Abstract
Objective: To describe a case series of patients presenting with autoimmune hepatitis after initiation of antiretroviral therapy.
Materials and methods: The demographics, clinical and laboratory features, and therapeutic response of HIV-infected patients on antiretroviral therapy presenting to our Division between November 2011 and November 2014 with elevated liver enzymes, were analysed.
Results: Nine patients with elevated liver enzymes, immunoglobulin G and autoimmune markers in keeping with autoimmune hepatitis were identified. All were anti-hepatitis C virus negative. One patient was hepatitis B surface antigen positive but his hepatitis B viral load was undetectable. All patients denied using any traditional herbal remedies. Liver histology was consistent with autoimmune hepatitis showing interface hepatitis and infiltrates of lymphocytes and plasma cells. Diagnosis was made according to the Autoimmune Hepatitis Group Scoring Systems. All patients were started on 15–20 mg of oral prednisone with clinical and biochemical improvement after 1–6 weeks.
Conclusions: Immune reconstitution related autoimmune hepatitis should be considered in the differential diagnosis of hepatitis in the HIV-infected patient on antiretroviral therapy. Liver biopsy should be performed and the diagnosis confirmed using scoring systems developed by the Autoimmune Hepatitis Group. Timely treatment with prednisone and other agents for autoimmune hepatitis is indicated, and can be lifesaving in acute liver failure.
Acknowledgements
I, Eric Murunga would like to express my sincere gratitude to Professor Christo Van Rensburg, my research supervisor for his enthusiastic encouragement and patient guidance, ideas and corrections during this research work. I would also like to thank Dr Monique Andersson for planting the seeds of this research work, ideas, tirelessly looking for, and following patients and helping to keep my progress on schedule. Finally, I thank Joy my wife and my children Joshua and Timothy for their support and patience.
Disclosure statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
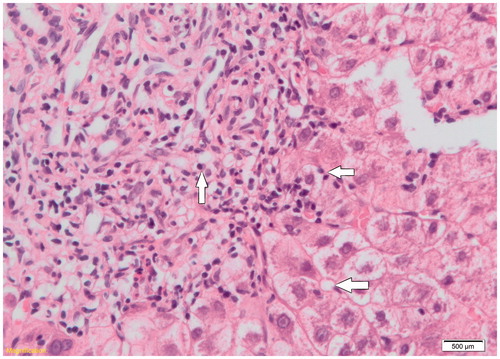
Figure 1. Patient 7’s histopathology slide showing lymphoplasmacytic infiltrates (left arrow), possible emperipolesis (top right arrow), and hepatic rosette formation (bottom arrow). Haematoxylin and eosin stain was used.