To the Editor,
The haemophagocytic syndrome (HPS) is a rare complication of solid tumours, especially of prostate cancer [Citation1,Citation2]. We report a case of HPS responsible for a severe haemorrhage, and which was successfully treated with chemotherapy.
A 57-year-old man presented with a metastatic prostate cancer (multiple bone lesions, PSA > 120 ng/ml, Gleason 8). The complete androgenic blockade (gosereline + bicalutamide) was effective until May 2010 until PSA rose from 20 to 47 ng/ml and new bone lesions appeared. The patient was then considered for chemotherapy with docetaxel. An implanted port was inserted with the following haematological parameters: haemoglobin 9 g/dl, 67 000 platelets/mm3, and prothrombin ratio 75%. The day after, the patient was admitted to the emergency room because of a major haematoma around the implanted part, and some bleeding through the surgical wound. This required the ablation of the CVC, and the administration of platelet units, erythrocyte units, and frozen plasma. The biological parameters which suggested a diagnosis of HPS were: anaemia (6 g/dl), thrombopenia (45 000/mm3), leucopenia (2600/mm3), abnormal ferritine (5.8 times upper limit of normal), and abnormal fibrinogen (1.36 g/l; normal value 2–4). The bone marrow aspirates revealed the presence of many activated macrophages (), but no prostate carcinoma cells. We excluded the following diagnoses: auto-immune haemolytic anaemia, auto-immune thrombopenia, haemolytic and uremic syndrome, bone narrow involvement, vitamin deficiencies and infections by HIV and hepatitis virus. Despite the absence of fever and splenomegaly, we retained the diagnosis of HPS. Because of the severity of the related thrombopenia, the patient received two cycles of weekly vincristin (2 mg/cycle) followed by six cycles of docetaxel (75 mg/m²/3 weeks). With this treatment, the general condition of this patient improved and all the biological abnormalities returned back to normal. Eleven months later, the patient was in good shape and the prostate cancer was stable, without any recurrence of the HPS.
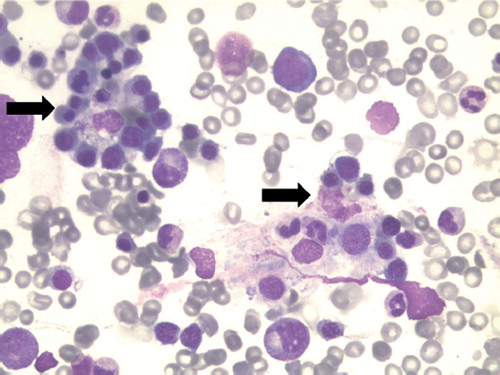
Figure 1. Haemophagocytosis observed in a bone marrow aspirate. Shown are two histiocytes (arrows) containing numerous haematopoietic elements within their cytoplasm (Wright-Giemsa stain).
HPS is a rare complication of malignancies. It is characterised by fever, pancytopenia, splenomegaly, coagulation abnormalities, increased ferritine, and haemophagocytosis in the bone marrow, liver or lymph nodes. The treatment of the HPS is the treatment of its cause. Some conditions have been suspected to trigger HPS: tumour secretion of cytokines, intensive chemotherapy, or infectious complications. The prognosis of HPS associated to metastatic cancer is very poor with an early death rate of about 40–80% [Citation1–3]. Up to now, two cases of HPS related to a prostate cancer have been reported; one caused by a sepsis due to Escherichia coli [Citation4] and the second case caused by with a massive intra-medullary extension [Citation5]. Our case illustrates the fact that the incidence of HPS may be underestimated in routine practice. The presence of activated macrophages in the bone marrow aspirate is highly suggestive of HPS. In this context, adequate chemotherapy could reverse this severe complication.
References
- Arico M, Danesino C, Pende D, Moretta L. Pathogenesis of harmophagocytic lymphohistiocytosis. Br J Haematol 2001; 114:761–9.
- Henter JI, Horne A, Arico M, Egeler RM, Filipovich AH, Imashuku S, . Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer 2007;48:124–31.
- Reiner A, Spivak J. Hematophagic histiocytosis: A report of 23 new patients and a review of the literature. Medicine 1988;67:369–88.
- El Khoury N, Lassoued K, Pellé G, Foucher A, Costa MA, Rondeau E, . Hemophagocytosis associated with an Escherichia coli sepsis: A case report. Rev Med Interne 2003;24:688–91.
- Koizumi K, Haseyama Y, Machino R, Sato Y, Sawada K, Koike T. The hemophagocytic syndrome in prostate cancer revealed by disseminated carcinomatosis of the bone marrow. J Urology 2002;168:1101–2.