international dosing guidelines. Antimicrob. Agents Chemother.56(6), 3232–3238 (2012).
- Naiker S , ConnollyC , WiesnerLet al. Randomized pharmacokinetic evaluation of different rifabutin doses in African HIV- infected tuberculosis patients on lopinavir/ritonavir-based antiretroviral therapy. BMC Pharmacol. Toxicol.15, 61 (2014).
- Ravimohan S , MaenetjeP , AuldSCet al. A common NLRC4 gene variant associates with inflammation and pulmonary function in human immunodeficiency virus and tuberculosis. Clin. Infect. Dis.71(4), 924–932 (2020).
- Seedat F , JamesI , LoubserSet al. Human leukocyte antigen associations with protection against tuberculosis infection and disease in human immunodeficiency virus-1 infected individuals, despite household tuberculosis exposure and immune suppression. Tuberculosis126, 102023 (2021).
- PharmGKB . Tuberculosis. (2021).
- Whirl-Carrillo M , McdonaghEM , HebertJMet al. Pharmacogenomics knowledge for personalized medicine. Clin. Pharmacol. Ther.92(4), 414–417 (2012).
- Chen BF , WangR , ChenYJ , ZhuY , DingL , WenYF. Association between HLA-DRB1 alleles and tuberculosis: a meta-analysis. Genet. Mol. Res.14(4), 15859–15868 (2015).
- Li C , ZhouY , XiangX , ZhouY , HeM. The relationship of HLA-DQ alleles with tuberculosis risk: a meta-analysis. Lung193(4), 521–530 (2015).
- De Albuquerque AC , RochaLQ , DeMorais Batista AH , TeixeiraAB , DosSantos DB , NogueiraNA. Association of polymorphism +874 A/T of interferon-gamma and susceptibility to the development of tuberculosis: meta-analysis. Eur. J. Clin. Microbiol. Infect. Dis.31(11), 2887–2895 (2012).
- Thompson SG , HigginsJP. How should meta-regression analyses be undertaken and interpreted?Stat. Med.21(11), 1559–1573 (2002).
- Matimba A , DhoroM , DandaraC. Is there a role of pharmacogenomics in Africa. Global Health Epidemiol. Genom.1 (2016).
- Campbell MC , TishkoffSA. African genetic diversity: implications for human demographic history, modern human origins, and complex disease mapping. Ann. Rev. Genom. Hum. Genet.9(1), 403–433 (2008).
- Mboowa G , MwesigwaS , KatagiryaEet al. The Collaborative African Genomics Network (CAfGEN): applying Genomic technologies to probe host factors important to the progression of HIV and HIV-tuberculosis infection in sub-Saharan Africa. AAS Open Res.1, 3 (2018).