
Abstract
It is well documented that oxidative stress is involved in the pathogenesis of idiopathic nephrotic syndrome (INS). Malondialdehyde (MDA) is a measurement of lipid oxidation; vitamin C and E are important components of antioxidants. However, the association between MDA, vitamin C or E levels and INS remains elusive. A meta-analysis was performed to investigate the alteration of serum levels of MDA, vitamin C and E in INS compared with controls. Eight studies were included in our meta-analysis according to predefined criteria. Active INS patients demonstrated significantly higher level of serum MDA (SMD: 2.13, 95% CI: 1.511 to 2.749, p < 10−4), markedly lower levels of serum vitamin C (SMD: −1.449, 95% CI: −2.616 to −0.281, p = 0.015) and E (SMD: −1.45, 95% CI: −2.544 to −0.356, p = 0.009) compared with those in controls. Active steroid-sensitive nephrotic syndrome (SSNS) patients showed comparable levels of serum vitamin C and E to those in controls. INS subjects in the remission stage demonstrated significantly higher level of serum MDA (SMD: 1.028, 95% CI: 0.438 to 1.617, p < 10−4), markedly lower level of serum vitamin C (SMD: −2.235, 95% CI: −3.048 to −1.421, p < 104) and similar level of serum vitamin E compared with those in controls. No significant publication bias was observed. In conclusion, the disorder of MDA and vitamin C persists in the remission stage of INS. It seems that the serum levels of vitamin C and E is associated with the responsiveness of INS to steroids. However, more studies should be performed in the future.
Introduction
Idiopathic nephrotic syndrome (INS) is a common glomerular disease affecting both adult and children.Citation1 Most INS patients respond well to steroids, those who respond to steroids therapy with complete remission are defined as steroid-sensitive nephrotic syndrome (SSNS).Citation2 However, a number of INS patients may suffer from frequent relapses or develop dependence on or resistance to steroids in the later stage leading to a protracted course. In contrast to congenital nephrotic syndrome behind which the mechanism is mostly genetic variations, such as nephrin, podcin,Citation3 the precise mechanism of INS remains unclear. For a thorough understanding of INS, it is necessary to explore the underlying cause provided the possibility that it may offer a new therapeutic target or prognostic marker.
Recently, the possible role of oxidative stress in the pathogenesis of INS has been well-documented in in vitro studies.Citation4,Citation5 Oxidative stress is referred to an imbalance between the production and elimination of reactive oxygen species (ROS).Citation6 ROS, by-product of reduction-oxidation reactions, can lead to lipid peroxidation, protein carboxylation, cytoskeletal disruption and DNA damage. The cell injury induced by ROS disrupts the integrity of the tubular epithelial cells and increases glomerular permeability to proteins resulting in nephrotic syndrome.Citation7 Due to the extremely short half life of ROS, such as free radicals, it is not feasible to test it directly. Malonyldialdehyde (MDA), by-product of lipid peroxidation, is often tested to predict the status of ROS indirectly.Citation7,Citation8 Also, the micronutrients including vitamin C and E are non-enzymatic antioxidants that will decline due to the consumption of oxidative stress. In this sense, it is reasonable to hypothesize that the alterations of MDA, vitamin C and E may be associated with INS.
To date, several studiesCitation9–16 have showed the alterations of these parameters in the INS subjects. However, the relative small number of participants limited the statistical power, and some of the results were in conflict. A meta-analysis from individual studies is a good way to better understand this issue; therefore, we performed this investigation to clarify the differences in serum levels of MDA, vitamin C and E between controls and INS subjects in the active or remission stage.
Materials and methods
Search strategy
According to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines,Citation17 an attempt was made to search the published studies that related to oxidant/antioxidant status in INS through May 2013 using PubMed, Embase and Cochrane databases. No restriction was imposed on search language. The used search terms were as follows: (1) oxidant, antioxidant, vitamin, micronutrient, trace element; (2) nephrotic syndrome, idiopathic; and (3) observational, relapse, remission, follow-up. We screened the identified titles and abstracts to select relevant publications. A second screening was based on full-text review. Reference lists of extracted reviews and articles were also examined. If the same subjects were included in more than one paper, we chose the study with the largest number of subjects.
