To the Editor
Chemotherapy is an integral part of today's multimodality cancer treatment. Side effects related to chemotherapy such as vomiting or weight loss are well known and treated routinely. Weight gain on the other hand is an often neglected problem although it has an important impact on both patient's quality of life and cancer prognosis. Analysis of the impressive weight gain in this case report clearly highlights the problem.
A 40-year-old premenopausal female patient in excellent general health was diagnosed in our institute in April 2006 with a locally advanced rectal cancer, cT4 cN1 cM0. The patient is a non-smoking, top female athlete and professional badminton teacher, who exercised three hours per day in addition to teaching badminton during the rest of the day. There was no incidence of weight changes before cancer diagnosis in our 162 cm tall patient. After establishing a protective colostomy neoadjuvant radiochemotherapy was started, during which the patient gained 2.7 kg body weight.
In June 2006, three weeks after radiochemotherapy, a pT4 pN1 tumor was successfully resected and adjuvant chemotherapy was started. In December 2006 the patient had gained another 12.5 kg body weight, when a seizure struck her. A CT scan showed left cerebral vein thrombosis of the inferior anastomotic vein of Labbé, the transverse sinus, the sigmoid sinus and the internal jugular vein. Extensive investigations did not identify any predisposing reason or underlying condition. Thus we concluded on a multifactorial origin; we hypothesized that chemotherapy-induced hypercoagulability, antiemetic steroid medication and the patient's physical inactivity likely induced a prothrombotic state. We suspected that the significant weight gain might in itself have also contributed to the thrombosis Citation[1]. The patient was put on Valproate for seizure control and anticoagulated with low molecular heparin followed by acenocoumarol. Adjuvant chemotherapy was not reintroduced.
From start of treatment in April 2006 until October 2007 the patient's body weight increased from 61.8 kg to 87 kg, i.e. a total weight gain of 25.2 kg in 18 months. Being a top athlete, the patient had regular follow-up at the Swiss Accident Insurance Fund where her body composition was regularly monitored before, during and after treatment (), indicating that weight gain was almost entirely due to an increase in body fat, amounting to at least 20.9 kg. Full work-up excluded all most common causes of obesity Citation[2] ().
Figure 1. Body composition changes in our patient. While absolute fat free mass remained constant during time, the patient gained 20.9 kg of body fat over the course of the study. Relative body fat, in 2005, measured at 22.8%; this value nearly doubled to 42.5% by 2008.
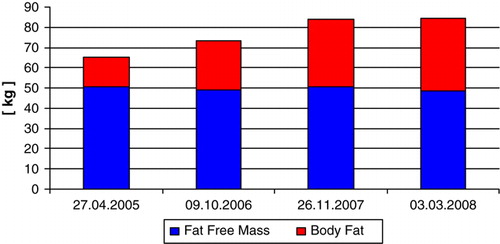
Table I. Differential diagnosis Citation[2] and diagnostic workup
We interpreted the impressive weight gain in our patient to be a consequence of several factors. First, energy expenditure before and after treatment start varied greatly in this female top athlete. Unchanged eating habits lead to a significant disparity between energy expenditure and caloric uptake. We estimated that her usual daily expenditure before treatment was two times that during treatment, thus fully explaining the weight gain. Additionally, chemotherapy had induced early menopause, a known cause of weight gain. Finally, the cerebral vein thrombosis and its anticoagulation postponed the restart of the patient's usual physical activities.
Weight gain during adjuvant chemotherapy is a well-known phenomenon affecting 60 to 90% of patients Citation[3–9], ranging from 2 to 6 kg depending on disease and treatment Citation[3], Citation[10]. Despite numerous publications, weight gain remains a neglected problem in daily routine. Aetiology remains unclear, but a disparity between calorie needs and nutrient energy intake might be the single most important reason Citation[4], Citation[5]. Diminished activity and energy expenditure along with unchanged eating habits lead to significant changes in body composition Citation[4–8], Citation[10] including increased total and relative body fat mass, and decreased relative fat-free mass whereas absolute fat-free mass remains stable ().
Menopausal women, especially during the onset of menopause Citation[3], Citation[6], are at an increased risk of gaining weight. Disease stage at diagnosis, duration of adjuvant treatment, use of multiagent regimens, oral chemotherapy Citation[6], Citation[9] and the comedication might also increase the risk of weight gain, while high body mass index before diagnosis, age older than 50 years and high education level Citation[9] are inversely associated with weight gain.
Weight gain, obesity and physical inactivity are not only risk factors for cardiovascular disease but also for cancer development and outcome Citation[11]. Obese patients are at an increased risk to develop rectal cancer Citation[12], colon cancer relapse and a secondary primary colon tumor Citation[13]. Physical inactivity increases the risk of death fourfold in breast cancer patients Citation[14], while physically inactive colon cancer patients are twice as likely to die from the disease compared to their physically active counterparts Citation[15].
