

Introduction
Hemimegalencephaly (HME) is a rare congenital malformation of cortical development, characterised by enlargement and hypertrophy of all, or some, of one cerebral hemisphere (CitationAlvarez et al. 2011). HME can be isolated or syndromic, and the syndromic form may be associated with cutaneous malformations (CitationSasaki et al. 2005). Imaging of the affected hemispheres may reveal signs of abnormal gyration, variable types of cortical malformation, dilated and/or constricted ipsilateral ventricles, displacement of the occipital lobe across the midline, thickened ipsilateral corpus callosum and, in rare cases, hypertrophy of the ipsilateral brain stem and cerebellum (CitationFlores-Sarnat 2002). Here, we describe a case of HME accompanied by fetal high-output congestive heart failure due to decreased inter-cerebral vascular resistance and increased blood flow.
Case report
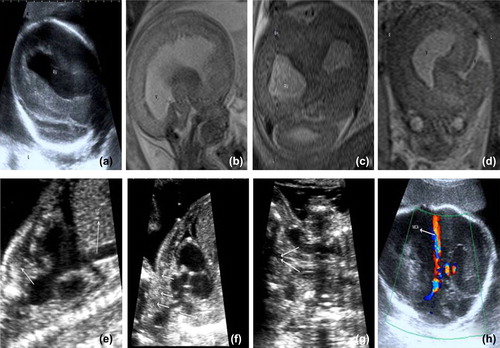
A 36-year-old woman, gravida 2, para 1, was referred to our department at 21 weeks’ gestation for detailed sonography due to a suspected cerebral malformation. A detailed evaluation revealed macrocrania, asymmetry of cerebral hemispheres, ventricular dilation, displacement of the occipital lobe across the midline, absence of the corpus callosum and colpocephaly (). Fetal echocardiography revealed no abnormalities, and fetal magnetic resonance imaging (MRI) was performed. The MR images revealed a significant increase in the volume of the right hemisphere. The cortical thickness of the right hemisphere was increased, and a subcortical band of heterotopic grey matter was also noted, in addition to sulcation and gyration anomalies in the right hemisphere. The absence of corpus callosum was also observed (). These radiological findings confirmed the diagnosis of HME and subcortical band heterotopia. The family was given detailed information about the expected impaired fetal neurological outcome, and the termination of the pregnancy was discussed. The family refused a termination and decided to carry on with the pregnancy. Sonographical evaluation at 24 weeks’ gestation revealed fetal hydrops and sinus tachycardia, with atrioventricular and ventriculoatrial concordance. Moderate cardiomegaly was observed, with right atrial, right ventricular and superior vena caval dilation (). The ascending aorta and brachiocephalic artery were dilated (). The bilateral internal jugular veins were dilated (). The aortic arch was 2.6 mm, and the velocity of the blood flow in the ascending aorta was 1.5 m/s. The aortic isthmus and transverse arch appeared hypoplastic, with turbulent flow across the area of narrowing (). The flow velocity in the aortic isthmus was 1.5 m/s, and this increased flow was considered a pseudocoarctation secondary to the increased low-resistance distal circulation, as no cardiac abnormality was observed in the preceding echocardiographical evaluation performed at 21 weeks’ gestation. Pulse and colour Doppler velocity waveforms of the middle cerebral artery also revealed increased velocity (). These findings were mostly consistent with fetal high-output congestive heart failure and impending fetal hydrops secondary to HMC.
Fetal demise was confirmed in the sonographical evaluation at 25 weeks’ gestation. A post-mortem was not performed after the delivery of the infant, as the parents did not give consent for the procedure.
Discussion
The pathogenesis of HME has been attributed to a variety of mechanisms, including disturbances in cellular lineages and proliferation (CitationBarkovich et al. 2001, CitationSalamon et al. 2006), differentiation (CitationFlores-Sarnat 2002), migration (CitationBarkovich and Chuang 1990, CitationBattaglia et al. 2006), gene expression (CitationYu et al. 2005) and growth factors (CitationAntonelli et al. 2004). The human fetal brain undergoes significant growth throughout intrauterine life. Major developmental events, such as neuronal proliferation and migration, occur during the first half of gestation (CitationBarkovich et al. 2001). In general, the disturbances associated with HME are thought to occur between 12 and 20 weeks’ gestation (CitationBarkovich and Chuang 1990; CitationBattaglia et al. 2006).