Inclusion criteria
Studies were considered eligible if they met the following criteria: (1) case-control study; (2) case: subjects in the active or remission stage of INS; (3) control: population without renal disease or supplementation of antioxidants; (4) outcome of interest: a minimum of one common parameter (serum level of MDA, vitamin C or E). Studies were excluded if cases suffered from systemic disease or its data was not distributed in Gaussian manner.
Data extraction and quality assessment
We extracted study characteristics for each study. Data were recorded as follows: first author’s last name; year of publication; ethnicity; age at baseline; number of cases and controls; and confounding factors. Any reported mean and standard deviation were also retrieved. In addition, we assessed quality of each study using Newcastle-Ottawa Quality Assessment Scale, which assigned scores for participants’ selection, exposure categories and comparability. Two authors independently conducted the data extraction with any disagreements resolved by discussion.
Statistical analysis
Standard mean deviation (SMD) was used to measure the differences in serum level of MDA, vitamin C or E between INS subjects in the active or remission stage and controls across studies. Heterogeneity of SMDs across studies was tested by using the Q statistic (significance level at p < 0.10). The I2 statistic, a quantitative measure of inconsistency across studies, was also calculated. Either a fixed-effects model or, in the presence of heterogeneity, a random-effects model was used to calculate the pooled SMDs and corresponding 95% confidence intervals (CIs). Sensitivity analysis was performed in childhood, adult and SSNS studies. Potential publication bias was assessed by Begg’s test and Egger’s test at the p < 0.05 level of significance when the number of the studies included was more than 5. All analyses were performed using STATA version 12.0 (Stata Corp, College Station, TX). p < 0.05 was considered statistically significant, except where otherwise specified.
Results
Literature search
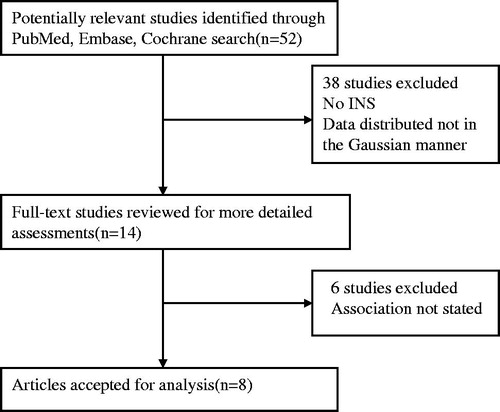
A flow chart showing the study selection is presented in . We initially retrieved 52 relevant studies from the PubMed, Embase and Cochrane databases. Of these, the majority were excluded after the first screening in terms of abstracts or titles, mainly because they were not relevant to INS. After full-text review of 14 articles, sixCitation18–23 studies were excluded because they did not display the status of MDA, vitamin C or E. Finally, eight studies were included.
Figure 1. Flow chart of study selection.
Study characteristics
The characteristics of the eight enrolled studies are presented in . These studies were published between 1997 and 2011. Seven studies were conducted in Asians, and one in Africans. The sizes of studies ranged from 45 to 268. The majority of controls were healthy check-up. Six studies adjusted for confounding factors.
Table 1. Baseline characteristics of studies included in this meta-analysis.
Quality of studies
As shown in , the assigned scores among studies ranged from 5 to 7. None of the studies included belonged to the low quality study (low quality: 1–3, medium quality: 4–6, high quality: 7–9).
Meta-analysis
Active INS patients demonstrated significantly higher levels of serum MDA (eight studies, random effects SMD: 2.13, 95% CI: 1.511 to 2.749, p < 10−4, , ) compared with those in controls, no evidence of publication bias was noted (Begg, p = 0.805; Egger, p = 0.473). Active INS patients demonstrated markedly lower levels of serum vitamin C (four studies, random effects SMD: −1.449, 95% CI: −2.616 to −0.281, p = 0.015, , ) and vitamin E (five studies, random effects SMD: −1.45, 95% CI: −2.544 to −0.356, p = 0.009, , ) compared with those in controls. INS subjects in the remission stage demonstrated significantly higher levels of serum MDA (four studies, random effects SMD: 1.028, 95% CI: 0.438 to 1.617, p = 0.001, ), markedly lower levels of serum vitamin C (one study, fixed effects SMD: −2.235, 95% CI: −3.048 to −1.421, p < 10−4, ) and similar levels of serum vitamin E (two studies, random effects SMD: −0.021, 95% CI: −0.44 to 0.398, p = 0.921, ) compared with those in controls. The results regarding the status of MDA from sensitivity analysis were comparable to those from non-sensitivity analysis, similar findings were observed in the status of vitamin C and E in both childhood and adult INS (). Notably, active SSNS patients showed comparable levels of serum vitamin C and E to those in controls ().
