
Abstract
Introduction: Multidetector-row computed tomography (MDCT) angiography is a reliable technique in preoperative renal anatomy evaluation in live renal donors. Objectives: To investigate the accuracy of early arterial phase findings and compares them with intraoperative findings. Methods: In this prospective study, 100 potential live donors undergoing preoperative MDCT and nephrectomy during 2010–2013 were included. The examination was performed with a 64-detector scanner including early arterial and venous phase. MDCT angiography started by bolus tracking and venous phase was acquired 9 s after arterial phase. Anatomical findings and vein and artery attenuation values were recorded and arterial phase findings were compared with intraoperative findings. Results: All anatomical findings reported by MDCT in early arterial phase were confirmed by intraoperative findings with sensitivity of 100%. Right renal vein was supernumerary in 17 cases and left renal vein was circumaortic in 3 and retroaortic in 5 cases. Renal arteries had early branching in 13, two arteries in 12 and accessory in 8 cases. Vein and artery attenuation values had significant difference between early arterial and venous phase (p < 0.001). Conclusion: Early arterial phase has similar results to venous phase in preoperative evaluation and intraoperative findings and could be used alone to reduce radiation dose.
Introduction
Renal transplantation represents the best available replacement treatment with better survival and quality of life for patients with end-stage renal disease. The shortage of organ donors has stimulated interest in living-related renal transplantation with better graft survival than cadaver donor.Citation1,Citation2 In living donor renal transplantation, preoperative anatomic and functional evaluation of donor kidneys for selection of a suitable donor and for planning surgery to decrease hospital stay and blood loss by reducing complications and to accelerate recovery is necessary.Citation3,Citation4
Preoperative radiologic evaluation of kidney donors is used to select the patient and the kidney to be harvested. Multidetector-row computed tomography (MDCT) angiography is a minimally invasive and well-established method for assessment of potential renal donors and obtaining kidney anatomy for the purposes of living kidney donation.Citation5–7 MDCT angiography has the advantage of assessing the main vessels (renal vein, renal artery), ureteral structure, renal parenchymal lesions, renal cystic diseases, tiny stones, and surrounding anatomic variants with one test.Citation8–10
Renal MDCT angiography includes unenhanced, arterial phase, and venous phase acquisitions.Citation11 Knowing the renal venous structure is essential for the evaluation of potential donor nephrectomy patients. The renal vein is the most important venous structure to evaluate before laparoscopic surgery. Venous structures are well enhanced and identified in venous phase, but it will substantially increase the radiation dose.Citation12 The renal veins are often visualized on arterial phase images and the accurate depiction of the renal venous anatomy on arterial phase imaging is previously reported.Citation13,Citation14
Almost all the kidney donors are young and healthy individuals, which make necessary the dose reduction of MDCT evaluation.Citation12 Due to the probable similar results in arterial phase in comparison to venous phase and lower dose of radiation, we aim to evaluate MDCT findings in early arterial phase and venous phase and compare them with findings of the nephrectomy.
Methods
In this prospective cross-sectional study, 100 consecutive potential living renal donors (91 male and 9 female with mean age of 28.14 ± 2.92) who underwent preoperative MDCT evaluation from January 2010 to January 2013 were included in this study. All candidates were evaluated using an MDCT scanner (Somatom Sensation 64; Siemens Medical Solutions, Forchheim, Germany). All patients gave written informed consent to participate in the study. The project was approved by the local Ethics Committee and conducted in accordance with the guidelines of the Declaration of Helsinki.
CT angiography was performed in the supine position using 120 kVp and 110 mA from the upper to lower poles. The area scanned extended from diaphragm to aortic bifurcation. The scanning parameters included a 64 × 0.625 mm collimation to obtain 0.6 mm-thick reconstruction, 0.5-mm reconstruction increment, and 0.5-s rotation time. The gantry speed was 0.33-s per rotation. The scanning delay time was determined using the bolus-tracking technique. An arterial scan of the abdomen was initiated 5 s after a threshold enhancement of 120 HU was reached in the lumen of the abdominal aorta at the level of the diaphragm and venous phase was initiated about 10 s after the end of the arterial phase. Intravenous contrast protocol was 85 mL of Visipaque 320 mg injected at a rate of 6 mL/s using an automatic single-head power injector through a 20-gauge IV catheter placed in an antecubital vein. There were no adverse reactions to the contrast material, such as renal toxicity, allergic reaction, or extravasation of contrast material.