The severity of HME is graded into three groups. Grade-1 HME is characterised by mild enlargement in the affected hemisphere and mild ventricular asymmetry, with straightening of the frontal horn. Patients with Grade-2 HME mostly present with moderate hemispheric enlargement, slight displacement of the midline, moderate ventriculomegaly and colpocephaly. In contrast, Grade-3 HME is characterised by significant hemispheric enlargement, marked distortion of the midline and severe ventriculomegaly and lissencephaly (CitationFlores-Sarnat 2002). It is important to emphasise that both the isolated and syndromic forms share a common set of neuroimaging findings (CitationFlores-Sarnat 2002).
Prenatal ultrasound features of HME, are macrocephaly, with marked ventricular asymmetry, a midline shift accompanied by displacement of the occipital lobe across the midline and large dilatation, which occurs mainly at the posterior horn of the affected lateral ventricle (CitationRomero et al. 2011). MRI is helpful to confirm and define the brain abnormalities. MRI allows better differentiation of the type, extension and localisation of the cortical malformations (CitationRomero et al. 2011).
Previous reports have provided insufficient information on the prenatal and neonatal echocardiographical findings that can accompany HME. As shown in the present case, HME can be associated with congestive heart failure, resulting from the decreased resistance and increased blood flow and may lead to in utero or neonatal death. We observed a dilated superior vena cava, with right atrial and right ventricular dilation due to the increased cardiac preload. In addition, the ascending aorta and the brachiocephalic vessels supplying the afferent flow to the HME are markedly dilated due to the diminished afterload afforded by the highly compliant cerebral circulation.
HME may be associated with congestive heart failure due to brain circulation. Cardiac failure and associated brain pathologies may be indicators of the survival of patients with this condition.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Alvarez RM, Garcia-Diaz L, Marquez J, Fajardo M, Rivas E, Garcia-Lozano JC et al. 2011. Hemimegalencephaly: prenatal diagnosis and outcome. Fetal Diagnosis and Therapy 30:234–238.
- Antonelli A, Chiaretti A, Amendola T, Piastra M, Di Rocco C, Aloe L. 2004. Nerve growth factor and brain-derived neurotrophic factor in human paediatric hemimegalencephaly. Neuropediatrics 35:39–44.
- Barkovich AJ, Chuang SH. 1990. Unilateral megalencephaly: correlation of MR imaging and pathologic characteristics. AJNR. American Journal of Neuroradiology 11:523–531.
- Barkovich AJ, Kuzniecky RI, Jackson GD, Guerrini R, Dobyns WB. 2001. Classification system for malformations of cortical development: update 2001. Neurology 57:2168–2178.
- Battaglia D, Chieffo D, Lettori D, Perrino F, Di Rocco C, Guzzetta F. 2006. Cognitive assessment in epilepsy surgery of children. Child's Nervous System: ChNS: Official Journal of the International Society for Pediatric Neurosurgery 22:744–759.
- Flores-Sarnat L. 2002. Hemimegalencephaly: part 1. Genetic, clinical, and imaging aspects. Journal of Child Neurology 17:373–384; discussion 384.
- Romero XC, Molina FS, Pastor E, Amaya F. 2011. Hemimegalencephaly: 2D, 3D ultrasound and MRI correlation. Fetal Diagnosis and Therapy 29:257–260.
- Salamon N, Andres M, Chute DJ, Nguyen ST, Chang JW, Huynh MN et al. 2006. Contralateral hemimicrencephaly and clinical-pathological correlations in children with hemimegalencephaly. Brain: A Journal of Neurology 129:352–365.
- Sasaki M, Hashimoto T, Furushima W, Okada M, Kinoshita S, Fujikawa Y et al. 2005. Clinical aspects of hemimegalencephaly by means of a nationwide survey. Journal of Child Neurology 20:337–341.
- Yu J, Baybis M, Lee A, Mckhann G II, Chugani D, Kupsky WJ et al. 2005. Targeted gene expression analysis in hemimegalencephaly: activation of beta-catenin signaling. Brain Pathology 15:179–186.