Figure 2. Comparison of serum MDA level between case 1 and control.
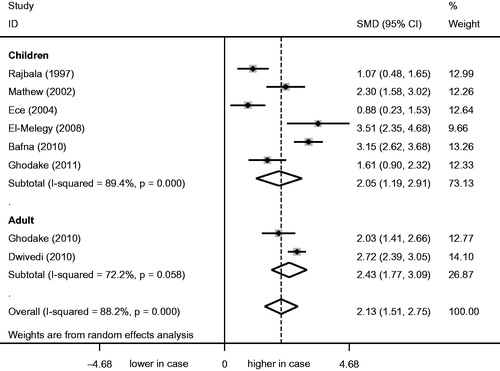
Figure 3. Comparison of serum vitamin C level between case 1 and control.
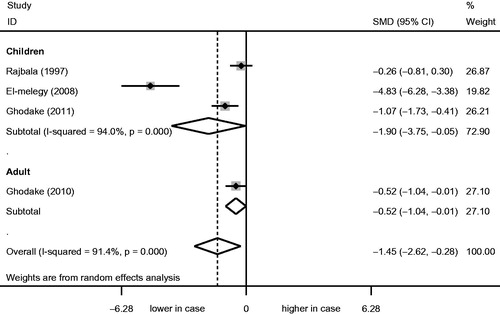
Figure 4. Comparison of serum vitamin E level between case 1 and control.
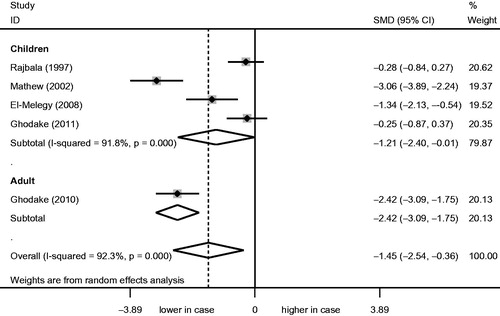
Table 2. Meta-analysis of the association of oxidative stress with INS.
Discussion
To our knowledge, this is the first meta-analysis of the association between oxidative stress and INS. Oxidative stress is involved in the pathogenesis of INS.Citation24 The extremely short half-life of free radicals prompted scientists and doctors to identify other indices to predict the status of oxidant/antioxidant. Due to the fact that MDA is the direct product of lipid peroxidation, MDA is believed to be the optimal marker to reflect the status of oxidative stress. On the other hand, antioxidants including vitamin C and E are usually determined, because they are indispensable for the growth and development of children.Citation25 Our study indicates that the significantly increased level of serum MDA persists in the remission stage of INS. Serum levels of vitamin C and E in INS subjects seem to be associated with the responsiveness to steroids.
Several facts may explain the alterations of MDA, vitamin C and E levels in INS. First, free radicals are possible mediators of injury in nephrosis by enhancing permeability of the glomerular capillary wall,Citation26 meanwhile, dyslipidemia of INS is known to be associated with oxidative stress.Citation12 Hence, MDA, by-product of lipid membranes peroxidation, would increase due to the above-mentioned mechanisms, similar results were observed in the active or remission stage of INS in our study. Second, the antioxidants, such as vitamin C and E, would decline because of the consumption of oxidative stress. Furthermore, the injection of antioxidants in experimental models of INS has been found to be ameliorative,Citation27 which at least indicate that the concentrations of antioxidants in INS are low. Our investigation also suggested that active INS subjects showed significantly decreased levels of vitamin C and E. Finally, active SSNS subjects in our study displayed no marked change of vitamin C and E levels. This is possibly attributable to the fact that the clinical and pathological changes of SSNS are relatively mild, the impact on the gastrointestinal absorption is not severe, and the loss of vitamin C and E may be offset by intake of extra nutrition. Of note, subjects in the remission stage of INS showed markedly decreased levels of vitamin C. This is probably because that the subjects included were frequent relapse of INS, and vitamin C is water-soluble which is more likely to lose compared with vitamin E. Moreover, only one study by El-Melegy et al.Citation12 investigated this issue, which made the results less robust. Further studies should be performed in the future.