The examinations were interpreted by an experienced abdominal radiologist before donor nephrectomy. The numbers and major variations of the renal arteries and veins were evaluated. Initial interpretations were compared with the surgical findings (the reference standard) and the accuracy of CT for the evaluation of renal vascular anatomy, particularly in terms of the numbers of arteries and veins, was determined. The accuracies of CT evaluations were derived from the donor side kidneys only, for which the surgical findings confirmed the anatomies. The radiologist also evaluated two vascular phase with regard to whether renal vessels were adequately enhanced; adequate enhancement was considered when both renal arteries and veins were well opacified throughout their entire length and the renal arteries could be easily differentiated from the renal veins, as the arteries enhanced stronger than did the veins. Imaging findings in arterial and venous phase were compared with surgical findings to define their accuracy in diagnosing renal anatomy.
Data analysis
All data were analyzed using SPSS statistical package version 16.0 (SPSS Inc., Chicago, IL). Continuous data with normal distribution are given as mean ± standard deviation, otherwise as median. Wilcoxon rank test was used for comparisons of renal artery and vein attenuation values between arterial and venous phase. A p value of 0.05 or less was considered significant.
Results
Of the 100 assessed candidates, 79 had left-side nephrectomy and 21 had right-side nephrectomy. The causes for right nephrectomy was right kidney cyst (1 case), vascular variation including early branching, left supernumerary and accessory arteries (12 cases), tissue scar and right kidney function reduction (8 cases).
Renal vein anatomy
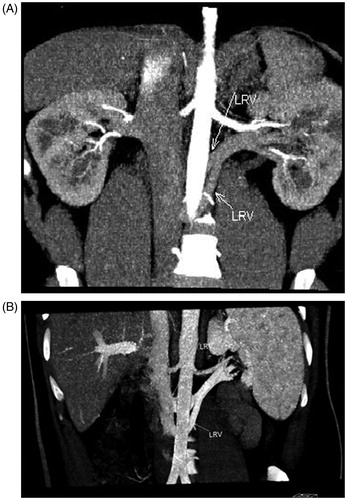
MDCT findings showed one renal vein in 83 and supernumerary veins in 17 cases including two renal veins () in 16 and three renal veins in 1 case in the right kidney. In the left kidney, venous variations were one renal vein in 92 cases, circumaortic left renal vein () in 3 and retroaortic left renal vein in 5 cases including 3 cases with one retroaortic vein, one case with three veins (two of them retroaortic veins) and one case with two vein with retroaortic route ().
Figure 1. MDCT angiogram in 32-year-old male renal donor with two right renal veins. Oblique coronal maximum intensity projection (MIP) of early arterial (A) and venous phase (B) images illustrate two right renal veins (arrows).
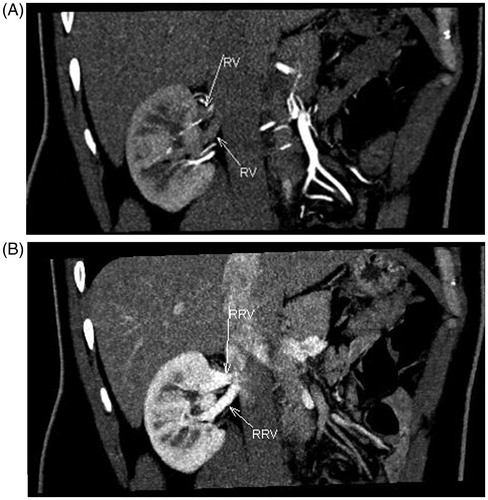
Figure 2. MDCT angiogram in 29-year-old male renal donor with circumaortic left renal vein. Oblique coronal MIP of early arterial (A) and venous (B) phase images illustrate circumaortic left renal vein (arrow). (C) Axial MIP of early arterial phase image reveal retroaortic component (arrow) of circumaortic left renal vein.
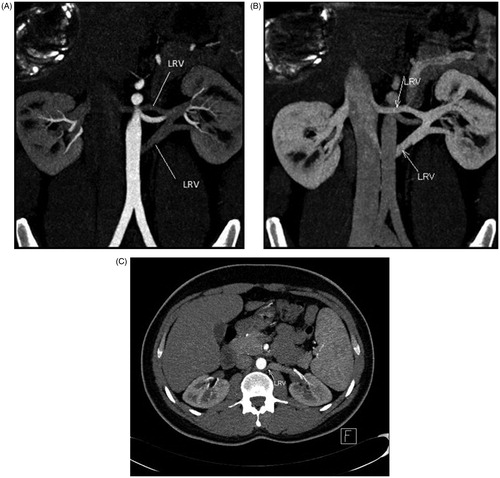
Figure 3. MDCT angiogram in 25-year- old male renal donor with two retroaortic left renal vein. Oblique coronal maximum intensity projection of early arterial (A) and venous (B) phase images show two retroaortic left renal veins (arrows).