The more than 20 kg gain in fatty body mass in our patient illustrates the common, but often neglected and therefore undertreated problem of weight gain during chemotherapy. Current efforts in oncological practice focus on avoiding weight loss, but – unfortunately – not to enforce physical activity and continuing previous daily activities. This might be due to misconceptions about the hazards of weight gain during chemotherapy, by both the patient as well as the team treating the patient.
Weight gain management during chemotherapy remains an important clinical challenge. Therefore, further efforts should be taken to avoid significant weight gain as this negatively impacts on daily life and worsens cancer prognosis. Oral or written weight management instruction, as well as group exercises suited to the specific population may prove to be beneficial for patients. Our patient received nutritional counselling and was encouraged to re-engage again in athletic activity, as soon as she recovered from the cerebral vein thrombosis.
Acknowledgements
CR was responsible for conception and writing of the article and for patient care; DG supervised radiologic imaging and supervised the case; SL supervised the case; MM was responsible for conception and writing of the article and supervised patient care. Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal. Declaration of interest: The authors declare that they have no competing interests.
References
- Stein PD, Beemath A, Olson RE. Obesity as a risk factor in venous thromboembolism. Am J Med 2005; 118: 978–80
- Uptodate, http://www.uptodateonline.com/online/content/image.do;jsessionid=CE23B6DBF597D2D26F26307CD4DE5295.0604?imageKey=endo_pix/etiolo1.htm&title=Etiology%20of%20obesity. accessed Nov 6, 2008.
- Camoriano JK, Loprinzi CL, Ingle JN, Therneau TM, Krook JE, Veeder MH. Weight change in women treated with adjuvant therapy or observed following mastectomy for node-positive breast cancer. J Clin Oncol 1990; 8: 1327–34
- Harvie MN, Campbell IT, Baildam A, Howell A. Energy balance in early breast cancer patients receiving adjuvant chemotherapy. Breast Cancer Res Treat 2004; 83: 201–10
- Harvie MN, Howell A, Thatcher N, Baildam A, Campbell I. Energy balance in patients with advanced NSCLC, metastatic melanoma and metastatic breast cancer receiving chemotherapy – a longitudinal study. Br J Cancer 2005; 92: 673–80
- Demark-Wahnefried, W, Rimer, BK, Winer, EP. Weight gain in women diagnosed with breast cancer. J Am Diet Assoc 1997;97:519–26, 529.
- Demark-Wahnefried W, Hars V, Conaway MR, Havlin K, Rimer BK, McElveen G, et al. Reduced rates of metabolism and decreased physical activity in breast cancer patients receiving adjuvant chemotherapy. Am J Clin Nutr 1997; 65: 1495–501
- Demark-Wahnefried W, Peterson BL, Winer EP, Marks L, Aziz N, Marcom PK, et al. Changes in weight, body composition, and factors influencing energy balance among premenopausal breast cancer patients receiving adjuvant chemotherapy. J Clin Oncol 2001; 19: 2381–9
- Rock, CL, Flatt, SW, Newman, V, Caan, BJ, Haan, MN, Stefanick, ML, , et al. Factors associated with weight gain in women after diagnosis of breast cancer. J Am Diet Assoc 1999;99:1212–18, 1221.
- Freedman RJ, Aziz N, Albanes D, Hartman T, Danforth D, Hill S, et al. Weight and body composition changes during and after adjuvant chemotherapy in women with breast cancer. J Clin Endocrinol Metab 2004; 89: 2248–53
- Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M. Body-mass index and incidence of cancer: A systematic review and meta-analysis of prospective observational studies. Lancet 2008; 371: 569–78
- Dai Z, Xu YC, Niu L. Obesity and colorectal cancer risk: A meta-analysis of cohort studies. World J Gastroenterol 2007; 13: 4199–206
- Dignam JJ, Polite BN, Yothers G, Raich P, Colangelo L, O'Connell MJ, et al. Body mass index and outcomes in patients who receive adjuvant chemotherapy for colon cancer. J Natl Cancer Inst 2006; 98: 1647–54
- Irwin ML, Wilder Smith A, McTiernan A, Ballard-Barbash R, Cronin K, Gilliland FD, et al. Influence of pre- and postdiagnosis physical activity on mortality in breast cancer survivors: The health, eating, activity, and lifestyle study. J Clin Oncol 2008; 26: 3958–64
- Meyerhardt JA, Heseltine D, Niedzwiecki D, Hollis D, Saltz LB, Mayer RJ, et al. Impact of physical activity on cancer recurrence and survival in patients with stage III colon cancer: Findings from CALGB 89803. J Clin Oncol 2006; 24: 3535–41