Our findings give rise to two questions. First, how long will the status of oxidant/antioxidant normalizes after the induction of INS remission? A study by Mishra et al.Citation28 showed no complete normalization of plasma levels of MDA after 6 months of induction of INS remission. Another study by Kniazewska et al.Citation29 showed complete normalization of serum levels of ferric-reducing antioxidant power and paraoxonase-1 after 4–15 years of induction of INS remission, regrettably, MDA was not tested in this study. Nevertheless, our findings still have important clinical implications that the therapy of antioxidants should be used in both the active and remission stage of INS. Second, how do various clinical or pathological types of INS affect the serum levels of MDA, vitamin C and E? One study by Bakr et al.Citation30 showed that steroid-resistant nephrotic syndrome (SRNS) patients demonstrated significantly higher level of serum MDA than that in SSNS subjects. Our investigation also showed that SSNS subjects demonstrated similar levels of vitamin C and E to those in controls, while all INS subjects displayed decreased concentrations of vitamin C and E. Conversely, another study by Mishra et al.Citation28 showed no differences in the level of serum vitamin C between frequently relapsing INS and infrequently relapsing INS. Nonetheless, our findings indicated that the responsiveness of INS to steroids might affect the serum levels of vitamin C and E.
Our study has obvious strengths: all the studies included had similar baseline characteristics, such as selection of case and control, sample size, methodological testing of parameters. Also, none of the studies included had a low quality in terms of the quality assessment. Yet several limitations should be considered. First, it is not ethical to make a model of INS in human subjects, all the studies included had to be case-control design, which resulted in the unavoidance of reversal causation. Second, substantial heterogeneity was observed across studies. It might affect the results, although a random-effects model was used. Finally, the small number of studies limited the statistical power, further larger number of studies is needed.
Taken together, this meta-analysis suggests that oxidative stress persists in the remission stage of INS. It seems that the responsiveness of INS to steroids is associated with the serum levels of vitamin C and E. Further larger number of studies should be performed.
Declaration of interest
All the authors declared no competing interests.
This study was supported by Grants from the National Basic Research Program of China 973 Program (nos. 2012CB517602 and 2013CB530604), the National Natural Science Foundation of China (nos. 81170635 and 81270785) and the Research and innovation Project for College Graduates of Jiangsu Province, China (grant number CXLX13_556).
Related Research Data
References
- Bagga A, Mantan M. Nephrotic syndrome in children. Indian J Med Res. 2005;122:13–28
- Lombel RM, Gipson DS, Hodson EM. Treatment of steroid-sensitive nephrotic syndrome: new guidelines from KDIGO. Pediatr Nephrol. 2013;28:415–426
- Jalanko H. Congenital nephrotic syndrome. Pediatr Nephrol. 2009;24:2121–2128
- Gwinner W, Landmesser U, Brandes RP, et al. Reactive oxygen species and antioxidant defense in puromycin aminonucleoside glomerulopathy. J Am Soc Nephrol. 1997;8:1722–1731
- Vega-Warner V, Ransom RF, Vincent AM, et al. Induction of antioxidant enzymes in murine podocytes precedes injury by puromycin aminonucleoside. Kidney Int. 2004;66:1881–1889
- Sies H. Role of reactive oxygen species in biological processes. Klin Wochenschr. 1991;69:965–968