Renal artery anatomy
Renal artery anatomy included one artery in 67 cases, twofold in 12 cases, early branching in 13 and accessory in 8 cases. Two arteries were observed in left side in 2 cases, in right side in 9 cases and in both sides in one case. Early branching was reported in left in 6 cases, in right in 5 cases and in both sides in 2 cases. Eight accessory renal arteries included 4 in left side, 3 in right side and one in both sides.
Vascular phase attenuation
In all patients, renal arteries and veins were adequately enhanced throughout their entire length, and renal arteries could be easily differentiated from renal veins because arteries showed stronger enhancement than did veins in artery phase and weaker enhancement in venous phase ().
Table 1. Vascular enhancement in early arterial and venous phases.
Of the 100 sides operated on, surgical findings corroborated the MDCT results in all cases. According to these findings, the sensitivity of early arterial phase imaging in the detection of the renal vascular was 100%.
Discussion
In recent years, there is a great interest in identifying methods to reduce radiation dose of MDCT angiography in healthy subjects. There are few reports considering arterial phase instead of venous phase for renal vasculature evaluation. In this study, we evaluated the accuracy of early arterial phase of MDCT in identification of renal vasculature and their variations in live renal donors. Early arterial phase findings about renal artery, vein and their variations were all confirmed by surgery evaluation, giving the accuracy and sensitivity of 100%.
MDCT accuracy is 90–100% in diagnosing main vessels and 75–100% in diagnosing minor vessels.Citation11,Citation15–17 In one of the few studies about arterial phase findings, Namasivayam and colleaguesCitation16 reported a 100% sensitivity of this phase in identifying renal veins.
Identifying renal vein anatomy is the most important evaluation, especially in laparoscopic surgery. It is necessary to identify main anomalies of left renal vein including retroaortic and circumaortic left renal vein, as it is at risk of unintentional injury during surgery. The reported incidence of multiple right renal veins ranged from 11% to 28% and 1–2% for multiple left renal veins;Citation18 as it is reported that single left retroaortic renal vein to be found in 2–3%.Citation9,Citation18
In our study, renal vein variations included 17 supernumery right veins, 3 left circumaortic and 5 retroaortic vein (2 with multiple veins) in early arterial phase. Zamboni et al.Citation19 found 9 venous variations among 50 live donors in arterial phase. Namasivayam et al.Citation16 in the study of 48 potential donors in the arterial phase found accessory right renal vein in 14 cases, left retroaortic vein in 2 and left circumaortic vein in 1 case. The differences in the reported variations between studies is justifiable according to the regional and race differences. However, it is important to note that in all these three studies, the accuracy of arterial phase in diagnosing renal veins and their variations was 100%.
Nephrectomy is usually performed in the kidney with more simple vascular anatomy to reduce complications during the surgery.Citation20,Citation21 Left kidney is the preferred site for nephrectomy, especially in laparoscopic surgery because it is easily accessible with longer renal vein and with no artery behind superior vena cava, as well as lower vascular complications and graft loss.Citation22 However, preoperative evaluation of accessory and early branching arteries are important especially in deciding nephrectomy site and the type of vascular anastomosis.Citation23–26
Holden et al.Citation27 reported early branching in 12%. Kawamoto et al.Citation10 reported 2 renal arteries in 16 and early branching in 14 donors (all in left renal artery) among 74 potential donors. In our study, also renal artery variations were reported in 23 cases including early branching in 13, two arteries in 12 and accessory arteries in 8 cases. All these variations were diagnosed in early arterial phase and proved by surgery. Twenty-one donors underwent right-side nephrectomy, of which 12 was due to early branching, 2 renal or accessory arteries in the left.
Considering the identification of renal vasculature with 100% accuracy in early arterial phase and the possible low-radiation dose, it could be concluded that early arterial phase is able to identify renal function and vasculature anatomy with high accuracy and venous phase could be omitted from preoperative MDCT evaluation to reduce radiation dose and cost burden. However, in this study we did not evaluated the received radiation dose in each phase and we cannot surely emphasize on the lower radiation dose of early arterial phase evaluations.
Declaration of interest
This research was financially supported by Vice Chancellor for Research, Tabriz University of Medical Sciences, Iran. The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the article.
References
- Kim J, Park S, Kim H, et al. Living donor kidneys: usefulness of multi-detector row CT for comprehensive evaluation. Radiology. 2003;229:869–876
- Sahani D, Rastogi N, Greenfield A, et al. Multidetector row CT in evaluation of 94 living renal donors by readers with varied experience. Radiology. 2005;235:905–910
- Shaffer D, Sahyoun AI, Madras PN, Monaco AP. Two hundred one consecutive living-donor nephrectomies. Arch Surg. 1998;133:426–431
- Rydberg J, Kopecky KK, Tann M, et al. Evaluation of prospective living renal donors for laparoscopic nephrectomy with multisection CT: the marriage of minimally invasive imaging with minimally invasive surgery. RadioGraphics. 2001;21(Spec Issue):S223–S236
- Fishman EK. CT angiography: clinical applications in the abdomen. RadioGraphics. 2001;21:S3–S16
- Laugharne M, Haslam E, Archer L, et al. Multidetector CT angiography in live donor renal transplantation: experience from 156 consecutive cases at a single centre. Transpl Int. 2007;20:156--166
- Schlunt L, Harper J, Broome D, et al. Improved detection of renal vascular anatomy using multidetector CT angiography: is 100% detection possible? J Endourol. 2007;21(1):12–17
- Rubin GD, Alfrey EJ, Dake MD, et al. Assessment of living renal donors with spiral CT. Radiology. 1995;195:457–462
- Pozniak MA, Balison DJ, Lee FT Jr, Tambeaux RH, Uehling DT, Moon TD. CT angiography of potential renal transplant donors. RadioGraphics. 1998;18:565–587
- Kawamoto S, Montgomery R, Lawler LP, Horton KM, Fishman EK. Multidetector CT angiography for preoperative evaluation of living laparoscopic kidney donors. Am J Roentgenol. 2003;180:1633–1638
- Rastogi N, Sahani DV, Blake MA, Ko DC, Mueller PR. Evaluation of living renal donors: accuracy of three-dimensional 16-section CT. Radiology. 2006;240:136–144
- Rubin GD. Helical CT of potential living renal donors: toward a greater understanding. RadioGraphics. 1998;18:601–604
- Kawamoto S, Lawler LP, Fishman EK. Evaluation of the renal venous system on late arterial and venous phase images with MDCT angiography in potential living laparoscopic renal donors. Am J Roentgenol. 2005;184:539–545
- Namasivayam S, Kalra MK, Waldrop SM, Mittal PK, Small WC. Multidetector row CT angiography of living related renal donors: is there a need for venous phase imaging? Eur J Radiol. 2006;59:442–452
- Kawamoto S, Montgomery RA, Lawler LP, Horton KM, Fishman EK. Multi-detector row CT evaluation of living renal donors prior to laparoscopic nephrectomy. RadioGraphics. 2004;24:453–466
- el-Diasty TA, Shokeir AA, el-Ghar ME, Gad HM, Refaie AF, el-Din AB. Contrast enhanced spiral computerized tomography in live kidney donors: a single session for anatomical and functional assessment. J Urol. 2004;171:31–34
- Roh JR, Park CM, Hyun JH, et al. evaluation of living renal transplant donors using helical CT angiography: comparison with conventional angiography. Korean J Urol. 2002;43:43–48
- Pollak R, Prusak BF, Mozes MF. Anatomic abnormalities of cadaver kidneys procured for purposes of transplantation. Am Surg. 1986;52:233–235
- Zamboni GA, Romero JY, Raptopoulos VD. Combined vascular-excretory phase MDCT angiography in the preoperative evaluation of renal donors. Am J Roentgenol. 2010;194(1):145–150
- Lockhart ME, Robbin ML. Renal vascular imaging: ultrasound and other modalities. Ultrasound Q. 2007;23(4):279–292
- Buzzas GR, Shield CF III, Pay NT, Neuman MJ, Smith JL. Use of gadolinium-enhanced, ultrafast, three-dimensional, spoiled gradient-echo magnetic resonance angiography in the preoperative evaluation of living renal allograft donors. Transplantation. 1997;64(12):1734–1737
- Mandal AK, Cohen C, Montgomery RA, Kavoussi LR, Ratner LE. Should the indications for laparoscopic live donor nephrectomy of the right kidney be the same as for the open procedure? Anomalous left renal vasculature is not a contraindication to laparoscopic left donor nephrectomy. Transplantation. 2001;71(5):660–664
- Chai JW, Lee W, Yin YH, et al. CT angiography for living kidney donors: accuracy, cause of misinterpretation and prevalence of variation. Korean J Radiol. 2008;9:333–339
- Zhang J, Zhang X. A discussion on definition of accessory renal artery. Chin J Clin Anat (Chin). 2010;28:109–110
- Zhang J, Zhang X. Vascular anatomy of donor and recipient in living kidney transplantation. Chin J Reparative Reconstr Surg (Chin). 2009;23:1138–1142
- Zhang J, Hu X, Yin X, et al. The role of multi-detector row CT in evaluation of living renal donors. Chin J Organ Transplant (Chin). 2009;30:419–421
- Holden A, Smith A, Dukes P, Pilmore H, Yasutomi M. Assessment of 100 live potential renal donors for laparoscopic nephrectomy with multi-detector row helical CT. Radiology. 2005;237(3):973–980