- Kamireddy R, Kavuri S, Devi S, et al. Oxidative stress in pediatric nephrotic syndrome. Clin Chim Acta. 2002;325:147–150
- Ghodake SR, Suryakar AN, Ankush RD, et al. Role of reactive oxygen species in pathogenesis of nephrotic syndrome. Ind J Clin Biochem. 2010;25:82–85
- Mathew JL, Kabi BC, Rath B. Anti-oxidant vitamins and steroid responsive nephrotic syndrome in Indian children. J Pediatr. 2002;38:450–454
- Rajbala A, Sane AS, Zope J, et al. Oxidative stress status in children with nephrotic syndrome. Panminerva Med. 1997;39:165–168
- Ece A, Atamer Y, Gürkan F, et al. Anti-oxidant status in relation to lipoproteins, leptin and pro-inflammatory cytokines in children with steroid-sensitive nephrotic syndrome. Nephrology. 2004;9:366–373
- El-Melegy NT, Mohamed NA, Sayed MM. Oxidative modification of low-density lipoprotein in relation to dyslipidemia and oxidant status in children with steroid sensitive nephrotic syndrome. Pediatr Res. 2008;63:404–409
- Bafna A, Sarkar PD. Oxidative stress in primary nephrotic syndrome in relation to dyslipidemia. Int Biol Med Res. 2010;1:144–148
- Ghodake SR, Suryakar AN, Ankush RD, et al. Role of reactive oxygen species in pathogenesis of nephrotic syndrome. Indian J Clin Biochem. 2010;25:82–85
- Dwivedi J, Sarkar PD. Lipoprotein (A), homocysteine, lipid profile with oxidative stress in nephrotic syndrome and cardiovascular nephropathy. Int J Pharma Bio Sci. 2010;1:340–350
- Ghodake SR, Suryakar AN, Ankush RD, et al. Role of free radicals and antioxidant status in childhood nephrotic syndrome. Indian J Nephrol. 2011;21:37–40
- Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010;8:336–341
- Zachwieja J, Bobkowski W, Dobrowolska-Zachwieja A, et al. Decreased antioxidant activity in hypercholesterolemic children with nephrotic syndrome. Med Sci Monit. 2003;9:287–291
- Sinha I, Ghosh S, Dey P, et al. Reduction of urinary thiols in nephrotic syndrome – a possible effect of free iron. Clin Chim Acta. 2005;355:91–96
- Ece A, Atamer Y, Gürkan F, et al. Paraoxonase, total antioxidant response, and peroxide levels in children with steroids-sensitive nephrotic syndrome. Pediatr Nephrol. 2005;20:1279–1284
- Musante L, Bruschi M, Candiano G, et al. Characterization of oxidation end product of plasma albumin ‘in vivo’. Biochem Biophys Res Commun. 2006;349:668–673
- Karthikeyan K, Sinha I, Prabhu K, et al. Plasma protein thiols and total antioxidant power in pediatric nephrotic syndrome. Nephron Clin Pract. 2008;110:10–14
- Zachwieja J, Bobkowski W, Zaniew M, et al. Apoptosis and antioxidant defense in the nephrotic syndrome. Pediatr Nephrol. 2003;18:1116–1121
- Granqvist A, Nilsson UA, Ebefors K, et al. Impaired glomerular and tubular antioxidative defense mechanism in nephrotic syndrome. Am J Physiol Renal Physiol. 2010;299:898–904
- Kurpad AV, Edward BS, Aeberli I. Micronutrient supply and health outcomes in children. Curr Opin Clin Nutr Metab Care. 2013;16:328–338
- Diamond JR, Bonventre JV, Karnovsky MJ. A role for oxygen free radicals in aminonucleoside nephrosis. Kidney Int. 1986;29:478–483
- Ohtake T, Kimura M, Nishimura M, et al. Roles of reactive oxygen species and antioxidant enzymes in murine daunomycin-induced nephropathy. J Laboratory Clin Med. 1997;129:81–88
- Mishra OP, Gupta AK, Prasad R, et al. Antioxidant status of children with idiopathic nephrotic syndrome. Pediatr Nephrol. 2011;26:251–256
- Kniazewska MH, Obuchowicz AK, Wielkoszyński T, et al. Evaluation of certain constituents of antioxidant defense in youth treated in the past for steroid-sensitive idiopathic nephrotic syndrome. Pediatr Nephrol. 2009;24:2187–2192
- Bakr A, Abul Hassan S, Shoker M, et al. Oxidant stress in primary nephrotic syndrome: does it modulate the response to corticosteroids? Pediatr Nephrol. 2009;24:2375–2380